






Reference: October 2025 | Issue 10 | Vol 11 | Page 42
Influenza, commonly referred to as the flu, is a highly contagious and communicable respiratory illness caused by influenza viruses. There are four types of influenza viruses, A, B, C, and D. Influenza types A and B cause human infection annually and are notable for their ability to cause seasonal epidemics and, occasionally, pandemics, leading to significant morbidity and mortality worldwide.
Influenza viruses spread through respiratory droplets released when a person coughs, talks, or sneezes. They can also be transmitted if people touch surfaces contaminated with the virus and then touch their nose, mouth, or eyes. A person with influenza can spread the virus even before they show symptoms and continue to do so for five to seven days after becoming infected. Following an infection, most healthy individuals recover in seven to 10 days. However, complications such as pneumonia and death are more prevalent among certain high risk groups.1
Those at higher risk of experiencing severe illness or complications from an influenza infection include pregnant women, children under five years of age, the elderly, people with chronic medical conditions such as heart, lung, kidney, metabolic, neurodevelopmental, liver, or blood disorders, and individuals with compromised immune systems such as those with HIV, those undergoing chemotherapy or steroid treatment, or those dealing with malignancies. Healthcare workers have an increased risk of contracting the influenza virus due to their frequent exposure to patients, which also increases the likelihood of spreading the virus to vulnerable populations.1,2
Epidemiology
Globally, influenza creates a significant burden on healthcare systems. According to the World Health Organization (WHO), there are around a billion cases of seasonal globally per year, including three to five million cases of severe illness and between 290,000 to 650,000 respiratory deaths. Influenza A and B viruses are primarily responsible for these seasonal epidemics, while influenza A viruses also have the potential to cause pandemics due to their ability to undergo significant genetic changes.2
In Ireland, the Health Protection Surveillance Centre (HPSC) is responsible for monitoring influenza activity through a comprehensive national surveillance system. The influenza season in Ireland runs from October to May, with peak activity often observed between December and February, impacting the healthcare system with increased hospital admissions and extra pressure on general practice services.3
Trends in Ireland
The period from 2019 to 2024 saw significant changes in influenza activity in Ireland, influenced largely by the Covid-19 pandemic and the resultant public health measures.3 During the 2019-2020 influenza season, Ireland experienced over 4,000 laboratory-confirmed cases of influenza. The HPSC reported peak influenza-like illness (ILI) rates in January. This season was marked by a substantial number of hospital admissions due to influenza complications, particularly affecting vulnerable populations such as the elderly and those with underlying health conditions.3
The 2020-2021 influenza season was unprecedented due to the Covid-19 pandemic. Public health interventions aimed at controlling Covid-19 such as lockdowns, social distancing, mask mandates, and enhanced hygiene practices significantly reduced influenza transmission. Consequently, the HPSC reported historically low influenza levels, with minimal laboratory-confirmed cases and reduced ILI rates. The stringent measures, although primarily targeting Covid-19, effectively curtailed the spread of influenza.
Additionally, there was an increased uptake of the influenza vaccine driven by heightened public awareness of respiratory illnesses, resulting in higher vaccination rates among high risk groups compared to previous seasons. Ireland had the highest vaccination rate in the EU, with 75.4 per cent of people over 65 being vaccinated against influenza in 2021.3
As Covid-19 restrictions eased during the 2021-2022 influenza season, there was concern about the potential resurgence of influenza. The HPSC observed a gradual increase in influenza activity, though it remained below pre-pandemic levels. The partial resurgence was mitigated by ongoing public health practices and vaccination efforts.
The HPSC reported sustained high vaccine uptake rates, particularly focusing on high risk groups. The flu vaccine campaign was integrated with Covid-19 vaccination efforts to maximise coverage. The simultaneous presence of Covid-19 and influenza posed diagnostic challenges, necessitating increased reliance on laboratory testing to differentiate between the two infections.3
During the 2022-2023 season, influenza activity in Ireland normalised as public health measures for Covid-19 were largely relaxed. The HPSC emphasised maintaining vigilance and vaccination coverage. Influenza activity returned closer to pre-pandemic levels, with a significant number of laboratory-confirmed cases and increased ILI rates.
