







Reference: Jan-Feb 2025 | Issue 1 | Vol 18 | Page 49
Sepsis can hide behind any infection. Do not miss the signs
The General Practice Update (GPU) on Adult Sepsis in Primary Care was formally launched in October 2024. This provides a concise, relevant, and summarised document on adult sepsis in primary care which can be accessed online by members through the Irish College of Practitioners College (ICGP) website.1
The GPU aims to promote sepsis awareness in primary care and to promote vaccination as an essential part of sepsis prevention. The document aims to assist GPs in the detection, assessment, and early management of suspected sepsis. It is limited to people 16 years or over who are not or have not recently been pregnant, ie, not in the 42 days after giving birth.
Despite perceived infection being a common reason for presentation in general practice, there was no national guidance on sepsis in primary care prior to this GPU. This article gives a brief synopsis of adult sepsis in primary care, it recognises the importance of the general practice team in creating a sepsis aware environment and its significant role in identifying sepsis at an early stage with prompt referral and management.
Sepsis: A medical emergency
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection.2 Sepsis can be caused by any micro-organism; bacteria, virus, fungus, or parasite.3
Sepsis is a time dependent medical emergency4,5,6,7 which can be difficult to recognise, especially in primary care. Without early detection and urgent management, sepsis can rapidly lead to tissue damage, organ failure, and death. In patients with sepsis, early intensive treatment increases the chance of survival and every hour that treatment is delayed increases mortality with septic shock.
The National Sepsis Report states that in 2023, sepsis and septic shock was documented in 14,535 non-maternity adults in Ireland.8 These patients had a mortality rate of 20.6 per cent and the average length of hospital stay was 22 days.
Who develops sepsis?
Sepsis can affect anyone at any time, but it does occur more commonly in those with risk factors. Recognition of risk factors for developing sepsis is central to any sepsis assessment. These risk factors are cumulative,9
and so, extra caution should be applied to patients who develop deterioration due to infection and
who have one or more risk factors.
The severity and speed of progression of sepsis is affected by the genetic characteristics of the patient, the presence of co-existing illnesses, as well as the number and virulence of the infecting micro-organism.
| CATEGORY | RISK FACTOR |
|---|---|
| Demographic features |
Age >75 years10,11 Frailty11 Socioeconomic deprivation12 Learning disabilities13,14 |
| Co-morbidities |
Diabetes11 Chronic liver, kidney, heart, or lung disease10 Impaired immune function, e.g., malignancy, splenectomy, poorly controlled HIV, bone marrow suppression/failure11 Immunosuppressant medications: Chemotherapy, long-term steroids, biologics, immunomodulator drugs11 |
| Breach of skin integrity |
Recent surgery or invasive procedures in the past six weeks11 Cuts, burns, blisters, or skin infections11 Indwelling lines or catheters11 |
| Others |
Alcohol dependency10 Intravenous drug misuse11 |
TABLE 1: Clinical risk factors that increase the risk of adult sepsis
Sepsis in general practice
General practice is at the frontline of sepsis recognition. Community onset sepsis is acknowledged as a substantial public health problem.15,16,17 The Centres for Disease Control and Prevention (CDC) have identified that 70-80 per cent of cases of sepsis arise in the community.18
The epidemiology of community-based sepsis is however not well understood19 and there is a lack of reliable sepsis incidence and prevalence data from Irish primary care.
The role of general practice in sepsis care is:
- Prevention: Vaccination and infection control;
- Patient education and increasing public awareness of sepsis;
- Early detection and management.
The most effective way to reduce sepsis morbidity and mortality is by prevention. Prevention of microbial transmission and infection is a key step outlined by the World Health Organisation (WHO) to prevent sepsis. Vaccination is crucial, especially in the case of immunocompromised persons who are at increased risk of severe infection. Patient groups include those with HIV infection, acquired asplaenia, and hyposplaenia, those treated with immunosuppressive drugs or radiation, chronic kidney disease (CKD), dialysis and renal transplant patients.20
Endorsement of existing recommendations regarding pneumococcal vaccination,21 Covid vaccination,22 pertussis vaccination in pregnancy,23 and the annual influenza vaccination for both the paediatric and adult population is essential. Influenza is known to be a cause of a significant amount of secondary bacterial infections and could lead to acquiring invasive pneumococcal disease. 80-90 per cent of reported deaths from influenza occur in the elderly, mainly from secondary bacterial pneumonia.24
Optimising vaccination of family members and household contacts to provide indirect protection for those for whom vaccination either does not provide adequate protection or is inappropriate is also a key recommendation in recent vaccination guidelines for immunocompromised patients.20
Infection control measures25 including hand hygiene26 by both healthcare professionals and the public is recommended and plays a key role in preventing infection and sepsis.
