







Reference: May-June 2026 | Issue 3 | Vol 19 | Page 43
Osteoporosis is a major cause of disability but prevention and targeted treatment can reduce the risk of falls and fractures
Osteoporosis is a condition where bones lose density, in turn making fractures more likely. Approximately 50 per cent of women and 20 per cent of men aged over 50 will experience a fracture due to osteoporosis. Osteoporosis can affect all age groups, but it is most common in postmenopausal women.
Osteoporosis does not automatically mean bones will fracture ‒ it just means fractures are more likely. Osteoporosis is a bigger cause of disability than common non-communicable diseases such as Parkinson’s disease, rheumatoid arthritis, and breast cancer.
The Irish Osteoporosis Society (IOS) estimates that around 300,000 people in Ireland are living with osteoporosis. Recent HSE and international data suggest that this number may now be rising gradually, driven by Ireland’s ageing population, longer life expectancy, and low diagnosis rates.
The IOS continues to highlight that up to 70 per cent of cases remain undiagnosed until a fracture occurs, underscoring the need for better screening and early intervention.
Symptoms
Osteoporosis may have no symptoms initially, and patients may be unaware of any problems until they fracture a bone or start to lose height.
The most common fractures associated with osteoporosis are broken wrists, hips, and spinal bones but fractures can occur in any bone. This leads to pain, disability, loss of independence, and influences self-esteem. Symptoms can include:
✽ Upper, middle, or lower back pain that can be severe
✽ Loss of height (greater than 2cm)
✽ Development of a hump on the back or a change in body shape, for example, the rib cage may rest on pelvic rim, or a pot belly develops.
Diagnosis
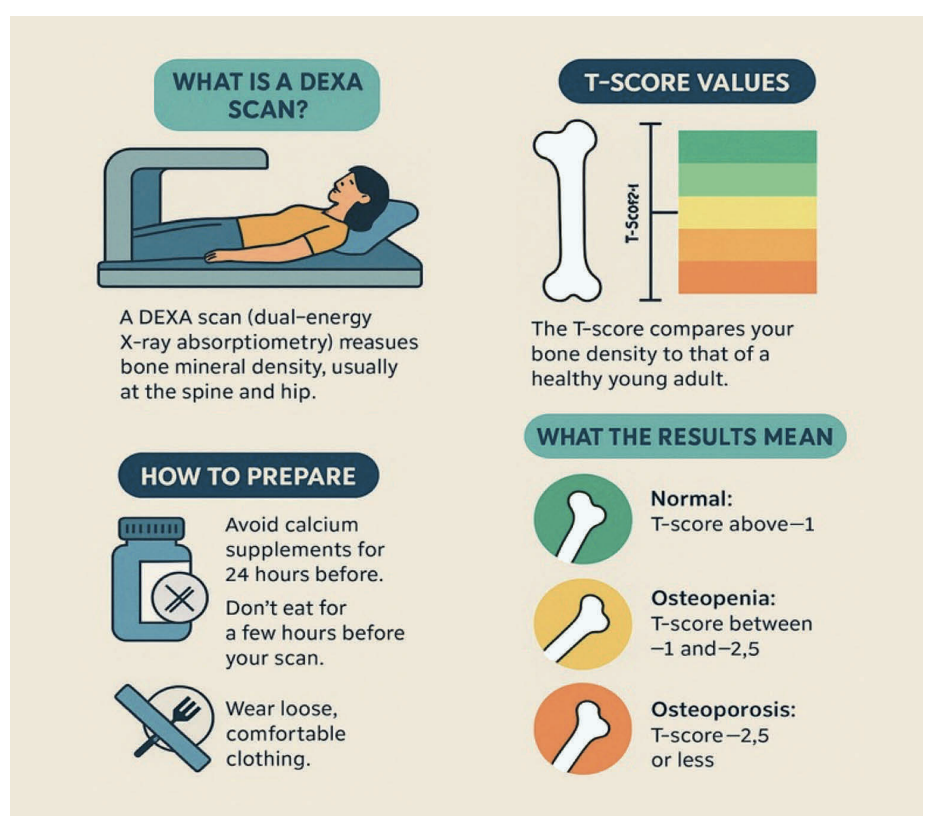
Diagnosis often only occurs after a fall or a bone fracture. Bone density is measured using a dual-energy x-ray absorptiometry (DEXA) scanner. A DEXA scan uses low energy x-rays to determine the density profile of x-rays that pass through the bone and from this information the average density of bone is determined. Osteoporosis is diagnosed when bone density is found to be significantly lower than average.
