







Within the MMUH specialist headache service, structured pathways have facilitated suitable patient selection, safe delivery, and close monitoring of the latest transformative migraine therapies
Migraine is one of the most common neurological conditions, affecting 1.16 billion people with an age-standardised prevalence of 14.2 per cent.1 Despite being non-life-threatening, it is the second leading cause of disability worldwide and the leading cause among young women with a high burden of years lived with disability (YLDs).2 Migraine not only affects the patient’s quality-of-life (QoL), engagement in daily activities, and productivity at home and work, but is also associated with substantial societal and healthcare costs. QoL questionnaires such as MIDAS are often used to stratify the impact of migraine on daily functioning. The MIDAS score evaluates the number of days in the previous three months that migraine interfered with a person’s ability to engage in day-to-day activities (See Table 1). According to a US study of 7662 patients with migraine, patients with severe disability (MIDAS score >20) had around 42 per cent higher mean healthcare visit costs and over 50 per cent higher mean pharmacy costs compared to those with moderate disability (MIDAS score 11-20).3 Thus, greater level of disability in migraine leads to a more substantial economic impact.
According to the International Classification of Headache Disorders (ICHD-3), chronic migraine is a headache occurring on ≥15 days/month for more than three months with at least eight of these days having features typical of migraine.4 Episodic migraine is a similar headache, but happening less than 15 days/month. Studies have shown that episodic migraine may progress to chronic migraine at an estimated rate of 2.5 per cent per year, thereby increasing the disease burden.5 This transition is mainly attributed to medication exposure, especially barbiturates and opioids.
| MIDAS score | Grade | Disability level | Clinical meaning |
|---|---|---|---|
| 0–5 | I | Little or no disability | Minimal impact on daily life |
| 6-10 | II | Mild disability | Noticeable but limited impact |
| 11-20 | III | Moderate disability | Significant impact on daily activities |
| ≥21 | IV | Severe disability | Severe functional impairment, needs substantial care |
Table 1: Interpretation of MIDAS score
Conventional treatment for migraine
Moreover, the use of some conventional prophylactic therapies for chronic migraine is limited by contraindications and intolerability. Asthma may limit the use of beta blockers, while hypotension may render agents like candesartan unsuitable. Some patients are reluctant to take antidepressants like amitriptyline, dosulepin, venlafaxine, and nortriptyline. Antiepileptic drugs like topiramate may cause cognitive impairment and valproate leads to teratogenicity. Additionally, the adherence to these agents is often limited due to the delayed onset of action with slow titration over weeks to months. There is commonly an incomplete response leading to over utilisation of acute-headache-medications, which then causes a secondary headache called medication overuse headache (MoH). Excessive consumption of over-the-counter analgesia including NSAIDs, paracetamol, opioids, and even triptans causes a paradoxical worsening of the headache frequency and chronicity. The recurrent exposure to such drugs is believed to enhance central sensitisation and a self-perpetuating cycle of headache and medication use. Breaking this cycle is the cornerstone of the management of MoH. Abrupt withdrawal is recommended for non-opioids while tapering is necessary for opioids. This will undoubtedly cause transient worsening of symptoms, but must be followed by dose-adjustment of conventional preventives in order to alleviate the headache frequency and reliance on acute treatments. The entire process requires appropriate education and structured follow-up and if done inappropriately, may lead to failure of treatment. However, if done correctly, then many patients experience significant improvement over time.
For the above reasons, migraine is often thought to be difficult to treat, especially in inexperienced hands. Nonetheless, we have now entered a new era of calcitonin gene-related peptide (CGRP) monoclonal antibodies that have revolutionised migraine treatment.
