







The future of migraine care, and more widely headache care, is no longer a distant prospect; it is here
For decades, the field of migraine prevention worldwide has been defined by what could only be described as clinical ‘hand-me-downs’. Because specific molecular treatments were unavailable until very recently, clinicians in primary care and hospitals were forced to rely on repurposed medications to treat their migraine patients. These non-specific agents, which were happened upon by chance, included such medicines as antihypertensives, anticonvulsants, and antidepressants. We are all familiar with these non-specific preventive treatments: Topiramate, pizotifen, amitriptyline, flunarizine, venlafaxine, and propranolol. They were never designed for the migraine brain and they were utilised out of necessity as there was nothing else available that had any decent level of efficacy. They were ‘blunt instruments’ that often resulted in systemic side-effects or ‘collateral damage’, leading to high discontinuation rates, mainly due to poor tolerability and lack of efficacy. For example, it is well established in several trials that somewhere between 35 and 45 per cent of patients with episodic/chronic migraine stop these daily oral preventive treatments in year one due to side-effects alone. In addition, approximately the same proportion stop in year one due to lack of efficacy. Consequently, approximately 80 per cent of patients or more stop these migraine therapies in year one due to side-effects or lack of efficacy or both. I think that we can all agree that this is bad clinical practice and futile medicine. The only other preventive treatment that was available for more chronic patients in the last 20 years was periodic Botox (onabotulinum toxin A) injections using the PREEMPT protocol, which involves giving 31 injections approximately four times a year (every 12/13 weeks). However, this treatment is expensive, labour intensive and is only available in a few specialist clinics around the country. It is, however, very effective for some of our more chronic and refractory patients, and we continue to use it in selected patients in our clinics.
For the field of headache medicine, the last few years have changed completely the way that we practise in our specialist hospital-based headache/migraine clinics, both in Ireland and worldwide. Since the end of 2018, we have witnessed an enormous evidence-based shift away from non-specific treatments to that of pathophysiology-driven, molecular biology therapies which are highly efficacious and have significantly lower side-effects. By targeting the molecular mechanisms of migraine and specifically using calcitonin gene-related peptide (CGRP) therapies, we are finally moving away (albeit slowly) from the low efficacy and systemic ‘collateral damage’ of older agents. This evolution has not only been overwhelmingly positive for clinical efficacy, but it has also been a ‘game changer’ for improving patient adherence and quality-of-life by providing tolerable, targeted interventions. Patients are now frequently using the term ‘life-changing’ every day in our clinics. It is a very positive time for patient care. There are currently six CGRP specific therapies available in Ireland for migraine prevention: Three self-administered monoclonal antibody injections (erenumab, fremanezumab, and galcanezumab) once a month or every 28 days, one intravenous monoclonal antibody (eptinezumab) given every three months, and two daily oral tablets (atogepant and rimegepant).
There is no doubt that clinical practice in secondary/tertiary care has been transformed for a proportion of patients who have access to specialist hospital headache services, albeit with some caveats. However, primary care in Ireland is not being allowed to move forward in the same way and the majority of patients are suffering unnecessarily. The barriers that remain for most migraine patients are mainly financial and are being enforced by the HSE, with restrictive managed access programmes (MAP) being employed, which are limited to a few clinical specialists. These MAP exclude almost all primary care and are mandatory in secondary/tertiary care. They are run by the HSE’s Medicines Management Programme and the protocols dictate that clinicians should use the ‘old ways’ (at least three historical, non-specific oral preventives) for a total of at least six–12 months prior to approval of the newer, more appropriate molecular treatments. Currently, this negative practice applies specifically to CGRP monoclonal antibodies and gepants. We would argue that these therapies should be first-line options. Mainly because of these finance-driven MAP, approximately 90 per cent of all migraine preventive CGRP therapies in Ireland are prescribed by only 15–20 individual consultants/doctors. To add to this injustice and restrictive practice, patients attending specialised hospital services are forced to wait for long periods for outpatient appointments, often one to two years due to inadequate resources for specialist headache/migraine services in hospitals throughout the country. When the patients are eventually seen in specialist clinics, they then need to provide pharmacy evidence of oral preventive failures for qualification. There are barriers for patient care at almost every level.
