







A practical approach for primary care on the interpretation of kidney function in older adults
Case report
An 82-year-old woman with hypertension is found to have an eGFR of 48 mL/min/1.73m² on routine blood testing. She is independent, but mildly frail. Repeat testing over three years shows stable kidney function, with no albuminuria or symptoms.
In this scenario, the label of chronic kidney disease adds little clinical value. Management should focus on blood pressure control, medication review, and maintaining independence rather than referral or escalation.
Chronic kidney disease (CKD) is one of the most frequently encountered abnormalities in routine blood testing in general practice. In Ireland, approximately one in 10 adults has CKD, rising to around one in seven among those aged over 50 years. Despite this high prevalence, its clinical significance in older adults is often unclear.
For GPs, the challenge is not detection, but interpretation. A large proportion of older patients labelled with CKD stage 3 have stable kidney function that will not progress or require intervention. However, the diagnosis often triggers repeated monitoring, referrals, and patient anxiety. This raises a fundamental clinical question: When does CKD matter in older adults?
CKD in Ireland: Common, but often misinterpreted
CKD is both common and frequently under-recognised in Ireland, particularly in primary care. However, the increasing detection of CKD has not necessarily translated into improved patient outcomes. Much of what is identified represents mild reductions in kidney function, often discovered incidentally during routine monitoring for other conditions, such as hypertension or diabetes.
This distinction is important. A high prevalence of CKD does not automatically imply a high burden of clinically significant disease. In many cases, reduced eGFR reflects age-related physiological change rather than progressive renal pathology.
Renal ageing: Physiology versus disease
Ageing is associated with structural and functional changes in the kidney, including reductions in cortical mass, glomerulosclerosis, and declining renal blood flow. These changes contribute to a gradual reduction in glomerular filtration rate, typically in the order of 1 mL/min per year after midlife.
As a result, many older adults have an eGFR between 45 and 60mL/min/1.73m² without symptoms, albuminuria, or evidence of progression. Importantly, the majority of these individuals will never develop end-stage kidney disease.In fact, competing risks such as cardiovascular disease and frailty are far more likely to determine outcomes.
Despite this, current diagnostic frameworks classify these patients as having CKD. This raises concerns regarding overdiagnosis and the potential for unnecessary intervention.
The problem of overdiagnosis
The use of fixed eGFR thresholds to define CKD does not adequately account for age-related physiological decline. Consequently, a large proportion of older adults are labelled with CKD based on laboratory values alone.
In clinical practice, this often leads to a cascade of follow-up testing, increased surveillance, and referral, even in patients who are unlikely to benefit from such interventions. It can also contribute to patient anxiety, particularly when the implications of the diagnosis are not clearly explained.
Overdiagnosis is not a benign phenomenon. It consumes healthcare resources and risks shifting attention away from more meaningful aspects of care, such as functional status, symptom control, and overall wellbeing.
Assessing clinical significance in practice
In primary care, the interpretation of CKD should move beyond a single eGFR value and instead focus on trajectory and context. A stable eGFR over time is often reassuring, whereas a consistent downward trend warrants closer attention.
The presence of albuminuria remains an important marker of renal risk and should be assessed alongside eGFR. Similarly, recurrent episodes of acute kidney injury, resistant hypertension, or symptoms suggestive of fluid overload or uraemia may indicate more significant disease.
In contrast, an older patient with stable kidney function, no albuminuria, and no symptoms is unlikely to benefit from aggressive investigation or referral. In such cases, CKD may be better understood as a marker of ageing rather than a target for intervention.
Frailty: A more important predictor than eGFR
Frailty is a central determinant of outcomes in older adults and has relevance in the context of CKD. Patients with reduced physiological reserve are more vulnerable to adverse events, including hospitalisation, functional decline, and mortality.
Evidence consistently demonstrates that frailty is a stronger predictor of outcome than kidney function alone. This has important implications for clinical decision-making. A frail patient with mild CKD may have a poorer prognosis than a fitter individual with more advanced renal impairment.
Multimorbidity further complicates the picture. CKD rarely occurs in isolation and is commonly associated with cardiovascular disease, diabetes, and cognitive impairment. These conditions often exert a greater influence on outcomes than renal function itself.
Medication risk and polypharmacy
Medication-related harm is a significant and often modifiable contributor to adverse outcomes in older adults with CKD. Reduced renal clearance can lead to drug accumulation, while polypharmacy increases the risk of interactions and side-effects.
In primary care, careful attention should be paid to medications that may exacerbate renal dysfunction or increase the risk of acute kidney injury. Non-steroidal anti-inflammatory drugs (NSAIDs) are a common culprit and should generally be avoided. Renin–angiotensin system inhibitors require monitoring, particularly during episodes of acute illness, when temporary discontinuation may be appropriate.
