Reference: April 2025 | Issue 4 | Vol 11 | Page 32
Lung cancer is the third most common cancer in Ireland, with almost 2,600 people diagnosed each year, and is the leading cause of cancer death amongst both sexes, accounting for one in five of all cancer deaths between 2020-2022. Most people diagnosed with lung cancer are over the age of 65 years and many have a history of smoking.
Non small cell lung cancer (NSCLC) accounts for 80 per cent of primary lung cancer cases, while small cell lung cancer (SCLC) accounts for the remainder. Accurate staging is crucial for prognostic assessment and treatment decisions in patients with lung cancer.
With the advent of immunotherapy and targeted therapies, the lung cancer treatment paradigm is shifting, and the importance of accurate staging in lung cancer remains paramount. This article seeks to outline the recent changes in the new 9th edition of the tumour-node-metastasis (TNM) staging system, addressing what potential impact it may have on future management and what the 10th edition of the staging system may hold.1
The purpose of the TNM classification is to facilitate a consistent nomenclature for the anatomical extent of a tumour, to standardise healthcare professionals’ communication on outcomes, and applicability of data to individual patient outcomes. The TNM classification system for lung cancer applies to both NSCLC as well as to neuroendocrine neoplasms ranging from typical carcinoids to SCLC. It does not apply to other rarer forms of pulmonary neoplasms such as pulmonary sarcomas or lymphoma.
Accurate staging of lung cancer to determine the extent of disease is essential due to its impact on treatment options and overall prognosis.2,3 The types of staging in patients with NSCLC include clinical staging, surgical-pathological staging, and re-staging for recurrent disease or following neoadjuvant treatment. The clinical or diagnostic stage (which is assigned the prefix ‘c’) is informed by all radiological, pathological, and laboratory investigations completed prior to a definitive treatment decision including surgical resection.4
The accuracy of clinical staging is dependent on the intensity of the pre-operative assessment and, as a result, an insufficiently investigated patient may be inaccurately under- or over-staged, with direct implications for their treatment. Multi-disciplinary team discussion is critical in ensuring accurate staging and treatment decisions.
The more accurate surgical-pathological stage (which is assigned the prefix ‘p’) is based on clinical stage (cTNM) in addition to histopathological information from the resected tumour and lymph nodes.4 This staging confirms the T descriptor, N descriptor and histological type of lung cancer. It also incorporates information on resection margins, histological grade, and the presence of any lymphovascular invasion.
The 9th edition of the TNM classification for lung cancer came into effect in clinical practice on 1 January 2025. The differences between the 8th and 9th editions are summarised in Table 1.
