NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Mark Emanuel Debono and Dr Francesca Briffa
- 09th Sep 2024
Diabetic retinopathy (DR) is the commonest microvascular complication of diabetes mellitus (DM). The retina is vulnerable to microvascular damage in DM as a result of its high oxygen and metabolic demands, as well as its dependence on an intact blood-retinal barrier (BRB). All diabetic individuals will be at risk of developing DR. DM causes multiple physiological and metabolic changes in the retina, and it has been suggested that retinopathy starts to develop approximately seven years before the clinical diagnosis of type 2 DM is made. DR is considered to be a leading cause of vision loss in working-age populations globally, notably in middle- and high-income countries, and it imposes a substantial economic burden on healthcare systems. Vision impairment resulting from this condition also creates a burden on patients’ quality-of-life.
Epidemiology
The global prevalence of DM is predicted to increase substantially in the coming decades, with a predicted estimation of 592 million affected individuals by 2035 compared to 382 million in 2013. As the global prevalence of DM increases, so will the number of individuals with DR. The World Health Organisation has estimated that DR is responsible for approximately 15-to-17 per cent of total blindness in Europe and the US alone. From a worldwide perspective, DR is an even larger issue, with an estimated prevalence of 35 per cent. The global prevalence for sight-threatening stages, typically proliferative DR (PDR) and diabetic macular oedema (DMO), is estimated to be 7 per cent. DR is the most common cause of blindness in working age individuals’ in Ireland, at the present time. It is estimated that there are approximately 190,000 people in Ireland with diabetes and 10 per cent of them are at risk of sight-threatening retinopathy (HSE).
Risk factors
Poor glycaemic control, duration, and severity of DM and hypertension: These are the most relevant causative risk factors related to DR, however, control of blood glucose has been noted to have a greater impact than blood pressure control when it comes to the risk of development of DR.
Age: In younger onset DM, DR is unusual before 13 years of age, whilst in those with older-onset DM, there is an increased frequency of DR in patients less than 50 years of age.
Gender: Women not only have twice the overall risk of blindness, but are also more likely than the male sex to have DM.
Ethnicity: Moderate and more severe retinopathy is commoner in Polynesians than Europeans. Studies have also demonstrated other ethnic differences, with higher levels of DR in Hispanics (36 per cent) followed by African Americans (29 per cent), and non-Hispanic white individuals (22 per cent).
Smoking: Is a potential risk factor for the development of DR in type 1 DM. However, when it comes to type 2 DM, evidence is controversial, and smoking in these individuals has been suggested to serve as protection against the progression of retinopathy in a certain number of patients, despite the fact that smoking is in itself an independent risk factor for cardiovascular disease and death in patients with diabetes.
Genetics and family history: Various twin studies have also classified DR as a genetically inherited polygenic disorder with a recognisable familial clustering, also leading to a family history of DR being a risk factor.
Others: Include anaemia, dyslipidaemia, a high BMI, puberty, pregnancy, nephropathy, cataract surgery, DR in the other eye, and vitamin D deficiency.