Any break in skin integrity, such as a cut, abrasion, burn or a scrape can provide an entry point for microbes to enter the body. Aim to ensure and promote that all wounds be cleaned in a timely fashion, are kept clean as they heal, and are monitored for signs of an infection.
Increased awareness
Increasing public awareness of sepsis, its risk factors, and symptoms is critical to save lives from sepsis. Irish data suggest that there is moderate public awareness about sepsis, but that an understanding of its true impact and associated morbidity and mortality is lacking.27
A HSE sepsis public information campaign including radio ads, social media ads, as well as press and media activity was launched in 2024 to encourage appropriate health-seeking behaviours when someone suspects sepsis. People are encouraged to ask, ‘Could it be sepsis?’
Sepsis information leaflets (Figure 3) were developed in late 2023 and distributed to GPs and pharmacies. These leaflets are available to order for free on www.healthpromotion.ie. Select ‘SEPSIS’ in the ‘Search by topic’ drop-down menu. New posters (Figure 4) are also available for display in waiting rooms to increase sepsis awareness.
Early detection and management are key. We have a unique opportunity in general practice for sepsis detection and early referral, but it is not without its challenges. Sometimes it can feel like we are looking for a needle in a haystack. The key challenge is how to accurately identify the small number of patients who may have sepsis from the numerous innocuous presentations with mild infection. The signs are often mild and non-specific, patients do not always appear unwell or have a temperature and signs are easily overlooked if we don’t actively look for them.
When assessing patients in general practice, where there is limited access to blood tests and diagnostics, the GP team must depend entirely on their clinical skills. There is no single test that confirms the presence of sepsis, the diagnosis of sepsis is based on the presence of a suite of symptoms and signs supported by investigations in secondary care.28
When to suspect sepsis
Patient assessment
History: It is vital to carry out and document a thorough history to identify the focus of infection, rapidity of decline, and potential risk factors for sepsis.
- Past medical history: Identify and document the presence/absence of any risk factors.
- Drug history: Including history of recent chemotherapy or biologic agents.
- Be aware that sepsis may present with vague, common, and non-specific symptoms and patients may not have a fever.11
- Patient deterioration on antibiotic therapy and repeat visits for the same illness should heighten suspicion of sepsis.
- Pay particular attention to concerns expressed by the person and their family or carers.11 Changes may be subtle and not clear to those who have not known the patient previously.
- Consider asking ‘Do you feel that [patient’s name] has been more confused recently?’ This simple question can contribute significantly to detection of altered mental status.29
- For patients in care or nursing homes consider ‘soft signs’30 of potential deterioration, eg, lethargy, withdrawal, agitation, poor appetite, decreased mobility, and reduced fluid intake.
- Assessment of urine output is important – ask the person, family member, or carer how often the person urinated in the past 12-18 hours.
Examination
- Examine the patient to look for the potential source of infection.
- In addition, look for a mottled or ashen appearance, cyanosis of the skin, lips, or tongue, non-blanching rash or other rash indicating potential infection.
- It is recommended that patients at risk of deterioration and/or in whom sepsis is suspected are risk assessed using a structured set of observations, ie, vital signs.
Vital signs
Vital sign measurement is key to detection of early sepsis: ‘Measure and document.’ Sepsis is a time-crucial medical emergency and is usually preceded by measurable physiological abnormalities, ie, vital sign abnormalities.7 By early detection of these abnormalities, we can recognise the deteriorating patient in a timely manner and prioritise clinical response to improve patient outcomes.
