NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD as a “heterogenous lung condition characterised by chronic respiratory symptoms (dyspnoea, cough, sputum production and/or exacerbations) due to abnormalities of the airways (bronchitis/bronchiolitis) and/or alveoli (emphysema), that cause persistent, often progressive airflow obstruction”.1
Despite COPD being the most prevalent chronic respiratory disease in adults, it is an underdiagnosed condition. This in part relates to the fact the signs and symptoms of COPD often go unnoticed until 30-40 per cent of lung function is lost.2
Historically, COPD was more common in men, however in recent years it has become increasingly prevalent in women, likely due to changes in smoking habits. Studies have suggested that women are more susceptible to developing COPD and more likely to develop severe disease compared to men.3
In Ireland, patients with COPD are now eligible for enrolment in the GP-delivered HSE Chronic Disease Management (CDM) programme, which provides for a dedicated six-monthly review incorporating disease optimisation. According to the latest HSE CDM report, 12 per cent of adults enrolled in the programme have COPD.4
Pathophysiology and risk factors
The hallmark of COPD is chronic airway inflammation, leading to irreversible structural changes, airflow limitation, and impaired gas exchange. These inflammatory and structural changes persist even after smoking cessation. COPD is also associated with systemic inflammation, which contributes to cardiovascular, skeletal, and metabolic comorbidities.5
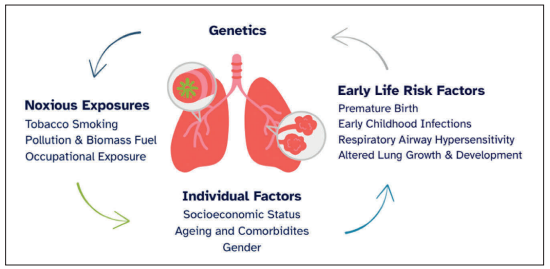
Tobacco smoking is the most significant risk factor for developing COPD; however, up to 25 per cent of individuals with COPD are non-smokers. Several environmental and host factors play a role in the pathogenesis of the disease.
Environmental risk factors include household and air pollution from burning biomass fuels (eg, coal, wood, and crop residues) and heavy exposure to occupational dusts.
The best documented genetic risk factor for COPD is α1-antitrypsin deficiency. It is also increasingly recognised that COPD can result from reduced peak lung function in early adulthood and/or accelerated lung function decline in later life.6
Co-existent asthma
Separating asthma from COPD can be clinically difficult. Typically, the onset of asthma is earlier in life, symptoms are episodic in nature, and airflow obstruction is reversible. However, adults with long-standing asthma may develop fixed airflow obstruction.
The term ‘asthma-COPD overlap syndrome’ (ACOS) was proposed to identify patients who have features of both asthma and COPD, however, this term is controversial and since 2021 GOLD has not recommended its use, instead preferring to delineate COPD and asthma as distinct conditions while recognising that they may share common traits and clinical features.1
FIGURE 1: Risk factors for the development of COPD
Comorbidities
Comorbidity is common in COPD and associated with a poorer prognosis. COPD is an independent risk factor for cardiovascular morbidity and mortality. Even after adjustments for confounding shared risk factors, patients with COPD have a two- to three-fold increased risk of cardiovascular events, including death.
Heart failure is more common in patients with COPD, and comorbid COPD often delays heart failure diagnosis due to overlapping symptoms and shared mechanisms.7
COPD has several extrapulmonary manifestations, including low BMI, malnutrition, and skeletal muscle dysfunction, all of which worsen exercise intolerance. Importantly, muscle dysfunction is a treatable cause of exercise intolerance through pulmonary rehabilitation.
Osteoporosis and related fractures significantly impact morbidity and mortality in COPD. Although corticosteroids are important in managing COPD exacerbations, they are a leading iatrogenic cause of osteoporosis. Physicians should be mindful of this and limit unnecessary steroid use.8
The presence of COPD does not significantly alter the management strategies of common comorbid diseases. However, the diagnosis of comorbid disease in the presence of COPD can be challenging. It is essential that clinicians have a high index of suspicion to ensure early diagnosis and management.