Classification/staging
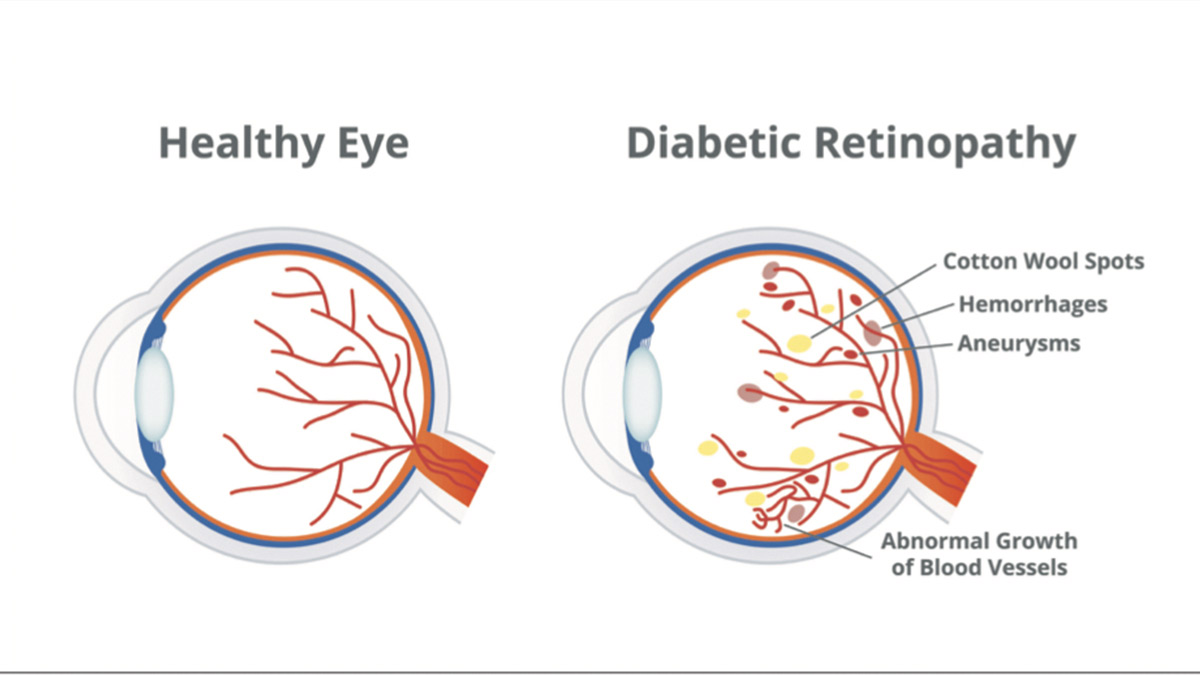
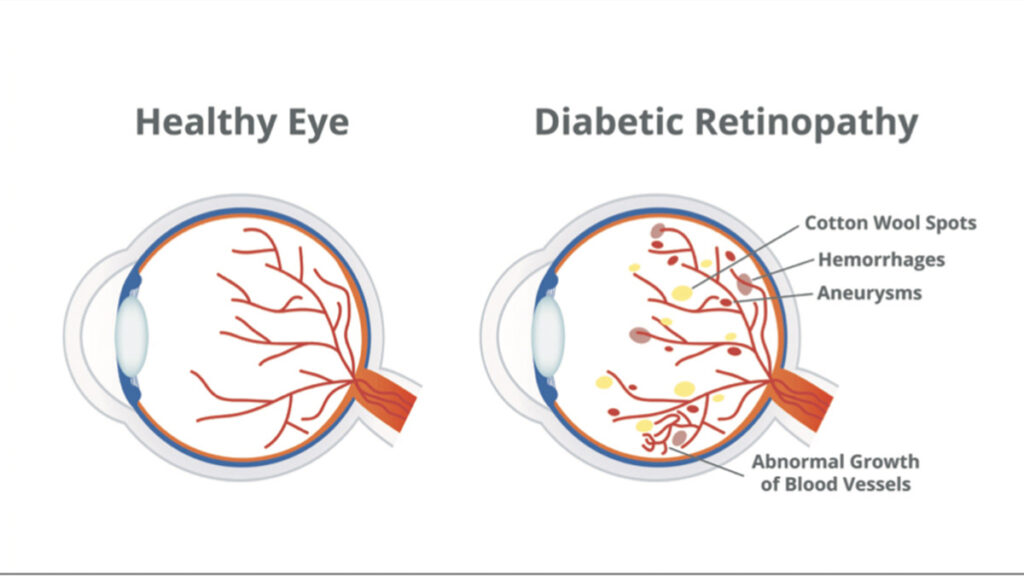
The clinically visible lesions seen in DR are predominantly vascular in nature and, in view of this, DR has been regarded as a vascular disorder for a number of years. According to the International Clinical Disease Severity Scale, a modified classification originating from the Airlie House Classification, DR is classified according to the presence of microvascular lesions in the retina. There is the non-proliferative stage, which is characterised by retinal haemorrhages, microaneurysms, vascular tortuosity, and lipid exudates, that can be further classified into mild, moderate, and severe; and the proliferative stage, during which there is the formation of new pre-retinal abnormal vessels.
An additional category of DR is DMO, which is characterised by fluid accumulation in the neural retina leading to aberrant retinal thickening and subsequent cystoid macular oedema. DMO can be subdivided into mild, moderate, and severe, and can occur across all severities of DR, both in non-proliferative diabetic retinopathy (NPDR) and PDR. It has been named as the commonest culprit of vision loss in patient with DR.