Measuring and documenting the patient’s vital signs is crucial, even in a busy primary care environment. It provides essential, objective information. Vital signs should be interpreted in context, considering baseline values for the patient, and used as an adjunct to decision making, not as a replacement for clinical judgement. Vital sign measurement can be challenging, it has been demonstrated that most physiological vital signs were not recorded consistently by primary care teams.31,32
The SIX recommended vital signs for detection of sepsis are:
1. Respiratory rate (RR);
2. Oxygen saturations (sp02);
3. Heart rate (HR);
4. Systolic blood pressure (SBP);
5. Temperature;
6. Level of consciousness.
Risk stratification and management of sepsis
Sepsis is a complex, multisystem disease and requires diagnosis and treatment in hospital coordinated by a secondary care team with expertise in managing patients with sepsis. It is important to note that there is currently no gold standard for sepsis detection in primary care. Early warning scores have not been validated for use in primary care. There is however a growing evidence-base to support their use in the pre-hospital setting.33,34,35,36,37
Physiological assessments using the six vital sign measurements can be used to stratify patient risk, inform decision making, and improve communication at the interfaces of care. Although used in sepsis detection, single extreme vital sign scoring systems for defining sepsis have not been shown to be predictive of outcomes with suspected sepsis.38
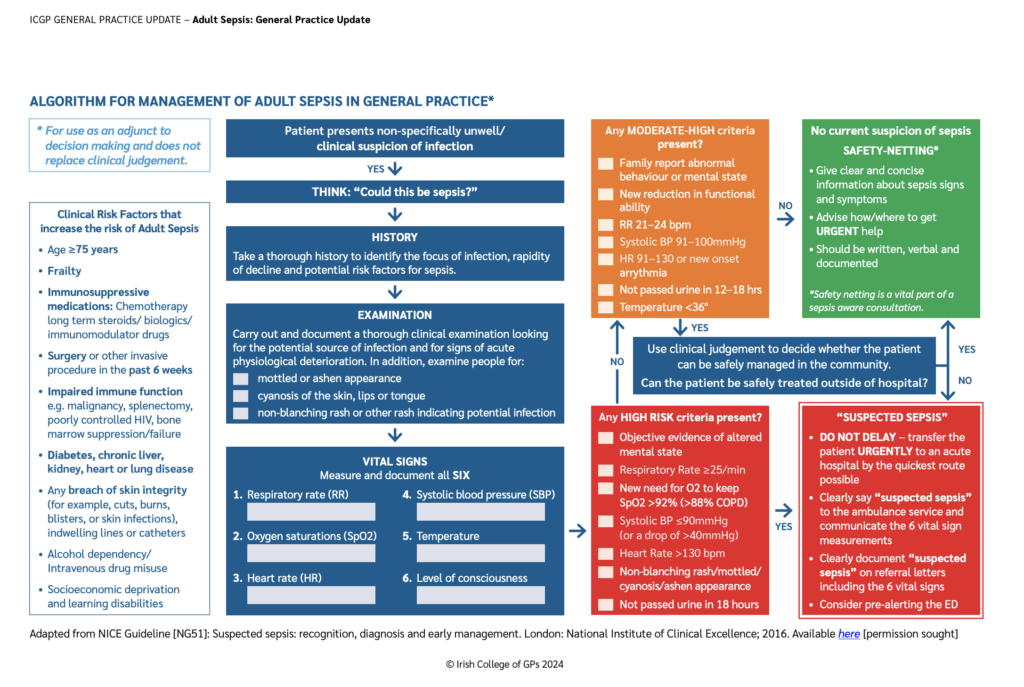
Recent UK guidance uses single vital sign measurements in addition to history and examination findings to aid decision making in the detection, assessment, and early management of suspected sepsis in primary care. Patients are stratified into high, moderate-high, and low-risk categories based on pre-defined criteria.
Recommendations on escalation of care are made according to risk category – see Figure 2. Clinical judgement remains paramount and vital signs/sepsis guidance should be interpreted in the context of what is normal for the patient, accurate history taking and examination, and the primary care setting.
Consider patients with any high-risk criteria to be at high-risk of severe illness or death from sepsis.11 If the patient meets any high-risk criteria, consider referral for emergency medical care.11
Transfer – transfer all patients to hospital immediately by the quickest route possible. Use local judgement around carer and private transport versus ambulance transfer.