Global consensus for CGRP therapies as the new first-line standard
A major breakthrough in the traditional migraine preventive ‘step-care’ model has arrived, both in Ireland and worldwide: The medical community no longer accepts that patients should fail multiple poorly tolerated, non-specific drugs before being offered disease-specific molecular treatments (Figure 1). The major international headache societies including the American Headache Society, the European Headache Federation, and the International Headache Society, have all reached a critical inflection point in their management philosophies. The position statements for each organisation are:
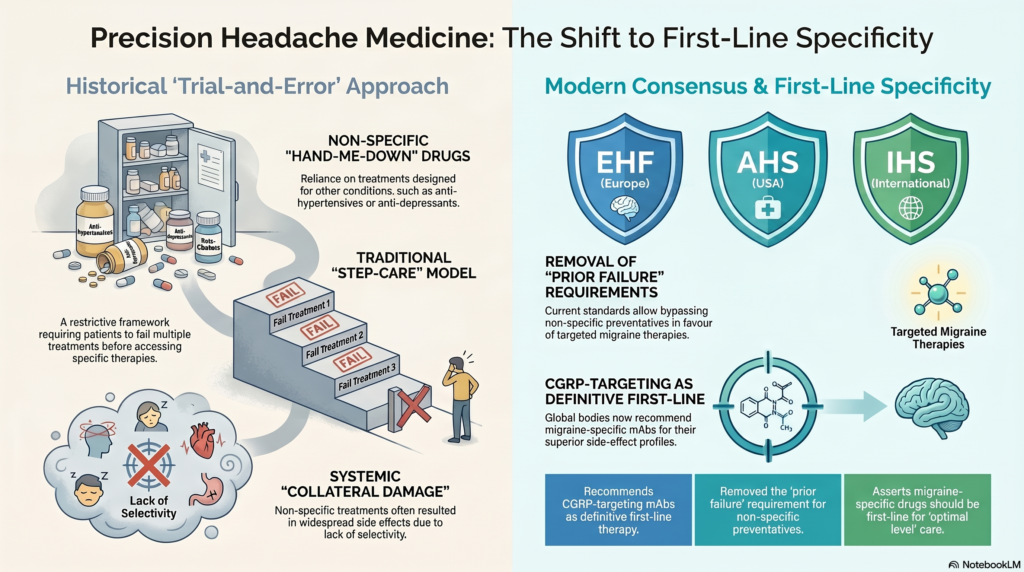
▶ European Headache Federation (EHF): The EHF now explicitly recommends that monoclonal antibodies (mAbs) targeting the CGRP pathway be included as a first-line treatment option. This recommendation is based on their superior side-effect profile and highly specific mechanism of action compared to legacy treatments.
▶ American Headache Society (AHS): In a significant move in 2025, the AHS recommended removal of the ‘prior failure’ requirement. In their opinion, CGRP-targeting therapies should now be positioned alongside historical preventives as a first-line approach, allowing clinicians to bypass the traditional trial-and-error period with older drugs.
▶ International Headache Society (IHS): Operating under an ‘optimal level’ management philosophy, the IHS Practice Recommendations state that where resources permit, the first treatment option should always be a migraine-specific drug, even when comorbidities are present.
The clinical impact of these concordant recommendations for use of specific molecular migraine treatments cannot be overstated. There is emerging evidence that using these therapies as first-line options may change the long-term prognosis for more chronic migraineurs by preventing disease progression and avoiding the cumulative ‘treatment fatigue’ caused by the side-effects of non-specific agents. In addition, by intervening with high specificity early in the disease course, the hope is to maximise the chances of maintaining neurological stability and avoiding hypersensitisation of neuronal pathways which can lead to more chronic migraine. Overall, it is very clear that this evolving strategy is best for patients, and their needs should be our primary goal. These new CGRP pathway targeting molecular treatments are superior in almost every way as compared to prior historical preventive therapies, with the only downside being cost in the initial phase. Moreover, there is overwhelming international evidence that we need to significantly reduce or stop altogether using a significant proportion of the older medications used in migraine: Topiramate and valproate are perfect examples given the risks that they pose and considering that most of our patients with migraine are female. It is no longer justified to continue what we are doing.