Presentation
DR is considered to be unusual among retinal diseases due to the fact that symptomatology may vary drastically and may be out of proportion to the severity of pathology within the retina. Patients with NPDR are usually asymptomatic. However, if PDR develops, the patient could present with a sudden vision loss owing to vitreous haemorrhage. In cases of development of DMO, the patient might notice a more gradual loss of vision.
Figure 1: Healthy eye versus eye with diabetic retinopathy
Pathophysiology
In DR, hyperglycaemia plays a crucial role in its pathogenesis. The elevated blood glucose levels lead to activation of a variety of pathways including:
Polyol mechanism: In high glucose levels, through the enzymatic activity of aldolase reductase, sorbitol is produced from glucose with the cofactor nicotinamide adenine dinucleotide phosphate (NADPH). In turn, sorbitol is converted to fructose by sorbitol dehydrogenase. Sorbitol, in view of its hydrophilic properties, causes damage to the retinal cells via intracellular osmotic imbalance. In addition, fructose is metabolised to 3-deoxyglucosone and fructose-3-phosphate which lead to oxidative stress in the retinal cells, including pericytes via the promotion of advanced glycation end products (AGE).
Accumulation of AGE: AGE leads to an increase in reactive oxygen species (ROS), leading to damage of the retinal cells and also to reduced mRNA levels of pigment epithelium-derived factor (PEDF). PEDF has a protective role, therefore, reduced levels of PEDF lead to increased inflammation and damage to the microvascular endothelial cells of the retina. Simultaneously, the enzyme complex NADPH oxidase and nuclear factor-B (NF-κB) are activated, leading to inflammation and cellular damage. Tumour necrosis factor-α (TNF-α), interleukin (IL)-1β, lipoprotein-PLA2, and other biomolecules are all involved in the inflammation caused in the vessels.
PKC activation: Elevated blood glucose levels lead to activation and stimulation of protein kinase C (PKC)-δ signalling, leading to expression of PKC and p38 mitogen-activated protein kinase, as well as dephosphorylation of PDGF receptors. This in turn leads to a decrease in the signalling of PDGF receptors, leading to death of the cells of the pericytes.
Oxidative stress: Elevated glucose levels leads to increased intracellular NADL levels and elevated lactate levels in the tissue. This leads to an influx of excessive electrons into the mitochondria, leading to the formation of ROS causing retinal oxidative stress. This process alters DNA metabolism that in turn augments the nuclear enzyme PARP (poly-adenosine diphosphate-ribose polymerase) and enhances the activation of NF-κB. This process leads to further formation of TNF-α and NF-κB-dependent genes that lead to further oxidative stress.
Pericytes enwrap the microvasculature and support endothelial cells. All of the above-mentioned mechanisms lead to oxidative stress, which in turn leads to loss of pericytes in the early stages of DR. Loss of pericytes and subsequently, endothelial cells, leads to capillary occlusion, which in turn results in retinal ischaemic conditions along with cotton wool patches, microaneurysms, and dot-and-blot haemorrhages. This is accompanied by basement membrane (BM) thickening in the early stages of DR. In view of the oxidative stress caused by these processes, the BRB breaks down. Dysfunction of the BRB leads to thickening of the retina and increased leukocytosis, which is an intravascular immune response.
Retinal ischaemia leads to an increase in VEGF levels, with the latter playing a critical role in restoring blood supply to the ischaemic retina. This process is referred to as neovascularisation and it damages the retina more severely, possibly even causing retinal detachment. This process of neovascularisation leads to the formation of delicate and permeable blood vessels that lead to vitreous haemorrhages. Such haemorrhages lead to the formation of fibrovascular scars and gliosis. Studies have shown that upregulation of VEGF is mediated by hypoxia-inducible factors (HIFs). Genes regulated by HIFs, including stromal-derived growth factor-1 (SDF-1) and platelet-derived growth factor-B (PDGF-B), play important roles in this retinal neovascularisation. It is, therefore, no surprise that regulation of VEGF and HIFs is being targeted for the treatment of DR.
Apart from neovascularisation, neurodegeneration also plays an important role towards the end-stage of DR. Neurodegeneration occurs in view of the reduced signalling and activation of neurotrophic factors, including NGF (nerve growth factor), PEDF, IRBP (interphotoreceptor retinoid-binding protein), and somatostatin.