DEXA scans are painless, take 10-20 minutes, and are the gold standard for the diagnosis of osteoporosis.
The results of the scan are available immediately or very soon after, depending on where it is done. Scan results are in the form of a T-score. A T-score value greater than -1 shows that bone density level is normal and there is no osteoporosis. A T-score value of between -1 and -2.5 indicates osteopenia.
Osteopenia indicates early stages of osteoporosis and is an opportunity for early interventions like modification of risk factors including diet, smoking, and excessive alcohol intake to prevent osteoporosis developing. A T-score of below -2.5, meanwhile, indicates osteoporosis (Figure 1).
Improved GP access to osteoporosis diagnostics
Ireland still does not have a national osteoporosis screening programme, meaning that DEXA scans remain largely dependent on GP referral. While access has improved in recent years, waiting times for public patients remain variable across regions. Private DEXA services are still readily available and listed by county on the IOS website, which remains the most complete public directory of scanning facilities.
Since the HSE’s 2021 direct access initiative, GPs have been able to refer public patients for a range of diagnostic tests – including DEXA scans, x-rays, CT, and MRI – in participating private hospitals, with costs covered by the HSE. The goal was to ensure urgent referrals are completed within one month, and routine cases within three months.
According to HSE updates through 2024-2025, the scheme has expanded, with more than 140,000 diagnostic slots now available annually. However, reports from primary care suggest regional disparities persist, with DEXA scan delays still notable in some areas.
Causes
Strong healthy bones comprise of a mix of protein and minerals, including calcium and phosphorous. Bone is living tissue that is maintained and renewed by two types of cells. Osteoblast cells build up new bone and osteoclast cells break down old bone. Up to the mid-20s, the skeleton strengthens, but from the 40s onwards, bones gradually lose their density as a natural part of ageing.
There is a genetic influence with osteoporosis, so women who have family members with the condition are more at risk. However, other factors increase the risk of osteoporosis. Oestrogen protects women from osteoporosis from puberty until the menopause. After menopause, the breakdown of bone is quicker as the protective effect of oestrogen on the bones is gone.
Primary issues that increase the likelihood of osteoporosis include early menopause; total hysterectomy with bilateral salpingo-oophorectomy before 45 years; and excessive exercise. Other risk factors include age; race (Caucasian or Asian patients are at increased risk compared to African-Caribbean patients); gender, as smaller bones and less muscle mass put women at more risk; family history of osteoporosis, particularly a history of hip fracture in a parent; previous fragility fracture; long-term immobility; very low body mass index (BMI) (less than 18.5kg/m2); and excessive alcohol consumption or smoking.
Low dietary intake of vitamin D and calcium is also a notable risk. Diet-related factors include:
✽ Being vegan: A vegan diet limits the amount of calcium and vitamin D consumed.
✽ Excess fibre: While fibre is healthy in the diet, more than 30g of fibre a day can reduce calcium absorption. However, the association between fibre and osteoporosis is not strong, and high-fibre foods like fruit and vegetables are good for overall health, while green leafy vegetables are a good source of calcium.
✽ Caffeine: Excess caffeine can increase calcium excretion, thus increasing osteoporosis risk.
Medication and disorders can increase risk including:
✽ Long-term use of corticosteroids. Patients require preventive treatment for osteoporosis if they are starting oral corticosteroids and are likely to be on these for at least three months.