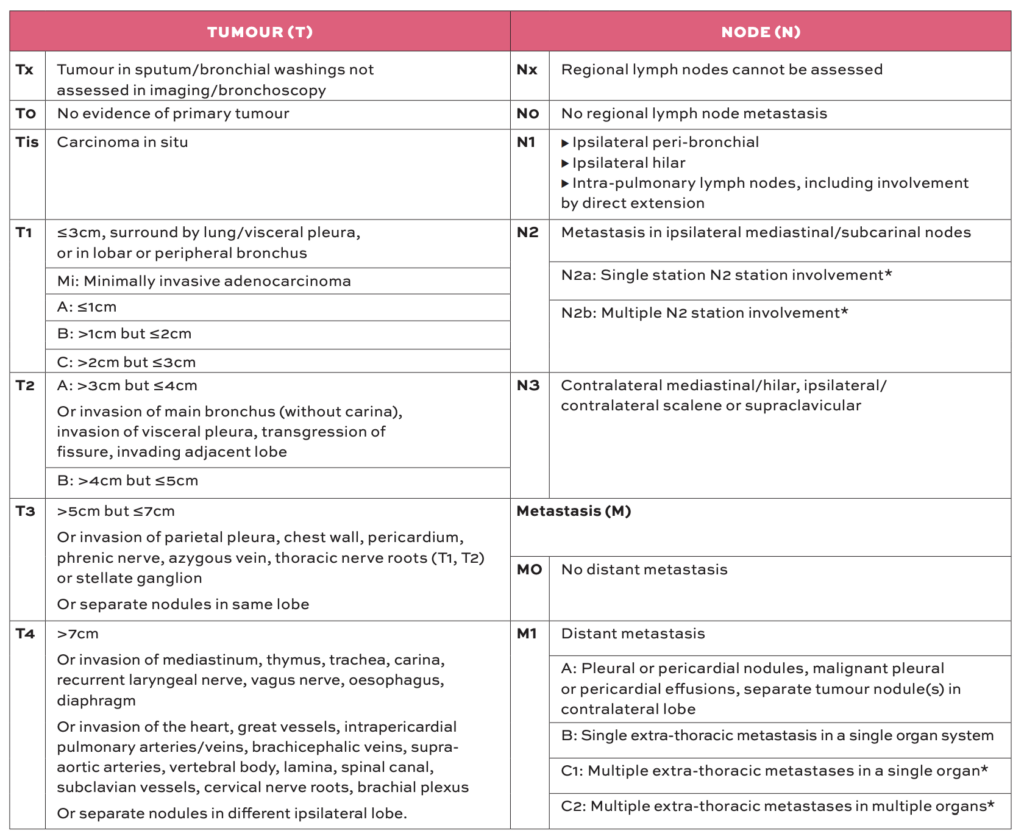
The 9th edition did not offer any changes in T stage when compared to the previous edition. The T stage is determined by the greatest dimension of an invasive tumour based on either pathological or radiological assessment. Tumours ≤3cm that are surrounded by lung/visceral pleura, or in lobar or peripheral bronchi, are designated as T1 (further subdivided by 1cm increments into T1a, T1b, and T1c).
Tumours between 3cm and 5cm, or those invading the main bronchus (but not the carina), invading the visceral pleura, transgressing the fissure, or directly invading an adjacent lobe are designated as T2 (further subdivided by 1cm increments into T2a and T2b). Tumours between 5cm and 7cm, or those that invade parietal pleura, chest wall, pericardium, phrenic nerve, azygous vein, thoracic nerve roots (T1, T2) or stellate ganglion (or separate nodules in the same lobe) are designated as T3.
Tumours >7cm or those that invade into the mediastinum, thymus, trachea, carina, recurrent laryngeal nerve, vagus nerve, oesophagus, diaphragm, heart, great vessels, intrapericardial pulmonary arteries/veins, brachiocephalic veins, supra-aortic arteries, vertebral body, lamina, spinal canal, subclavian vessels, cervical nerve roots, brachial plexus (or separate nodules in a different ipsilateral lobe) are designated as T4.
The N stage is determined by the presence or absence of tumour involvement within regional lymph nodes and is classified using the International Association for the Study of Lung Cancer (IASLC) lymph node classification map.5 Involvement of ipsilateral peri-bronchial, hilar or intra-pulmonary (lymph node stations 10-14) are designated as N1.
Involvement of ipsilateral mediastinal or subcarinal nodes (lymph node stations 1-9) are designated as N2, with the 9th edition of the TNM classification further subdividing this into N2a (single lymph node station involvement) and N2b (multi-lymph node station involvement). N3 disease is defined as contralateral mediastinal/hilar or scalene/supraclavicular involvement.
M staging is based on the presence of metastases, their location and multiplicity. M0 describes no evidence of metastases and M1 defines evidence of distant metastases. This descriptor is further subdivided into M1a (pleural or pericardial nodules/malignant pleural effusion), M1b (single extra-thoracic metastasis in a single organ system), and M1c, which has the additional new descriptors of M1c1 (multiple extra-thoracic metastasis in a single organ) and M1c2 (multiple extra-thoracic metastases in multiple organs).
The introduction of the 9th edition of the TNM classification for lung cancer has coincided with substantial advancements within the domain of lung cancer diagnosis and treatment. Until a few years ago, effective interventions were primarily restricted to surgical resection focused on lower staged tumours predominantly without evidence of N2 disease, whereas chemotherapy and radiotherapy were employed for more advanced disease.