State – clearly say “suspected sepsis” to the ambulance service and offer the findings of your assessment, eg, vital sign measurements, likely source of infection.
Document – clearly document “suspected sepsis” on referral letters to secondary care including vital sign measurements, likely source of infection.
Alert – pre-alerting before arrival in the emergency department (ED) has been found to almost halve the time of in-hospital treatment for patients.39 Consider phoning the hospital ED to notify a senior clinician that you are referring a high-risk patient with suspected sepsis.
Consider patients with any moderate- to high-risk criteria to be at moderate- to high-risk of severe illness or death from sepsis.11 If the patient meets any moderate- to high-risk criteria, use clinical judgement to decide whether the patient can be safely managed in the community. “If a definitive diagnosis cannot be made, or the person’s condition cannot be safely treated outside a hospital setting, refer urgently for emergency care.”11
If the patient does not meet any high or high- to moderate-risk criteria, consider them as being at low-risk of sepsis.11 Safety netting is vital here, give patients clear and concise information about sepsis symptoms that should prompt them to get urgent medical attention and advise patients how/where to get urgent help. Sepsis patient information leaflets (Figure 3) should be readily available for use in general practice.
Antimicrobial stewardship
Judicious antimicrobial prescribing is a key part of sepsis management. About 80-90 per cent of antibiotics are prescribed in primary care, and there is some evidence of unnecessary antibiotic prescribing.40,41 Antibiotic consumption in Ireland is high. We were the eighth highest prescribers of antibiotics among 28 EU member states in 2022.42
It is critical that we continue to work to reduce unnecessary antimicrobial use to decrease antimicrobial resistance (AMR). AMR occurs when an antimicrobial that was previously effective becomes less effective or is no longer effective to treat an infection or disease caused by a microorganism. It is one of the top threats to global health and it is estimated that in 2050, there will be 1·91 million annual deaths attributable to AMR globally and 8·22 million annual deaths associated with AMR.43
Treatment of sepsis can be complicated by the presence of multi-drug-resistant organisms and if infections cannot be treated adequately the risk of sepsis and associated morbidity and mortality increases. Continued alignment of the national sepsis programme with national antimicrobial stewardship and antimicrobial resistance prevention programmes is a key recommendation of the National Sepsis Report.10,44
The principles of antimicrobial stewardship can help protect antimicrobial treatment options. The ‘green/red’ list of antibiotics has been developed which assists community prescribers in choosing an antibiotic, see www.antibioticprescribing.ie. ‘Green list’ antibiotics are effective, have fewer side-effects, and are less likely to lead to resistant infections.
Conclusion
The most effective way to reduce morbidity and mortality from sepsis is by prevention, eg, vaccination. General practice teams have a vital role in vaccine promotion and administration. Sepsis is a common, life-threatening, time-critical emergency hiding in plain sight in our communities.
When assessing any adult who presents non-specifically unwell or with symptoms or signs that indicate possible infection: Think sepsis. Carefully count the respiratory rate, assess and document all six vital signs. Sepsis: Seek and you shall find.
References
- Irish College of GPs. Adult sepsis: General practice update. ICGP General Practice Updates (ICGP GPU) Dublin: ICGP; 2024. Available at: www.irishcollegeofgps.ie/.
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-10.
- Van Engelen TSR, Joost Wiersinga W, Van Der Poll T. Pathogenesis of sepsis. In: Wiersinga WJ, Seymour CW. Handbook of Sepsis [Internet]. Cham: Springer International Publishing; 2018 [cited 2024 May 20]. p. 31-43. Available at: www.link.springer.com/10.1007/978-3-319-73506-1_3.
- Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement programme. Critical Care Medicine. 2014;42(8):1749-55.
- Seymour CW, Gesten F, Prescott HC, et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med. 2017;376(23):2235-44.
- Peltan ID, Brown SM, Bledsoe JR, et al. ED door-to-antibiotic time and long-term mortality in sepsis. Chest. 2019;155(5):938-46.
- Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304-77.
- Health Service Executive. National Sepsis Report 2023. Dublin: HSE; 2023. Available at: www2.healthservice.hse.ie/organisation/sepsis/clinical-resources/.