✽ Long-term use of heparin
✽ Aromatase inhibitors (for breast cancer treatment)
✽ Overactive thyroid disorders
✽ Rheumatoid arthritis
✽ Digestive disorders that affect nutrient absorption such as Crohn’s disease, chronic liver disease, or coeliac disease.
Causes in pre-menopausal women: Oestrogen prevents osteoporosis in pre-menopausal women. However, there are certain medical conditions and medications that reduce oestrogen levels, causing early-onset osteoporosis. Examples include:
✽ Hypogonadotropic hypogonadism caused by low body weight, eating disorders, excessive exercise, hyperprolactinemia, and hypopituitarism.
✽ Hypergonadotropic hypogonadism (premature ovarian failure) is associated with bone loss if oestrogen is not replaced. Women with Turner syndrome (a condition which occurs in less than one in 2,500 due to abnormal X chromosome) may have an additional selective reduction in bone mineral density that is independent of oestrogen exposure.
✽ In premenopausal women with breast cancer, chemotherapy often results in premature ovarian failure, and as a result, oestrogen deficiency and bone loss.
Drugs associated with bone loss in premenopausal women include glucocorticoids, anticonvulsants, antidepressants, and anticoagulants.
Criteria for assessing osteoporosis fracture risk
The National Institute for Health and Care Excellence (NICE) recommends validated fracture risk assessment tools, such as FRAX or QFracture, to estimate a patient’s 10-year probability of a major osteoporotic fracture or hip fracture. The most recent guidance (NICE NG226, updated 2023) refines some risk criteria and reinforces the importance of early assessment in both men and women.
Fracture risk assessment should be considered for:
✽ Women aged ≥65 years and men aged ≥75 years, regardless of additional risk factors.
✽ Younger adults (women <65, men <75) if one or more risk factors are present:
– Previous fragility fracture
– History of falls
– Parental hip fracture
– Low BMI (<18.5kg/m²)
– Current or frequent glucocorticoid use (oral or systemic)
– High alcohol intake (>14 units/week for women; >21 units/week for men)
– Smoking
– Conditions causing secondary osteoporosis (ie, rheumatoid arthritis, malabsorption, untreated hypogonadism).
Fracture risk assessment is not routinely indicated in people under 50 years unless they have major secondary risk factors like premature menopause, previous fragility fracture, or chronic/repeated corticosteroid use.
Non-pharmacological management
Non-pharmacological management includes prevention of falls and modification of risk factors like diet, smoking, and excessive alcohol intake. Important measures aimed at preventing falls include attention to modifiable factors, such as checking eyesight, exercise, reduced consumption of medication that alters alertness and balance, and improvement of the home environment.
There is debate regarding the use of hip protectors to prevent hip fractures, with evidence casting doubt on this preventive measure.
Nutritional intake: Attention to diet is important, because there is a high prevalence of calcium and vitamin D insufficiency, particularly among the elderly and multimorbid populations. A diet with adequate calcium (>1,200mg daily) and vitamin D (800IU daily) is recommended for those with risk factors ‒ however, supplementation and fortified foods are often required to achieve requirements.
The benefits of calcium and vitamin D supplements to maintain optimum bone density in healthy adults with normal dietary intake remains limited.
Exercise: Osteoporosis patients need to be careful of vigorous, high-impact exercise, although being active improves balance and co-ordination, increases muscle strength, and reduces falls and fractures. Beneficial exercise includes swimming, gardening, walking, and golf.
Physiotherapy falls prevention programmes: Most HSE physiotherapy departments across Ireland continue to offer falls prevention programmes for patients referred by GPs or hospital consultants. Referral criteria typically include reduced mobility, a history of falls, or a fear of falling – all key risk factors for both fracture and functional decline in older adults.
These programmes are still largely modelled on the Otago Exercise Programme, which combines progressive strength, balance, and gait training. Since 2023, several community specialist teams for older people and enhanced community care networks have integrated such programmes into primary care settings, making access easier for older adults without requiring hospital attendance.
Some regions have also adopted group-based and home-based exercise models supported by chartered physiotherapists, public health nurses, and occupational therapists, often supplemented with digital or telehealth follow-up introduced during and after the Covid-19 pandemic.