The HSE should follow the lead of the IHS, EHF, and AHS, and allow easier access to these new molecular medicines as first-line treatments in appropriate patients. We believe that what they are currently doing is morally and clinically unjust. We need to consider firstly, the ‘human’ costs in terms of suffering for our patients and secondly, the financial costs. The financial costs to the State will be higher in the first instance, but there is good evidence from recent studies that much of this cost will be recouped in the medium-term (one to five years). It is clear that there will be significant financial cost savings going forward, both directly and indirectly. For example, there will be fewer unscheduled visits to primary care and hospital emergency departments, fewer inpatient days, and also patients will be more productive in the workforce, providing additional revenue for the Government. Most importantly, patients will benefit from better clinical care at an earlier stage of disease, and overall migraine health will improve. Again, patient welfare should always be our primary goal.
Beyond CGRP: The next phase of precision headache medicine
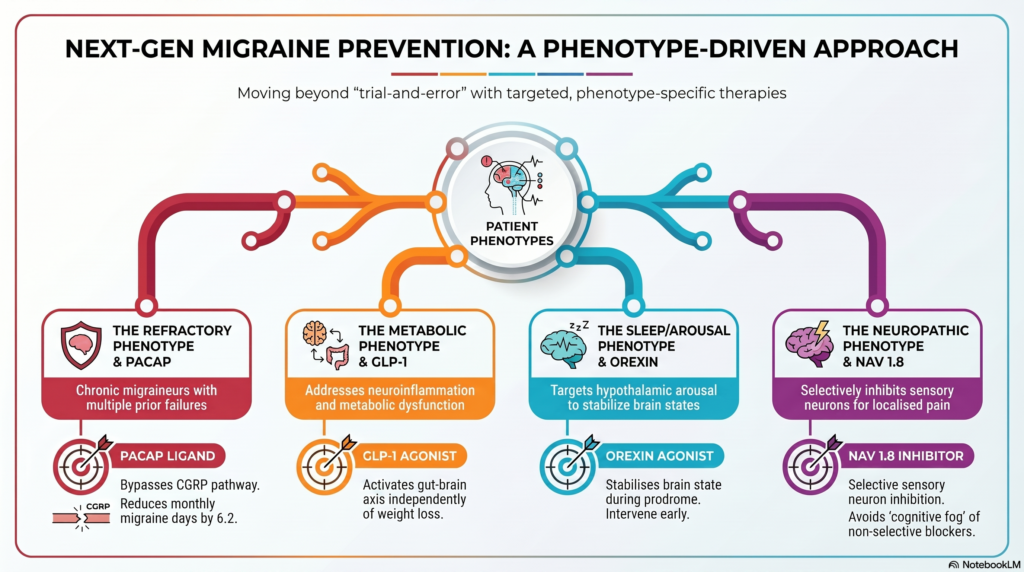
Despite the CGRP revolution in the last decade, the ‘non-responder’ remains a clinical challenge in our specialist clinics globally and beyond in primary care and pain clinics. In our specialist clinical practice, these patients probably represent one-third of all of our more chronic cases. For those who are refractory or partly responsive to CGRP-targeting, we must look to possible alternatives or additional treatments, and the next generation of molecular biology driven headache medicine (Figure 2). To this end, precision headache medicine utilises a strategy where therapeutic targets are dictated by a patient’s specific comorbidities (for example, hypertension, obesity, diabetes, obstructive sleep apnoea, and sleep disorders), individual migraine clinical features, response to prior preventives, and pain signatures. Current potential targets for novel molecular migraine treatments include the pituitary adenylate cyclase-activating polypeptide (PACAP), the Orexin system, glucagon-like peptide-1 (GLP-1) therapies, and selective sodium channel modulators.