Newer agents – CGRP targeted therapies
CGRP is a neuropeptide postulated to be involved in migraine pathophysiology.6 It is released from the trigeminovascular system during migraine attacks and leads to pain transmission, vasodilation and neurogenic inflammation. Small molecule CGRP receptor antagonists like atogepant and rimegepant are thus effective for acute migraine treatment while monoclonal antibodies against the CGRP receptor (erenumab) and the CGRP ligand (fremanezumab, galcanezumab and eptinezumab) have demonstrated favourable outcomes for chronic migraine prophylaxis.7 These agents inhibit CGRP-mediated signalling, thereby lowering the frequency and severity of migraine. Importantly, gepants can be used in triptan-unsuitable patients for the treatment of acute migraine attacks. Details about dosing in Table 2.
| Drug | Route | Dose | Duration |
|---|---|---|---|
| Eptinezumab | IV | 100mg or 300mg | Every 12 weeks |
| Erenumab | S/C | 70 – 140mg | Monthly |
| Fremanezumab | S/C | 225mg once monthly or 675mg every 12 weeks | Variable |
| Galcanezumab | S/C | 240mg loading then 120mg maintenance dose | Monthly |
| Rimegepant | PO | 75mg in acute attacks, 75mg on alternate days for prevention | Variable |
| Atogepant | PO | 10mg or 60mg during attacks or daily for prevention | Variable |
Table 2: Dosing guide about CGRP drugs. Adapted8,9
These CGRP-targeted therapies were introduced into clinical practice internationally in 2018 and then subsequently in Ireland over the next few years. They have limited side-effects due to their migraine-specific mechanism of action and a convenient dosing schedule, thus enhancing patient adherence. Most importantly, they are fairly rapid in achieving treatment response and do not require slow titration like the conventional therapies. Thus, they have completely transformed migraine treatment, delivering an effective modality for patients with acute and chronic difficult-to-treat migraine.
It is also essential to note some adverse effects and contraindications as mentioned in Table 3. These agents are safe in patients with stable cardiovascular disease, as they do not cause vasoconstriction, unlike triptans. However, caution is advised in acute cardiovascular conditions like recent myocardial infarction or stroke where CGRP may play a protective vascular role and due to limited clinical trial data in this scenario.
| Drug | Adverse effects | Contraindications |
|---|---|---|
| Eptinezumab |
|
Hypersensitivity |
| Erenumab |
|
Hypersensitivity |
| Fremanezumab |
|
Hypersensitivity |
| Galcanezumab |
|
Hypersensitivity |
| Rimegepant |
|
Hypersensitivity, Severe hepatic impairment, end-stage renal disease |
| Atogepant |
|
None |
Table 3: Side-effect profile of CGRP-targeted therapies. Adapted9
Eligibility for CGRP-targeted therapies
Even though the CGRP-targeted therapies have consistently demonstrated significant efficacy in migraine treatment/prevention across clinical trials and real-world studies, their relatively high procurement costs have prompted the introduction of reimbursement criteria in some healthcare systems. In Ireland, only approved consultants can apply for reimbursement under the HSE managed access protocols (MAP) on an individual patient basis through the Primary Care Reimbursement Service (PCRS). The eligibility criteria include failure of three or more conventional treatments with reimbursement supported for atogepant, erenumab, galcanezumab, fremanezumab, and eptinezumab for chronic migraine prophylaxis and atogepant and rimegepant for treatment of episodic migraine. However, rimegepant is available through private prescription for acute migraine as well. The strict criteria aim to balance clinical gain with cost-effectiveness and judicious use of resources.
Headache service at MMUH
Given these eligibility criteria, specialist headache services are crucial to ensure safe delivery of migraine-specific treatment to the right patient population. At the Mater Misericordiae University Hospital (MMUH), we have a dedicated tertiary headache service consisting of two consultants, three specialist nurses, and two to three registrars who ensure smooth running of the weekly consultant-led headache clinic. There is also a direct-access telephone line available to patients attending our clinic, allowing them to contact the service with queries or concerns during the working week. The line is managed by our specialist headache nurses, who provide advice and support directly or, where necessary, liaise with the consultant neurologist before responding. In addition, our specialist nurses run dedicated nurse-led clinics providing follow-up care, treatment monitoring, patient education, and support for patients receiving migraine therapies.