Evidence from Irish pilot sites (2023-2025) indicates that these multidisciplinary fall prevention initiatives can significantly reduce falls recurrence and hospital admissions, while improving confidence and independence among participants.
HSE falls prevention policy: The core principles of the HSE’s 2008 Strategy to Prevent Falls and Fractures in Ireland’s Ageing Population remain in place, and recent initiatives have strengthened implementation and integrated falls prevention into community and residential care programmes.
In 2023, the HSE and Department of Health reaffirmed falls prevention as a key element of Healthy Ageing and Sláintecare Integration projects, supporting early intervention and bone health assessment in primary care. Updated training resources now promote multifactorial assessment and fracture prevention, particularly for individuals at risk of a major osteoporotic fracture.
Current guidance for community-dwelling older adults includes annual screening questions like:
✽ “Have you fallen in the past year?”
✽ “Do you feel unsteady or have balance problems?”
✽ “Are you worried about falling?”
Those with recurrent or unexplained falls, gait or balance issues, or a fear of falling, should undergo a comprehensive assessment covering: Medication review, postural hypotension, vision, foot health, and home environment.
The role of vitamin D supplementation continues to be emphasised, with HSE and the Health Information and Quality Authority (HIQA) both recommending regular assessment and treatment for deficiency in long-term care residents. Exercise programmes incorporating strength, balance, and co-ordination remain the most evidence-based intervention.
In residential and nursing care settings, HIQA inspections now routinely assess:
✽ Existence and implementation of a falls prevention policy
✽ Annual falls risk assessments (and reassessment following health changes)
✽ Recording and review of each fall, including corrective action.
Since 2022, HIQA reports have noted improvements but also highlighted variation in fall prevention practice between facilities. Some community health networks have also begun piloting falls and fracture liaison services to ensure that residents who experience a fracture receive post-fall osteoporosis assessment and treatment, helping close a long-standing care gap.
Pharmacological management
BISPHOSPHONATES
Bisphosphonates slow the activity of osteoclasts. Examples include alendronic acid, risedronate sodium, and ibandronic acid. Oral bisphosphonates are taken once weekly, apart from ibandronic acid, which is once a month. Oral bisphosphonates are advised for patients with osteoporosis only if the 10-year risk of a fracture is at least 1 per cent.
An intravenous (IV) bisphosphonate available in Ireland is zoledronic acid. It is advised when the 10-year risk of fracture is at least 10 per cent, or when it is at least 1 per cent and oral bisphosphonates are contraindicated or poorly tolerated.
Zoledronic acid (Aclasta 5mg/100ml) is administered once a year by an intravenous (IV) infusion over 15 minutes. IV infusion ibandronic acid is licensed in UK and other countries but not available in Ireland.
The oral bioavailability of bisphosphonates is low and impaired by food. Oral formulations must be taken when fasting and sitting upright with a full glass of water, followed by no food for up to one hour. Patients are asked to sit upright to reduce the gastrointestinal effects such as oesophageal irritation. Compliance with treatment is a problem, particularly in view of these requirements.
Common side effects (over one in 100) of bisphosphonates are:
✽ Gastrointestinal side effects including non-ulcer dyspepsia
✽ Muscle, joint, or back pain and stiffness
✽ Headache
✽ Tiredness.
Less common side effects of bisphosphonates include:
✽ Oesophagitis
✽ Oesophageal strictures (narrowing of oesophagus)
✽ Gastric and duodenal ulcers
✽ An unusual fracture of the thigh bone (very rare)
✽ Osteonecrosis of the jaw (ONJ).
Bisphosphonates are contraindicated in the presence of abnormalities of the oesophagus and hypocalcaemia. Alendronates in tablet form should not be crushed, as this increases risk of oesophageal irritation. For patients with slow or poor swallow, alendronic acid 70mg/100ml liquid form does not cause oesophageal irritation; however, the same precautions such as sitting upright after taking and not eating for an hour after taking still hold true for the liquid version.