The CGRP refractory phenotype and targeting the PACAP pathway
For patients who remain refractory or only partly responsive to CGRP-targeting treatments, the PACAP pathway is the most promising possible ‘next step’ or additional treatment. PACAP is a relatively distinct signalling pathway (especially upstream in the biochemical process) that does not rely on CGRP signalling, making it a potential target for those who fail or insufficiently respond to current CGRP therapies. Combining both CGRP and PACAP may also be an option in the future. Layering different complementary treatments is not uncommon in our clinical practice, especially for more treatment-refractory patients. The development of bocunebart, a PACAP-ligand monoclonal antibody (mAb), has provided additional clinical data for this difficult-to-treat population. The phase 2 and 2b data for bocunebart provide an evidence base for its use in migraine in general and possibly in CGRP-refractory cases:
▶ Chronic migraine data: In studies of patients who had failed two to four prior preventives (the general definition of ‘refractory’ migraine), a 750mg IV dose of bocunebart reduced monthly migraine days by 6.2 days (as compared to 4.2 for placebo).
▶ Episodic migraine/chronic migraine monthly dosing: A longer phase 2b study demonstrated that monthly dosing resulted in a reduction of 4.24 monthly migraine days (as compared to 2.86 days for placebo; p=0.0178) in patients who had failed one to four prior preventives.
▶ Quality-of-life and holistic outcomes: Beyond primary endpoints, bocunebart has shown a significant reduction in acute medication use and improved migraine-specific quality-of-life (MSQ) scores. Patient-reported outcome measures, such as MSQ, are one of the only ways we can measure improvement.
It is not clear yet as to the potential clinical impact of the PACAP therapies. However, the future looks very promising. For example, the identification of the ‘CGRP non-responder’ phenotype may be important. It may well be that therapeutic failure in one pathway (such as CGRP) does not preclude success in the PACAP pathway. We know that bocunebart offers a mechanism of action that is effective in patients who have already cycled through multiple existing preventive therapies, including CGRP-directed therapies in a small proportion of patients in the recent clinical trials (approximately 15 per cent). However, it remains an unanswered question as to whether CGRP treatment failures are more likely to respond to PACAP pathway inhibitors in a significant proportion of patients.
Beyond neuropeptides such as PACAP and CGRP, we are also discovering the potential importance of metabolic signalling in the migraine brain.
GLP-1 receptor agonists for potentially treating the migraine-associated metabolic phenotype
GLP-1 receptor agonists, widely known for managing diabetes and obesity, are emerging as potential anti-migraine therapeutics. Their possible strategic value lies in their ability to address neuroinflammation, metabolic dysfunction, and possibly additional centrally-mediated systems (such as addiction and dependency). Mechanistically, GLP-1 activation may target several migraine and/or headache drivers:
▶ Reduction of cerebrospinal fluid pressure.
▶ Gut-brain axis: Activation of the vagal nerve to improve signalling across the gut-brain axis.
▶ Cytokine regulation: Blocking inflammatory cytokines like IL-6 and TNF-α, which may modulate central nervous system pain hypersensitivity.
▶ CGRP interaction: Preliminary evidence suggests that GLP-1 treatments can decrease the expression of CGRP itself. The data remains promising but requires careful interpretation and replication.
The GLP-1 evidence to date is promising, but is unfortunately limited. For example, a small case series for liraglutide showed a 50 per cent reduction in migraine days, and this appeared to be independent of or regardless of weight loss. Conversely, case data for tirzepatide showed a clear correlation between drug cessation and migraine worsening. Again, we are dealing with small numbers which need to be replicated. Real-world, single-centre cohorts have also demonstrated reduced emergency department visits for patients on GLP-1 medications as compared to those on topiramate. For weight loss, it remains unclear if the migraine effect is truly independent across the class or if it is partially tied to anti-obesity effects. One hypothesis is that GLP-1 therapies may be particularly relevant for the patient who is a ‘partial responder’ to anti-CGRP therapy and possesses comorbid metabolic dysfunction, offering a dual-benefit profile. Add on or layering is always a clinical option to consider in patients with migraine and multiple other medical conditions.