COPD and lung cancer
COPD is an important risk factor for the development of lung cancer, with the greatest risk in patients with emphysema independent of the presence of airflow obstruction or smoking.9
Lung cancers that develop in association with COPD are generally more aggressive and carry a poorer prognosis.10 Two large trials have demonstrated that screening smokers age 50 to 80 years for lung cancer reduces mortality by detecting lung cancer at an earlier stage.11 Screening has not been rolled out nationally in Ireland and is currently in the pilot phase.
Signs and symptoms
The three main symptoms of COPD are chronic cough, dyspnoea, and daily sputum production. Dyspnoea is a cardinal symptom of COPD and highly prevalent across all stages of airflow obstruction. Other symptoms of COPD include wheeze, chest tightness, fatigue, weight loss, and recurrent lower respiratory tract infections.
Although symptoms are often related to the degree of lung function impairment, COPD presents heterogeneously, and even mild airflow obstruction can result in a significant symptom burden.
Symptom scores in COPD are used to assess the severity and impact of symptoms on a patient’s daily life. Common tools include the COPD Assessment test (CAT) and Modified Medical Research Council (mMRC) Dyspnoea Scale.1
Physical exam findings with COPD vary with disease severity. Typical findings in severe disease include signs of hyperinflation, reduced chest expansion, hyperresonance to percussion, wheeze, and a prolonged expiratory phase.
Diagnosis
Spirometry is required to establish a diagnosis of COPD. Spirometry is a non-invasive, cheap, easily reproducible, and readily available test. Current recommendations suggest that adults who report dyspnoea, chronic cough or chronic sputum production should have spirometry performed, particularly if they have a risk factor for COPD.1
The most important values obtained by spirometry are the Forced Vital Capacity (FVC) and the Forced Expiratory Volume in one second (FEV1). Airflow obstruction is defined as a postbronchodilator FEV1/FVC ratio of <0.7.
It is important to note that the use of the fixed FEV1/FVC ratio to define COPD may result in over-diagnosis of COPD in the elderly and under-diagnosis in young adults. The Global Lung Initiative has proposed an alternative approach, which utilises z scores and may better account for age-related changes in the lung.
Spirometry is also used to assess disease severity, based on the decrement of FEV1. Table 1 outlines the GOLD grades and severity of airflow obstruction
GOLD GRADES AND SEVERITY OF AIRFLOW OBSTRUCTION IN COPD
GOLD 1
Mild
FEV1 ≥80% predicted
GOLD 2
Moderate
FEV1 50-80% predicted
GOLD 3
Severe
FEV1 30-50% predicted
GOLD 4
Very Severe
FEV1 <30% predicted
TABLE 1: GOLD stages of airflow obstruction
INVESTIGATION
RATIONALE
Oxygen sats and ABG
If oxygen sats ≤92%, an ABG should be performed to assess for respiratory failure.
FBC to assess blood eosinophils
Eosinophils >300 cells/μL can identify those more likely to respond to inhaled corticosteroids.
Nt-pro BNP
Evaluate for comorbid heart failure or cor pulmonale.
α1-antitrypsin level
All patients with a diagnosis of COPD should be screened at least once for α1-antitrypsin deficiency.
Sputum culture
In patients with frequent exacerbations to guide antimicrobial therapy.
Chest x-ray
Rarely diagnostic, but can rule out other pathologies and complications of COPD, eg, pneumonia.
CT
CT is most sensitive for identifying emphysema. CT is required to assess suitability for lung volume reduction surgery. Consider lung cancer screening with annual low-dose CT in patients 50-80yrs with >20 pack year smoking history.11
TABLE 2: Additional investigations in COPD
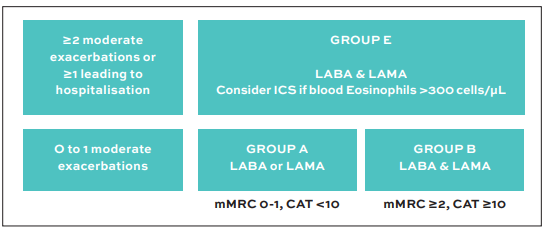
FIGURE 2: Initial bronchodilator treatment in COPD, GOLD (2025)1
In Ireland, GPs can now refer patients directly for spirometry at specialist respiratory integrated care hubs.