Risk of ONJ: There have been reports of ONJ, particularly with IV formulations given in high doses for metastatic bone disease. The prevalence of ONJ with bisphosphonates is about one in 100,000 patient-years, which is similar to the prevalence in the overall population.
Patients who develop sudden pain in the jaw while on bisphosphonates, especially IV versions, should report to their doctor as this can be a sign of ONJ. Patients prescribed the IV infusion forms of bisphosphonates can experience flu-like symptoms for a few days after the infusion, especially after their first infusion.
DENOSUMAB
Denosumab (ie, Prolia and new biosimilar entrants) is an alternative option if the patient is intolerant of oral bisphosphonates or unsuitable. It is given by six-monthly subcutaneous injections. Denosumab is a monoclonal antibody that works by inhibiting the cytokine RANKL (receptor activator of NFκB ligand). RANKL is an essential factor promoting bone turnover.
Denosumab inhibition of RANKL blocks osteoclast maturation, function, and survival, thus reducing bone resorption so increasing bone density. Patients should take adequate calcium and vitamin D while on denosumab as it can lower calcium levels significantly.
Side effects include:
✽ Skin infections
✽ Hypocalcaemia which can lead to:
– Numbness or tingling in extremities including fingers, toes, and around the mouth
– Muscle cramps, spasms, and twitches.
Denosumab is a treatment option for the primary prevention of fractures in postmenopausal women (diagnosed with osteoporosis) at increased risk of fractures who:
✽ Find difficulty complying with the specific instructions for administering oral bisphosphonates (hour before food, sit or stand for period after taking) or oral bisphosphonates are contraindicated or not tolerated; and
✽ Have a combination of T-score, age, and number of independent clinical risk factors for fracture as indicated in Table 1.
| Number of independent clinical risk factors for fracture |
|||
|---|---|---|---|
| Age (years) | 0 | 1 | 2 |
| 65-69 | N/R | -4.5 | -4.0 |
| 70-74 | -4.5 | -4.0 | -3.5 |
| 75 or older | -4.0 | -4.0 | -3.0 |
| N/R: Treatment with denosumab is not recommended | |||
TABLE 1: T-scores at (or below) which denosumab is recommended when oral bisphosphonates are unsuitable
Independent clinical risk factors for fracture include:
✽ Parental history of hip fracture
✽ Alcohol intake of more than four units per day
✽ Rheumatoid arthritis.
Xgeva is a higher-strength Denosumab preparation (ie, Denosumab 120mg) that is licensed for the prevention of skeletal-related events (pathological fracture, radiation to bone, spinal cord compression, or surgery to bone) in adults with advanced cancers involving the bone. The dose is 120mg by subcutaneous injection every four weeks but there may be additional doses over the first four weeks for some bone cancers ‒ ie, giant cell tumour of bone. Unlike Prolia, Xgeva is available via the Hi-Tech scheme.
| Number of independent clinical risk factors for fracture |
|||
|---|---|---|---|
| Age (years) | 0 | 1 | 2 |
| 50-54 | N/R | -3.5 | -3.5 |
| 55-59 | -4.0 | -3.5 | -3.5 |
| 60-64 | -4.0 | -3.5 | -3.5 |
| 65-69 | -4.0 | -3.5 | -3.0 |
| 70-74 | -3.0 | -3.0 | -2.5 |
| 75 or older | -3.0 | -2.5 | -2.5 |
| N/R: Treatment with raloxifene is not recommended | |||
TABLE 2: T-scores at (or below) which raloxifene is recommended when oral bisphosphonates are unsuitable
PARATHYROID HORMONE PEPTIDES
Teriparatide is the only osteoporosis drug in this class, and brands include Forsteo, Movymia, and Sondelbay. They are available via the Hi-Tech scheme. Teriparatide is delivered as a 20mcg subcutaneous injection once daily. It should be used for a maximum of two years ‒ the full two-year course should be completed to obtain best clinical outcome, and it should not be prescribed again over the patient’s lifetime. After stopping, an alternative osteoporosis treatment may be considered.