With the advent of neoadjuvant chemo-immunotherapy pathways, treatment options have progressed, with a resultant expansion of options along a multi-modal approach throughout the different stages of disease. This includes the introduction of targeted therapies for earlier stage lung cancers, as well as localised treatments for more advanced stages.6
The re-classification of N2 disease into N2a (single-station involvement) and N2b (multi-station involvement) in addition to subclassifying M1c disease in the 9th edition allows for potential downstaging, which could potentially expand treatment options for affected patients.
T1N1 is now classified as stage IIA (previously IIB). T1N2a is now classified as stage IIB, while T1N2b remains in stage IIIA, T2N2a is now classified as stage IIIA, T2N2b is classified as stage IIIB (previously IIIA), and T3N2a remains in stage IIIA. T3N2b is classified as stage IIIB (unchanged) and both T4N2a and T4N2b remain in stage IIIB. The introduction of subcategories M1c1 and M1c2 does not alter stage (remains stage IVB).
The development and cyclical updates of the TNM staging system continually strive to refine decision making to optimally manage individual lung cancer patients. We know that each centimetre of tumour size as well as extent of metastatic disease directly correlate to survival outcomes and so can enable delineation of the most appropriate treatment pathway.
The 9th edition is the first to include molecular data as well as the inclusion of survival analyses from patients who have undergone induction therapy prior to resection.7 Spread through airspaces has been recommended as an additional descriptor given its association with poorer prognosis, while vascular invasion, lymphatic invasion, and perineural invasion descriptors are also included.
Pending the development of a drug or drugs that can treat any lung cancer irrespective of extent, the TNM classification and its ongoing evolution are critical to optimise treatment decision-making.
The 10th edition seeks to include biomarker/tumour-related data as well as low dose CT data with the overall aim of advancing optimal treatment pathways and standardising care, with improved survival for all lung cancer patients worldwide. Sufficient data volumes and granularity are key components to facilitate that aim.
St James’s Hospital, Dublin, recently announced involvement in the Staging and Prognostic Factors Group of the IASLC. This is the first time surgical patients in Ireland will contribute to the IASLC’s international lung cancer staging project signifying Ireland’s growing role in advancing global cancer care. This contribution will ensure that Irish patients’ characteristics are accounted for in the international effort to refine lung cancer staging and ultimately improve patient outcomes. It also further highlights St James’s Hospital as the national centre for the surgical management of complex thoracic cancer care.
In conclusion, the 9th edition of the TNM classification for lung cancer allows for further refinement and precision in our approach to anatomical staging and has been designed to align with new therapeutic options and multimodal therapies that have shifted the paradigm of lung cancer treatment.
While anatomical characteristics remain crucial for local treatments, non-anatomical tumour factors (such as PD-L1 expression and driver mutations) are becoming increasingly important in guiding systemic therapies. The coming IASLC seven-year cycle will enable further refinement of this system as treatment modalities continue to evolve.
References
- Rami-Porta R, Nishimura KK, Giroux DJ, Members of the IASLC Staging and Prognostic Factors Committee and of the Advisory Boards, and Participating Institutions, et al (2024). The International Association for the Study of Lung Cancer. Lung Cancer Staging Project: Proposals for revision of the TNM stage groups in the forthcoming (9th) edition of the TNM classification for lung cancer. J Thorac Oncol 19:1007-1027.
- National Comprehensive Cancer Network (NCCN). NCCN clinical practice guidelines in oncology: Non small cell lung cancer, V1 2020. [Accessed 9 November 2019.] Available at: www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.
- Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e211S-50S.
- Rami-Porta R, editor. International Association for the Study of Lung Cancer Staging Manual in Thoracic Oncology, 2nd Edn. Editorial Rx Press, North Fort Myers, FL, 2016.
- Rusch V W, et al. The IASCLC Lung Cancer Staging Project: A Proposal for a New International Lymph Node Map in the Forthcoming Seventh Edition of the TNM Classification for Lung Cancer. Journal of Thoracic Oncology: Vol 4, Issue 5, P568-577, May 2009.
- Meyer ML, Peters S, Mok TS, et al (2024). Lung cancer research and treatment: Global perspectives and strategic calls to action. Ann Oncol S0923-7534:04055–04059.
- Rami-Porta R. The TNM classification of lung cancer – a historic perspective. J Thorac Dis 2024; 16 (11): 8053-67.