- Esper AM, Moss M, Lewis CA, Nisbet R, Mannino DM, Martin GS. The role of infection and comorbidity: Factors that influence disparities in sepsis: Critical Care Med. 2006;34(10):2576-82.
- Health Service Executive. National Sepsis Report 2022. Dublin: HSE; 2022. Available at: https://assets.hse.ie/media/documents/National_Sepsis_Report_2022.pdf.
- National Institute for Health and
Care Excellence. Suspected sepsis:
Recognition, diagnosis, and early management: NICE guideline. Published: 13 July 2016. Last updated: 31 January 2024. Available at: www.nice.org.uk/guidance/ng51. - 12.Zhong X, Ashiru-Oredope D, Pate A, et al. Clinical and health inequality risk factors for non-Covid-related sepsis
during the global Covid-19 pandemic:
A national case-control and cohort study. eClinicalMedicine. 2023 Nov;102321. - NHS England. The Learning Disability Mortality Review (LeDeR) Programme Annual Report 2018. Available at:
www.england.nhs.uk/learning-disabilities/improving-health/learning-from-lives-and-deaths/. - Mahase E. Deprivation and learning disabilities linked to increased risk of dying from sepsis, study finds. BMJ. 2023;383:2795.
- Tsertsvadze A, Royle P, Seedat F, Cooper J, Crosby R, McCarthy N. Community-onset sepsis and its public health burden: A systematic review. Syst Rev. 2016;5(1):81.
- Gray A, Ward K, Lees F, et al. The epidemiology of adults with severe sepsis and septic shock in Scottish emergency departments. Emerg Med J. 2013;30(5):397-401.
- Loots FJ, Smits M, van Steensel C, Giesen P, Hopstaken RM, van Zanten ARH. Management of sepsis in out-of-hours primary care: A retrospective study of patients admitted to the intensive care unit. BMJ Open. 2018;8(9):e022832.
- Centres for Disease Control and Prevention. CDC vital signs. Making healthcare safer. Think sepsis. Time matters [Online]. US: CDC; 2016. Available at: www.cdc.gov/vitalsigns/sepsis/index.html.
- World Health Organisation. Global report on the epidemiology and burden of sepsis: Current evidence, identifying gaps, and future directions. Geneva: WHO; 2020.
- Royal College of Physicians of Ireland. National Immunisation Advisory Committee (NIAC). NIAC Immunisation Guidelines. Chapter 3. Immunisation of the immunocompromised person. 2023.
- Health Service Executive. Pneumococcal vaccine. Available at: www2.hse.ie/conditions/pneumococcal-vaccine/.
- Health Service Executive. Covid-19 screening and vaccinations. Available at: www2.hse.ie/screening-and-vaccinations/covid-19-vaccine/.
- Royal College of Physicians of Ireland NIAC Immunisation Guidelines. Chapter 15. Pertussis. National Immunisation Advisory Committee (NIAC); 2016.
- Royal College of Physicians of Ireland. National Immunisation Advisory Committee (NIAC). NIAC Immunisation Guidelines. Chapter 11. Influenza. In: NIAC Immunisation Guidelines Chapter 11 Influenza. Royal College of Physicians of Ireland. National Immunisation Advisory Committee (NIAC); 2022.
- National Health and Medical Research Council. Australian Guidelines for the Prevention and Control of Infection in Healthcare. Canberra;2019. Available at: www.safetyandquality.gov.au/publications-and-resources/resource-library/australian-guidelines-prevention-and-control-infection-healthcare.
- National Institute for Health and Care Excellence. Healthcare-associated infections: Prevention and control in primary and community care. NICE Clinical guideline [CG139]. Published: 28 March 2012 Last updated: 15 February 201.
- Young YM, Hamilton V, Bedding M, et al. Sepsis awareness: An Irish survey. Int J Integr Care. 2017;17(5):198.
- Department of Health. NCEC National Clinical Guideline No. 26. DOH; 2021. Available at: http://health.gov.ie/national-patient-safety-office/ncec/.