The previously mentioned mechanisms also lead to retinal inflammation and retinal degeneration, which are features that can be detected from the early stages to the more chronic stages of DR. Glutamate excitotoxicity and loss of neuroprotective molecules further contribute to retinal neuronal cell death. Lipid dysregulation also plays a role in the development of DR, with studies showing a strong association between changes in the plasma levels of high-density and low-density lipoproteins (HDL and LDL) and development and severity of DR as well as diabetes. New research has in fact demonstrated that lipid-modifying drugs could have protective effects in DR.
More recent studies have been carried out examining the vitreous humour of PDR patients. Barba et al (2010) showed that lactate levels increased whilst ascorbic acid levels decreased in PDR patients compared to control patients. Paris et al (2015) showed that there is upregulation of arginine and proline levels in PDR patients, while Haines et al (2018) demonstrated that pyruvate levels increased and purine related pathways were activated in PDR patients.
Diagnosis
The primary method for evaluation of DR involves direct and indirect ophthalmoscopy. However, a vast range of imaging modalities are available to aid the clinician when it comes to examining the retina. These imaging methods include the following, amongst others:
Fundus photography: Enables detection of microaneurysms, intraretinal haemorrhages, cotton-wool spot, venous beading, intraretinal microvascular abnormalities, and neovascularisation of optic disc or elsewhere. Throughout the years, it has been the gold standard for evaluating DR.
Fluorescein angiography (FA): Able to detect microaneurysms, retinal capillary non-perfusion, vascular telangiectasia, capillary drop-outs, enlargement or irregularity of the foveal avascular zone, and the presence of neovascularisation.
Optical coherence tomography (OCT): Clinical findings include retinal thickness, subfoveal choroidal thickness, photoreceptor outer segment, hard exudates, intraretinal cystoid spaces, bridging retinal processes, and hyperreflective retinal and choroidal foci, amongst others.
Ultra-wide field (UWF) retinal imaging: Clinical findings include microaneurysms, intraretinal haemorrhages, cotton-wool spot, venous beading, preretinal and vitreous haemorrhages, neovascularisation of optic disc or elsewhere, and intraretinal microvascular abnormalities.
Biomarkers of disease Biomarkers related to glycation and oxidative stress
Serum N-epsilon-carboxy methyl lysine (CML) and pentosidine (AGEs) are increased in DR, as are asymmetric dimethylarginine (ADMA), symmetric dimethylarginine (SDMA), and I-arginine.
Elevated Apo-A1 levels (a component of HDL protein) and low Apo-B levels (component of LDL) are protective factors of DR.
A serum level of Apo-A1 ≥7.4umol/L is associated with reduced risk of DR.
In Ireland, the Diabetic RetinaScreen Programme offers annual screening to patients over 12 years with DM free of charge
Biomarkers related to inflammation and endothelial dysfunction
Higher levels of CRP, IL-1β, IL-8, and TNF-α are associated with DR.
Levels of intercellular adhesion molecule-1 (ICAM1) and vascular adhesion molecule-1 (VCAM1) rise as DR progresses.
Hyperhomocysteinaemia is associated with greater risk of developing DR.
High levels of adiponectin (anti-inflammatory role) is associated with improved retinal microcirculation.
Biomarkers of BM thickening
Elevated urinary and serum levels of collagen type IV is associated with DR, as are metalloproteinases (MMP) – MMP-9 in T1DM, and MMP-2 and MMP- 9 in T2DM.
Biomarkers of angiogenesis and thrombosis
VEGF levels with over 90 per cent specificity and sensitivity in predicting the presence of DR.
Serum erythropoietin (EPO) is associated with DR, with highest levels found in PDR and lowest levels in patients without DR (Davidović et al, 2019).
Fibroblast growth factor-21 (FGF-21) concentration is increased in DR, as is serum HIF-1α.
Elevated levels of TGF-β are strongly associated with the incidence of DR
Reduced PEDF levels have been found in diabetics with retinopathy.
Research has shown that diabetics with levels of vitamin D below 30nmol/L had a 60 per cent greater chance of developing PDR compared to those with vitamin D levels above 75nmol/L.
Novel biomarkers
mRNA encoding retina-specific pigment-protein rhodopsin (RHO) rises with progression of DR.