Diuretics, while often necessary, can contribute to dehydration and electrolyte imbalance, particularly in frail patients. Sedative medications and opioids may further increase the risk of falls and cognitive impairment.
Regular medication review, with an emphasis on deprescribing where appropriate, is a cornerstone of safe CKD management.
Acute kidney injury: Prevention and early recognition
Acute kidney injury represents a critical event in the trajectory of many older patients with CKD. It is associated with increased mortality, accelerated decline in renal function, and loss of independence.
Older adults are particularly susceptible due to reduced physiological reserve and the cumulative effects of comorbidities and medications. Episodes of AKI are often precipitated by relatively minor stressors, such as infection or dehydration.
Primary care has a key role in prevention. This includes early recognition of illness, adjustment of medications during periods of physiological stress, and patient education regarding ‘sick day rules’. Maintaining adequate hydration and avoiding nephrotoxic agents where possible are also important.
Referral and dialysis: Rethinking thresholds
Decisions regarding referral to nephrology should be guided by clinical context rather than eGFR alone. Patients with progressive decline in renal function, significant proteinuria, or diagnostic uncertainty are likely to benefit from specialist input.
However, routine referral of stable older patients with mild CKD is often unnecessary and may not improve outcomes.
The question of dialysis is particularly complex in older adults. While dialysis can prolong life in selected patients, the benefits are less clear in those who are frail or have significant comorbidity. Treatment burden is high and quality of life may be adversely affected.
For many patients, conservative management focused on symptom control and quality-of-life represents a more appropriate approach. These discussions are often initiated in primary care and should be informed by patient values and preferences.
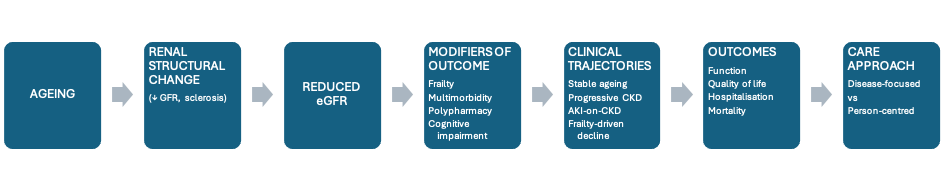
Conceptual model of geriatric CKD
Figure 1 illustrates the interaction between age-related renal decline and geriatric syndromes in determining clinical outcomes. Reduced eGFR should be interpreted within a broader framework incorporating frailty, multimorbidity, cognitive function, and patient goals. Clinical trajectories vary and outcomes are often driven more by geriatric syndromes than renal function alone.
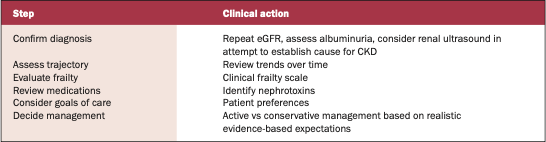
A practical approach for primary care
A structured approach can help guide decision-making in everyday practice. Confirming the diagnosis with repeat testing and assessing for albuminuria are essential first steps. Reviewing trends over time provides insight into whether kidney function is stable or declining.
Assessment of frailty and comorbidity helps to contextualise risk, while medication review identifies opportunities to reduce harm. Importantly, discussions regarding goals of care should be incorporated early, particularly in older patients with complex health needs.
This approach shifts the focus from disease labelling to clinical relevance.
Future directions in Ireland
Key points:
▶ CKD is common in older adults, but often overdiagnosed;
▶ Reduced eGFR alone does not indicate clinically-significant disease;
▶ Stable CKD stage 3a without albuminuria is usually low risk;
▶ Frailty and comorbidity are stronger predictors of outcome than kidney function;
▶ Medication review is a key intervention in primary care;
▶ Acute kidney injury is a major driver of decline and is often preventable;
▶ Referral should be guided by progression, proteinuria, and clinical context;
▶ Dialysis may not improve outcomes in frail older adults;
▶ Management should prioritise function, independence, and patient goals;
▶ In older adults, trajectory matters more than a single eGFR value.
Conclusion
CKD in older adults is common, but frequently overinterpreted. Reduced kidney function alone does not necessarily indicate clinically meaningful disease.
For GPs, the priority is to distinguish between patients who require active management and those in whom CKD represents physiological ageing.
A shift is required from disease-based thresholds to clinically relevant decision-making. Trajectory, frailty, symptoms, and patient priorities should guide care.
A simple principle may be helpful in practice: In older adults, stable kidney function matters less than how the patient is functioning overall.
References on request
Correspondence:
Dr Ikhwan Marion
Tel: 01 293 8669
Email: drmarionoffice@beaconhospital.ie











Leave a Reply
You must be logged in to post a comment.