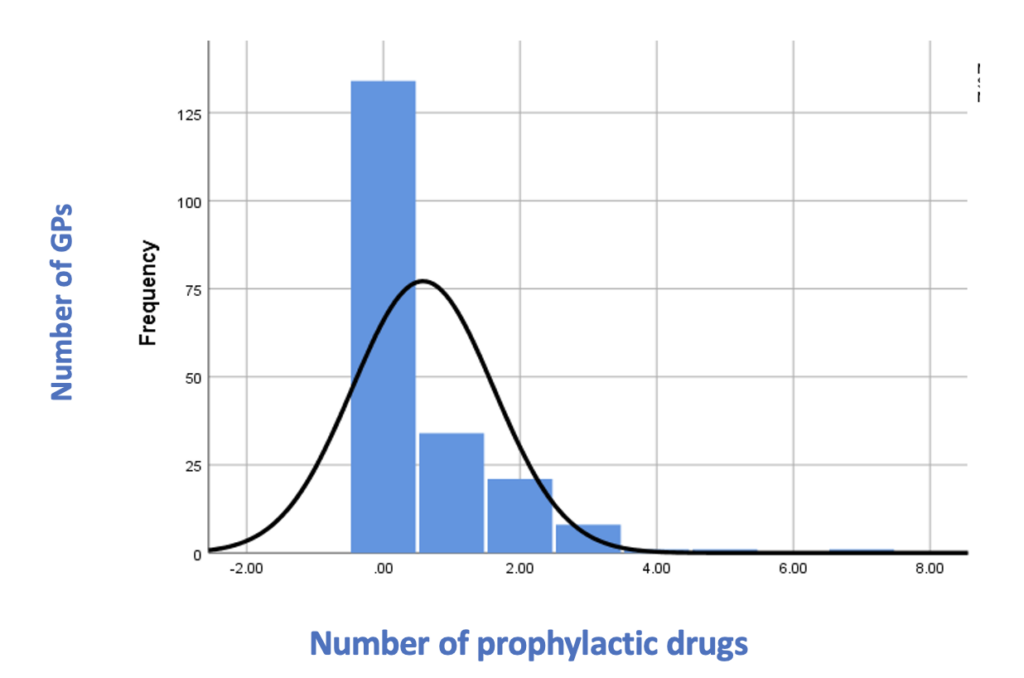
Patients with a broad range of headache-related conditions are seen in this clinic. According to a previous audit at MMUH, 1,073 patients with primary headache conditions attended in 12 months, with a large proportion (80 per cent) being female. Of these, 77 per cent were referred by GPs, thus constituting the major source of referral. About two-thirds were return patients, while one-third were new in the clinic. A small minority (2 per cent) attended for procedures like greater occipital nerve (GON) block which is used to treat both acute and chronic migraine. Of the total patients, 40 per cent had episodic migraine, 40 per cent had chronic migraine, and 20 per cent had other primary headache disorders (see Figure 1). Importantly, 70 per cent of the patients had not tried a conventional prophylactic agent before being referred to the neurology service (see Figure 2). It was also observed that triptans were underutilised for the acute management of migraine although they have been available for the past 30 years. The vast majority of patients (93 per cent) were followed up in clinic subsequently. Following this audit, a GP headache pathway has been implemented at MMUH where patients who have failed at least two conventional prophylactic agents will be listed to be seen in our headache clinic. Referrals that do not meet these criteria are redirected back to the GP with guidance on how to manage in primary care. This includes details about diagnostic criteria of primary headache disorders; their acute and prophylactic management options, as well as red flags and referral parameters. The rationale behind this GP headache pathway was to reduce the OPD waiting list numbers and times. The re-audit after implementation of this pathway showed 36 per cent of referrals being redirected back to GPs and the discharge rate from the clinic tripled. Notably, the waiting time to be seen in clinic reduced. In addition, the introduction of nurse-led headache clinics for follow-up patients has led to more new patients being seen in consultant-led clinics.
Figure 1: Diagnoses of patients being seen in the headache clinic at MMUH
There is a dire need for such pathways to accommodate the growing demand of specialist neurology services. According to the latest data available on the HSE website, there are currently approximately 26,000 patients waiting to be seen in neurology outpatient services.10 Of these, around 3800 (14.6 per cent of the total) are waiting to be seen in MMUH. Due to such large numbers, there is significant delay in the time-to-first appointment. To address this issue, a designated ‘long waiters’ clinic was initiated at MMUH in February 2025. After one year of the successful implementation of this clinic, waiting times were substantially reduced from up to five years to around 18 months. This is still an ongoing clinic so waiting times are expected to reduce even further as time passes.