ADDITIONAL INVESTIGATIONS
While spirometry is the only test required for a diagnosis of COPD, additional tests may guide treatment and rule out alternative diagnoses. See Table 2 which details the additional investigations that can be considered in those with COPD.
Management
COPD is a complex and heterogenous disease. There is increasing recognition that adopting a more individualised treatment strategy for patients with COPD is beneficial in terms of improving clinical outcomes and minimising side-effects associated with treatments.
Studies have suggested adopting the ‘treatable traits’ strategy, which involves identifying a set of treatable problems specific to the patients and subsequently developing a personalised treatment plan based on the patient’s ‘phenotype’ or ‘endotype’.12
GENERAL MEASURES
1. Vaccinations People with COPD should receive all recommended vaccinations including the yearly influenza and Covid-19 vaccines. The pneumococcal vaccine is recommended every five years up to the age of 65 years and once after 65 years. The US CDC now also recommends RSV vaccination for individuals >60yrs with chronic lung disease.
2. Smoking cessation Of all the interventions available for COPD, smoking cessation has the greatest impact on the progression and prognosis of the disease. Evidence suggests that a combination of counselling and pharmacotherapy is the most effective smoking cessation treatment.
When possible, patients should be referred to a comprehensive smoking cessation programme. Nicotine replacement should be prescribed to all without a contraindication. Other pharmacotherapies available include varenicline and bupropion.
Quit.ie is Ireland’s national smoking cessation website, offering free support, personalised quit plans and access to nicotine replacement therapy.13
3. Pulmonary rehabilitation Pulmonary rehabilitation is a multidisciplinary programme that includes skeletal muscle training, respiratory muscle training, psychological support, and nutritional counselling. Optimal benefits are achieved from a programme lasting six to eight weeks.
Pulmonary rehabilitation has been demonstrated to be the most effective treatment for relieving COPD-related shortness of breath. It also reduces hospitalisations following recent exacerbations and improves symptoms of depression and anxiety.
In Ireland, since the introduction of the integrated care respiratory programme, pulmonary rehabilitation is now available to patients nationwide. COPD Support Ireland also offers free exercise classes to which patients can self-refer or be referred by a healthcare professional.14
Pharmacological therapy
1. BRONCHODILATORS GOLD recommends a tailored approach based on the level of symptoms and risk of exacerbations. GOLD recommends the ‘ABE’ assessment tool that uses an individual’s symptoms (CAT Score or mMRC Dyspnoea Scale) and exacerbation history to guide pharmacotherapy. See Figure 2.
There are two classes of inhaled bronchodilators, β2-agonists and muscarinic antagonists. Long-acting β2-agonists (LABA) and long-acting muscarinic antagonists (LAMA) are superior for controlling symptoms and are recommended first-line in all symptomatic patients.
Poor adherence is common in COPD and is associated with higher mortality and higher admission rates. There are many factors that impact inhaler adherence in COPD, these include inhaler technique, dosing regimens and patient-related factors such as cognitive impairment.15
2. INHALED CORTICOSTEROIDS Studies have demonstrated that blood eosinophils are a potential biomarker to direct inhaled corticosteroids (ICS) treatment and identify patients in whom an ICS will reduce their exacerbation risk. Studies suggest that blood eosinophils <100 cells/µL predicts a poor response to ICS, whereas patients with blood eosinophils >300 cells/µL have the greatest response to ICS.16
There is evidence that the use of ICS results in a small increased risk of pneumonia, as well as higher rates of oral candidiasis, voice change, and skin bruising.17 Currently, guidelines recommend the use of ICS in patients with:
1. A history of exacerbations (≥2 moderate exacerbations or ≥1 leading to hospitalisation) 2. Blood eosinophil count >300 cells/µL 3. Coexistent asthma.