- Sands MB, Sharma S, Carpenter L, et al. “SQiD, the Single Question in Delirium; can a single question help clinicians to detect delirium in hospitalised cancer patients?”. BMC Cancer. 2021;21(1):75.
- Boockvar K, Brodie HD, Lacks M. Nursing assistants detect behaviour changes in nursing home residents that precede acute illness: Development and validation of an illness warning instrument. J American Geriatrics Society. 2000;48(9):1086-91.
- E. Hayes, L. Gannon, D. Quinlan. Sepsis and documentation of six physiological vital signs in GP out-of-hours. Ir Med J. 2023; 116(9);857.
- National Confidential Enquiry into Patient Outcome and Death. Just say sepsis! A review of the process of care received by patients with sepsis. 2015. Available at: www.ncepod.org.uk/2015report2/downloads/JustSaySepsis_FullReport.pdf.
- Inada-Kim M. NEWS2 and improving outcomes from sepsis. Clin Med (Lond). 2022;22(6):514-7.
- Inada-Kim M, Knight T, Sullivan M, et al. The prognostic value of national early warning scores (NEWS) during transfer of care from community settings to hospital: A retrospective service evaluation. BJGP Open. 2020;4(2):bjgpopen20X101071.
- Patel R, Nugawela MD, Edwards HB, et al. Can early warning scores identify deteriorating patients in pre-hospital settings? A systematic review. Resuscitation. 2018;132:101-11.
- Scott LJ, Redmond NM, Tavaré A, Little H, Srivastava S, Pullyblank A. Association between National Early Warning Scores in primary care and clinical outcomes: An observational study in UK primary and secondary care. Br J Gen Pract. 2020;70(695):e374-80.
- NEWS2 in out-of-hospital settings, the ambulance and the emergency department. Authors: Tavaré A, Pullyblank A, Redfern E, Collen A, Robert O, Barker E, Gibson A. Clinical Medicine 2022 Vol 22, No 6: 525-9.
- Bion J, Barton G, Boyle A, Carlson G, Carrol E, Christian W, Crossland S, Faust S, Gabbay F, Gent N, Gibbs P, Harden J, Howard P, Inada-Kim M, Lanzman M, Leanord A, Lees N, Noursadeghi M, Rajesh P, Shrestha S, Sriskandan S, Stockley S, Waldmann C, Walsh T, Wilson P, Singer M. Academy of Medical Royal Colleges Statement on the Initial Antimicrobial Treatment of Sepsis. Academy of Medical Royal Colleges 2022.
- Studnek JR, Artho MR, Garner CL, Jones AE. The impact of emergency medical services on the ED care of severe sepsis. The American Journal of Emergency Medicine. 2012 Jan;30(1):51-6.
- Dekker ARJ, Verheij TJM, Van Der Velden AW. Inappropriate antibiotic prescription for respiratory tract indications: Most prominent in adult patients. FAMPRJ. 2015 Apr 24;cmv019.
- Pouwels KB, Dolk FCK, Smith DRM, Robotham JV, Smieszek T. Actual versus ‘ideal’ antibiotic prescribing for common conditions in English primary care. Journal of Antimicrobial Chemotherapy. 2018 Feb 1;73(suppl_2):19-26.
- HPSC. European Surveillance of Antimicrobial Consumption (ESAC): Report 1. [Internet]. Ireland: Health Protection Surveillance Centre; [Quarter 4, 2023] [accessed 2024 May 15]. Available at: www.hpsc.ie/a-z/microbiologyantimicrobialresistance/europeansurveillanceofantimicrobialconsumptionesac/PublicMicroB/SAPC/Report1.html#International_Comparison].
- Naghavi M, Vollset SE, Ikuta KS, Swetschinski LR, Gray AP, Wool EE, et al. Global burden of bacterial antimicrobial resistance 1990-2021: A systematic analysis with forecasts to 2050. The Lancet. 2024 Sep;404(10459):1199-226.
- Health Service Executive. HSE. National Sepsis Report 2021 [Internet]. Health Service Executive; 2023 [cited 2023 Jun 29]. Available at: www.hse.ie/eng/about/who/cspd/ncps/sepsis/resources/national-sepsis-report-2021.pdf.












Leave a Reply
You must be logged in to post a comment.