Teriparatide is a treatment option for the primary prevention of fractures only in postmenopausal women (diagnosed with osteoporosis) at increased risk of fractures who:
✽ Find difficulty complying with the specific instructions for administering oral bisphosphonates (hour before food, sit or stand for period after taking) or if oral bisphosphonates are contraindicated or not tolerated
✽ Are over 65 years with a T-score of -4.0 or below, or a T-score of -3.5 or below plus two or more fractures, or who are aged 55 to 64 years with a T-score of -4 or less plus two or fractures.
SELECTIVE OESTROGEN RECEPTOR MODULATOR
This is a synthetic hormone that mimics the effect of oestrogen on the bones. The dose (ie, raloxifene) is 60mg daily. According to NICE guidelines, raloxifene is an alternative treatment option for the primary prevention of fractures only in postmenopausal women (diagnosed with osteoporosis) at increased risk of fractures who fulfill the criteria below and in Table 2.
Independent clinical risk factors for fracture include:
✽ Find difficulty complying with the specific instructions for administering oral bisphosphonates (hour before food, sit, or stand for period after taking) or oral bisphosphonates are contraindicated or not tolerated (ie, persistent upper gastrointestinal disturbance)
✽ Have a combination of T-score, age, and number of independent clinical risk factors for fracture as indicated in Table 2.
Raloxifene has been associated with an increased risk of venous thrombosis similar to that linked to hormone replacement therapy (HRT), and with exacerbation of hot flushes. An increased risk of death due to stroke has been reported with raloxifene, and it should be used with caution in women with a history of, or risk factors for, stroke.
It is contraindicated in women with child-bearing potential, history of venous thromboembolism, or unexplained uterine bleeding, hepatic impairment, and severe renal impairment.
HRT
The use of HRT for osteoporosis prevention is restricted to short-term use for younger post-menopausal women with menopausal symptoms at high risk of fracture.
First new osteoporosis drug in more than 10 years
ROMOSOZUMAB
Romosozumab (Evenity 105mg subcutaneous injection) is a new monoclonal antibody treatment option for severe osteoporosis and is the first new osteoporosis drug to come to market in over 10 years. It works by inhibiting sclerostin, ultimately increasing bone formation and decreasing bone resorption.
It is reserved for use in postmenopausal women with severe osteoporosis, patients who are intolerant to other treatments, or when other treatments have failed.
While not directly compared to denosumab yet, it appears to be as effective in preventing fractures – and there are early indications it may be more effective than denosumab in preventing non-spinal fractures, including hip fractures.
In postmenopausal women, criteria for selecting romosozumab over bisphosphonates is one severe or two moderate low-trauma fractures, ie, same criteria as teriparatide. The recommended dose of romosozumab is 210mg (administered as two subcutaneous injections of 105mg) once monthly for 12 months.
After 12 months, it can be followed with alternative osteoporosis treatment such as denosumab or a bisphosphonate to allow continued protection, as its benefits wear off quickly after stopping.
Contraindications of romosozumab:
✽ History of stroke or heart attack
✽ Hypocalcaemia: Adequate intake of calcium and vitamin D before commencing romosozumab is advised
✽ Pregnancy or breast feeding: While it is only licensed for women post-menopause, it may be prescribed by specialists for women pre-menopause.
Osteoporosis in men
Oral bisphosphonates alendronic acid and risedronate sodium are recommended first-line treatments for osteoporosis in men. Zoledronic acid or denosumab are alternatives in men intolerant of oral bisphosphonates or are otherwise unsuitable. Teriparatide is an additional alternative option for men.
Men undergoing androgen-blocking therapy for prostate cancer have increased risk of fracture, and a bisphosphonate can be offered to these male patients with confirmed osteoporosis and where fracture risk is present. Denosumab may be considered as an alternative for these patients where bisphosphonates are unsuitable or not tolerated.
References available on request












Leave a Reply
You must be logged in to post a comment.