3. BIOLOGICS Monoclonal antibody (biologic) therapies, which modulate specific inflammatory pathways (eg, IL-5, IL-4/IL-13) are emerging as targeted treatments for select patients with COPD, particularly those with eosinophilic inflammation and frequent exacerbations.
4. AZITHROMYCIN Studies have shown that azithromycin (250mg or 500mg three times per week) reduced the risk of exacerbations compared to usual care. Azithromycin can be considered in patients with recurrent exacerbations.
There is a lesser benefit in current smokers and prescribers should be aware of side effects including QT prolongation and hearing loss.18 It is recommended that azithromycin prophylaxis be initiated by a consultant in respiratory medicine and that an ongoing review of azithromycin prophylaxis be carried out every six to 12 months.19
5. THEOPHYLLINE
There is evidence that theophylline, a methylxanthine, has a small bronchodilator effect in COPD, leading to modest improvement in symptoms. However, methylxanthines have several side effects and toxicities, which mean they are not used as first-line agents in COPD.
Non-drug therapies
1. OXYGEN THERAPY AND VENTILATORY SUPPORT Long-term oxygen therapy (worn >15hrs/day) has been shown to improve survival in selected patients with severe resting hypoxaemia (defined as room air PaO2 <7.3kPa or room air PaO2 <8kPa in the presence of other signs of pulmonary hypertension).20
In patients with moderate hypoxaemia or who desaturate with exercise, current evidence suggests that ambulatory oxygen does not improve survival, breathlessness or hospitalisation rates.21 Ambulatory oxygen may be prescribed in patients undergoing rehab or who derive both a symptomatic and functional benefit from its use.
In patients with COPD and persistent stable state hypercapnia, domiciliary non-invasive ventilation has been shown to improve survival, health-related quality of life, exercise tolerance, and exacerbation frequency.22
2. SURGICAL INTERVENTIONS In selected COPD patients with severe emphysema and persistent disabling breathlessness, lung volume reduction procedures can be considered. These include surgical lung volume reduction surgery and the less invasive bronchoscopic placement of endobronchial valves or coils.
3. LUNG TRANSPLANT Patients with COPD should be referred for consideration of lung transplantation when they have progressive disease despite maximal medical therapy. Lung transplantation in those with COPD has been predominantly associated with an improvement in quality of life and not an increase in survival (except in patients with severe α1-antitrypsin deficiency).23
Exacerbations
An exacerbation of COPD is defined as an episode of worsening dyspnoea and/or cough and sputum that deteriorates over two weeks.1
Exacerbations should be considered significant events for patients with COPD as they have a significant negative impact on health status and contribute to disease.
Quach A, Giovannelli J, Chérot-Kornobis N, Ciuchete A, Clément G, Matran R, et al. Prevalence and underdiagnosis of airway obstruction among middle-aged adults in northern France: The ELISABET study 2011-2013. Respir Med. 2015;109(12):1553-61.
Lopez Varela MV, Montes de Oca M, Halbert RJ, Muiño A, Perez-Padilla R, Tálamo C, et al. Sex-related differences in COPD in five Latin American cities: The PLATINO study. Eur Respir J. 2010;36(5):1034-41.
HSE. The third report of the Structured Chronic Disease Management Treatment Programme in general practice. January 2025. Available at: www.hse.ie/eng/services/publications/primary/third-chronic-disease-report.pdf
Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165-85.
Vestbo J, Edwards LD, Scanlon PD, Yates JC, Agusti A, Bakke P, et al. Changes in forced expiratory volume in one second over time in COPD. N Engl J Med. 2011;365(13):1184-92.
Sin DD, Man SF. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality. Proc Am Thorac Soc. 2005;2(1):8-11.
Ogura-Tomomatsu H, Asano K, Tomomatsu K, Miyata J, Ohmori N, Kodama M, et al. Predictors of osteoporosis and vertebral fractures in patients presenting with moderate to severe chronic obstructive lung disease. COPD. 2012;9(4):332-7.