The sleep/arousal phenotype: Orexins and circadian regulation
The Orexin system is a central regulator of the sleep-wake cycle and is also involved in trigeminal pain processing. For many patients, the migraine prodrome (and often other migraine phases in many of our patients) is defined by profound fatigue, suggesting that the hypothalamus and the Orexin system are possibly early participants in the migraine attack. Targeting the Orexin 1 receptor (Ox1R) holds promise for maintaining and stabilising the brain’s arousal state during the prodrome, potentially preventing the transition to a full-blown attack in an ideal scenario. In this proposed mechanism, sleep regulation is not a secondary concern, but it is a central component of migraine prevention. Therapeutic potential of OxA/Ox1R therefore includes:
▶ Arousal promotion: Activation of Ox1R may help reduce migraine-related fatigue and stabilise pain processing.
▶ Sex-specific mechanisms: Emerging research indicates potential sex-specific pathways in Orexin regulation, which may lead to more personalised, sex-based prescribing.
▶ Future directions: There is a critical need for the development of novel Ox1R agonists to hopefully extrapolate these findings into positive translational clinical studies. By targeting the Orexin system, the hope is to intervene during the prodrome.
The neuropathic pain phenotype: Selective sodium ion channel innovation
Non-specific sodium channel (NaV) modulators have long been standards of headache and migraine care. For example, we use carbamazepine for trigeminal neuralgia, lamotrigine for SUNCT/SUNA, topiramate for migraine prophylaxis, and IV valproate for status migrainosus. However, these non-selective agents often carry a heavy burden of systemic and cognitive side-effects, and may be ineffective in a significant proportion of patients. Suzetrigine, a selective NaV 1.8 inhibitor, represents a move towards higher efficacy and fewer side-effects:
▶ Mechanism of action: It selectively inhibits NaV 1.8, which is heavily expressed in the peripheral pain receptors and the trigeminal system. It regulates the excitability of small-diameter sensory neurons linked to neuropathic and inflammatory pain.
▶ Target population: Based on its mechanism of action, it might be considered for CGRP non-responders with localised head pain, sharp/electric sensations, or scalp/face tenderness.
▶ Current status caveats: It is important to note that suzetrigine has not yet been studied in headache in placebo-controlled trials and its restricted US FDA approval (for acute pain only) currently limits its use to specific case-by-case scenarios only. However, it appears that selective NaV 1.8 inhibition offers a significantly ‘cleaner’ clinical profile than our current options. By targeting the peripheral and trigeminal systems without affecting the channels throughout the rest of the central nervous system, suzetrigine potentially avoids the ‘cognitive fog’ or systemic side-effects that lead to the high discontinuation rates seen with topiramate.
Conclusion: Integrating the next generation of therapies The integration and combination of specific molecular treatments including CGRP therapies, PACAP ligands, GLP-1 agonists, Orexin modulators, and selective NaV inhibitors marks the definitive end of the ‘trial-and-error’ era. These therapies represent a seismic shift away from general suppression of the nervous system towards a sophisticated, molecular biology and phenotype-driven strategy. Layering of these specific molecular treatments should become the norm to improve the health of our patients. International guidelines have provided a mandate: Migraine-specific drugs must be our primary clinical choice to reduce the global burden of this disease. In addition, by matching the right molecular target to the right patient profile, we can finally offer true precision prevention for patients with additional medical problems. There has been a complete change in our practice in recent years, and this should continue to evolve and be supported by our health service for the good of our patients. The future of migraine care, and more widely headache care, is no longer a distant prospect; it is here.
References on request












Leave a Reply
You must be logged in to post a comment.