Reduced circulating mRNA for retinal amine oxidase (RAO) and an elevation in RHO/RAO mRNA ratio as DR progresses.
Increased levels of circulating retinal pigment epithelium-65 (RPE65) mRNA and reduced retinoschisin mRNA as DR worsens.
Management
The principles of management of DR can be generally divided into prevention, early detection, and ophthalmological treatments. Luckily, much of the visual loss from DR can be prevented, and the rates of loss of vision from diabetes and DR have substantially decreased over the past few years. The risk of developing DR can be diminished by early detection of disease by means of screening, as well as tight control of blood glucose, blood pressure, and lipids.
Due to the impact of DR on individuals with DM, screening for DR is of utmost importance to detect preventable blindness as early as possible. Studies have shown that the clinical outcome of patients with DR is better if these individuals are screened and treated as early as possible. Many different methods are available for screening DR, such as direct ophthalmoscopy, dilated stereoscopic fundoscopy, fundus analogue photography, and the use of digital photography with wide-angle imaging, amongst others. It has been recommended that adults with type 1 DM should undergo an initial dilated and comprehensive examination of the eye by an ophthalmologist within the first five years of the onset of DM, while adults with type 2 DM should undergo this examination at the time of diagnosis of DM. If DR is not evident for one or more annual eye examinations, then examination every two years may be considered. However, if there is evidence of DR, consecutive dilated retinal examinations should be repeated at least annually for both type 1 and 2 DM patients.
Patients with any level of macular oedema, severe NPDR, or any PDR should be urgently referred to an ophthalmologist.
Laser photocoagulation therapy is one of the treatments used in DR and it has been proven to diminish the risk of loss of vision in patients with high-risk PDR and in some instances, severe NPDR. Intravitreous injections of an anti-VEGF agent are indicated in cases in which there is central DMO as this occurs below the foveal centre and may threaten reading vision. Intravitreal corticosteroids are also successful in patients with persistent DMO and loss of vision after the failure of conventional treatment, that is, laser photocoagulation therapy and risk factor modification. Vitrectomy has a prominent role in the management of retinal traction detachment (RTD) associated with severe fibrovascular proliferations in cases of PDR.
DR as a predictor of other diabetic complications
The presence of DR indicates that there has already been damage to the microcirculation by the diabetic background and hence, it can be considered to be a reliable biomarker of the destructive effects of DM in a certain individual. DR has been associated with two kinds of neuropathies – cardiac autonomic neuropathy and diabetic peripheral neuropathy. With DR, there is also an increase in the possibility of developing nephropathy and it is considered to be an independent and significant predictor of progression to macro- and micro- albuminuria along with a decline in the glomerular filtration rate in these individuals. There has also been a link between DR and the development of cognitive impairment and dementia. Apart from the aforementioned microvascular complications, individuals with DR are also prone to developing macrovascular complications including cardiovascular, cerebrovascular, and peripheral complications.
Diabetic RetinaScreen
In Ireland, the Diabetic RetinaScreen Programme offers annual screening to patients over 12 years with DM free of charge. Screening is carried out through a network of over 130 community-based screening locations. The programme, now over 10 years old, screens over 110,000 people each year, and refers over 7,000 people to one of its treatment clinics for further tests or treatment.
A 2023 national survey for Diabetic RetinaScreen found that just under one-in-four people who have diabetes, or have a spouse or child with diabetes, report that they know very little or nothing about DR. The HSE is keen to raise awareness of DR and the importance of screening. It recently launched a new Diabetic RetinaScreen e-learning module to increase knowledge about screening so that health and social care staff can support eligible patients to take part in the screening programme. The module takes around 15 minutes to complete. To access the module, log on to HSeLanD using your credentials and search for ‘Diabetic RetinaScreen’.
A GP can verify their patient’s diagnosis is on the Diabetic RetinaScreen register and can add newly diagnosed people with diabetes by calling Freephone 1800 45 45 55 (choose option 4) or online at www.diabeticretinascreen.ie.
Conclusion
DR is a burdensome and challenging disorder that requires prompt diagnosis and management. Early screening and detection are paramount in reducing vision loss for this patient group, while prevention offers the best outcomes.











Leave a Reply
You must be logged in to post a comment.