Zulueta JJ, Wisnivesky JP, Henschke CI, Yip R, Farooqi AO, McCauley DI, et al. Emphysema scores predict death from COPD and lung cancer. Chest. 2012;141(5):1216-23.
Cavaillès A, Brinchault-Rabin G, Dixmier A, Goupil F, Gut-Gobert C, Marchand-Adam S, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454-75.
Ru Zhao Y, Xie X, de Koning HJ, Mali WP, Vliegenthart R, Oudkerk M. NELSON lung cancer screening study. Cancer Imaging. 2011;11 Spec No A(1a):S79-84.
van Dijk M, Gan CT, Koster TD, Wijkstra PJ, Slebos DJ, Kerstjens HAM, et al. Treatment of severe stable COPD: The multidimensional approach of treatable traits. ERJ Open Res. 2020;6(3).
HSE. Quit Smoking. [Internet]. Available at: www2.hse.ie/living-well/quit-smoking/
COPD Support Ireland. [Internet]. Available at: www.copd.ie/
Sulaiman I, Cushen B, Greene G, Seheult J, Seow D, Rawat F, et al. Objective assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(10):1333-43.
Bafadhel M, Peterson S, De Blas MA, Calverley PM, Rennard SI, Richter K, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: A post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117-26.
Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;2012(7):Cd002991.
Albert RK, Connett J, Bailey WC, Casaburi R, Cooper JA Jr, Criner GJ, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365(8):689-98.
HSE. Azithromycin prophylaxis in adults with respiratory disease. 2022. Available at: www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/lower-respiratory/azithromycin-prophylaxis-in-adults-with-respiratory-disease/
Ameer F, Carson KV, Usmani ZA, Smith BJ. Ambulatory oxygen for people with chronic obstructive pulmonary disease who are not hypoxaemic at rest. Cochrane Database Syst Rev. 2014;2014(6):Cd000238.
Duiverman ML, Wempe JB, Bladder G, Jansen DF, Kerstjens HA, Zijlstra JG, et al. Nocturnal non-invasive ventilation in addition to rehabilitation in hypercapnic patients with COPD. Thorax. 2008;63(12):1052-7.
Weill D, Benden C, Corris PA, Dark JH, Davis RD, Keshavjee S, et al. A consensus document for the selection of lung transplant candidates: 2014 – an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2015;34(1):1-15.
Ho TW, Tsai YJ, Ruan SY, Huang CT, Lai F, Yu CJ. In-hospital and one-year mortality and their predictors in patients hospitalised for first-ever chronic obstructive pulmonary disease exacerbations: A nationwide population-based study. PLoS One. 2014;9(12):e114866.
Reilev M, Pottegård A, Lykkegaard J, Søndergaard J, Ingebrigtsen TS, Hallas J. Increased risk of major adverse cardiac events following the onset of acute exacerbations of COPD. Respirology. 2019;24(12):1183-90.
NCEC Respiratory ARS, Department of Health. Management of Chronic Obstructive Pulmonary Disease (COPD) National Clinical Guideline No. 27-Summary. 2021. Available at: www.hse.ie/eng/about/who/cspd/ncps/ncpr/copd/resources/management-of-copd-ncec-guideline-no-27.pdf
One study demonstrated that 20 per cent of patients died within one year following their first COPD exacerbation requiring hospitalisation.24
There is also mounting evidence that COPD exacerbations are associated with a period of increased cardiovascular risk, with one study observing a four-fold increased risk of a major adverse cardiac event in the period following an exacerbation.25
The main triggers for exacerbations are respiratory viral infections, although bacterial infections and environmental factors such as air pollution also play a role.
Clinicians can refer to the HSE Clinical Practice Guideline for the Management of COPD.26
Start this Module to earn CPD Points today
Click the "Start Module" button below
Module Title
The latest approaches to diagnosing and managing COPD
Dr Eleanor Cronin, Respiratory Specialist Registrar, Beaumont Hospital, Dublin; and Prof Breda Cushen, Consultant Respiratory Physician, Beaumont Hospital, Dublin and HSE National Clinical Lead for the National Clinical Programme Respiratory (COPD and Asthma)