Once reviewed in the headache clinic, patients undergo a detailed assessment of their headache characteristics, treatment history, and migraine-related disability, which then leads to subsequent management decisions including eligibility for advanced treatment including CGRP-targeted therapies. As these high-cost medications are regulated by the HSE MAP, the patient selection criteria revolves around definite diagnosis of migraine, significant disease burden, and failure of at least three traditional prophylactic medications. Once these criteria are met and there are no contraindications to the use of CGRP-targeted therapies (as mentioned in Table 2), then the consultant sends the application through the PCRS. It usually takes about one to two weeks for the actual treatment to start.
Currently, more than 300 patients at MMUH have received this migraine-specific treatment that includes oral medications like atogepant, subcutaneous injections like erenumab, galcanezumab, and fremanezumab, as well as intravenous injections of eptinezumab. Thus, we have a large cohort of patients with highly disabling migraine. Such patients are monitored very closely by our specialist headache nurses to assess treatment response as well as tolerability. If any issue arises which cannot be resolved through the direct telephone lines, then they are given an early follow-up appointment in the consultant-led clinic.
Real-world experience with eptinezumab
We have seen a relatively positive treatment outcome following CGRP initiation in our patients. A real-world study is currently ongoing at our headache service to assess effectiveness of eptinezumab through patient-reported outcomes. Eptinezumab was approved for chronic migraine internationally in 2022 and received HSE reimbursement approval a year later. Delivery of eptinezumab requires dedicated nursing and infusion unit resources, particularly during the initial treatment phase, after which ongoing administration can transition into the community setting.
Our patient population represents a super-refractory cohort of chronic migraine who have not only failed at least three conventional preventative therapies, but also another alternative CGRP-targeted therapy. Such a cohort is usually excluded from clinical trials so there is an unmet need to evaluate their treatment response.
Conclusion
Migraine is a highly prevalent and disabling disease with a huge individual and societal impact. While conventional preventive therapies are usually limited by tolerability, slow onset of action and incomplete response, CGRP-targeted therapies represent a notable therapeutic revolution with better effectiveness and tolerability. Yet, these novel therapies have underscored the urgent need for structured specialist pathways to ensure appropriate patient selection and management while ensuring adequate utilisation of outpatient neurology services. Such service redesign is imperative to ensure timely access to effective therapies for patients with disabling migraine. Within the MMUH headache service, structured pathways have facilitated suitable patient selection, safe delivery, and close monitoring in routine clinical practice.
References
- Steinmetz J, Seeher K, Schiess N, et al. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024;23:344-381
- Chen ZF, Kong XM, Yang CH, et al. Global, regional, and national burden and trends of migraine among youths and young adults aged 15-39 years from 1990 to 2021: Findings from the Global Burden of Disease Study 2021. J Headache Pain. 2024;25:131
- Harris L, L’Italien G, Kumar A, et al. Real-world assessment of the relationship between migraine-related disability and healthcare costs in the US. Headache. 2022;62:473-481
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (ICHD-3). Cephalalgia. 2018;38(1):1-211
- Bigal ME, Serrano D, Buse D, et al. Acute migraine medications and evolution from episodic to chronic migraine: A longitudinal population-based study. Headache. 2008;48:1157-1168
- Edvinsson L, Warfvinge K. Recognising the role of CGRP and CGRP receptors in migraine and its treatment. Cephalalgia. 2019;39(3):366-373
- Edvinsson L. CGRP and migraine: From bench to bedside. Rev Neurol (Paris). 2021;177(7):785-790
- Sacco S, Amin FM, Ashina M, et al. European Headache Federation guideline on the use of monoclonal antibodies targeting the calcitonin gene-related peptide pathway for migraine prevention: 2022 update. J Headache Pain. 2022;23:67
- Özge A, Baykan B, Bıçakçı Ş, et al. Revolutionising migraine management: Advances and challenges in CGRP-targeted therapies and their clinical implications. Front Neurol. 2024;15:1402569
- Health Service Executive. National waiting list data [Internet]. Dublin: Health Service Executive; [cited 2026 Mar 27]. Available at: www2.hse.ie/services/activity-performance-data/waiting-for-care/waiting-lists/national












Leave a Reply
You must be logged in to post a comment.