Enhanced surveillance measures were implemented to track influenza and other respiratory viruses, involving greater collaboration with healthcare providers and public health laboratories. While vaccine uptake remained strong, there was a slight decline compared to the previous season, prompting the HPSC to continue advocating for vaccination, especially among high risk populations.3
The 2023-2024 influenza season was notable for several developments, including updated vaccination eligibility and an ongoing emphasis on public health preparedness. The HPSC expanded the criteria for free influenza vaccination to include children aged two to 17 years, individuals with a body mass index (BMI) over 40, residents of long-term care facilities, and carers or household contacts of vulnerable individuals. This expansion aimed to increase overall vaccine coverage and reduce the transmission of influenza among high risk groups.3
Generally, the flu vaccine is available free of charge for:
- All persons aged 60 years and over
- Children aged two to 17
- Pregnant individuals
- Patients aged six to 23 months and 18 to 64 years at increased risk of flu-related complications
- Residents of nursing homes and other long-stay facilities
- Healthcare workers
- Household contacts of people with underlying conditions or Down syndrome
- Out-of-home care givers for people who have an underlying chronic health condition or have Down syndrome.4
and immunocompromised
Pathophysiology
Influenza viruses are single-stranded RNA viruses belonging to the orthomyxoviridae family. They primarily infect the epithelial cells of the respiratory tract. Influenza A viruses are further classified into subtypes based on two surface proteins – haemagglutinin (HA) and neuraminidase (NA). There are 18 HA and 11 NA subtypes, with H1N1 and H3N2 being the most common subtypes causing human infections.1,5
The virus spreads primarily through respiratory droplets when an infected person coughs, sneezes, or talks. It can also spread by touching surfaces contaminated with the virus and then touching your mouth, nose, or eyes. After an incubation period of one to four days, symptoms typically begin abruptly.
Influenza viruses have a remarkable ability to undergo genetic changes, including antigenic drift and shift. Antigenic drift involves minor changes in the HA and NA proteins, leading to seasonal epidemics. Antigenic shift, on the other hand, involves a major change in the HA and/or NA proteins, potentially resulting in a new influenza A subtype and leading to pandemics.1,5
Presentation
Influenza presents with a wide range of symptoms, from mild to severe. The clinical presentation often includes the sudden onset of high fever, chills, sweats, headache, myalgia, fatigue, and weakness. Respiratory symptoms such as nasal congestion, sore throat, and a severe cough are also common. Gastrointestinal symptoms such as nausea, vomiting, and diarrhoea may occur, especially in children.1,6,7
Complications of influenza can be severe and include viral pneumonia, secondary bacterial pneumonia, sinus infections, and exacerbation of chronic medical conditions such as asthma, chronic obstructive pulmonary disease, and cardiovascular disease. Vigilance is necessary in populations at higher risk for complications, including young children, the elderly, pregnant women, and individuals with underlying health conditions.1,6,7
Diagnosis
The diagnosis of influenza is primarily clinical, based on the presence of typical signs and symptoms during the influenza season. However, laboratory testing can confirm the diagnosis and is particularly useful during outbreaks or for patients with severe disease.1,2,6,7
Several diagnostic methods are available. Rapid influenza diagnostic tests detect viral antigens in respiratory specimens and provide results within 15-to-30 minutes. While convenient, they have variable sensitivity and may produce false-negative results.
Reverse transcription polymerase chain reaction (RT-PCR) is the most sensitive and specific method for detecting influenza viruses. It can differentiate between influenza A and B and identify specific subtypes. Results are typically available within a few hours to a few days.
Viral culture involves growing the virus from respiratory specimens in cell culture. While highly specific, it is time-consuming and results may take several days. Immunofluorescence assays detect viral antigens using fluorescent-labelled antibodies and they require specialised equipment and expertise.
In clinical practice, RT-PCR is often the preferred diagnostic method due to its high sensitivity and specificity. A chest x-ray should be obtained in patients with pulmonary symptoms to exclude bacterial pneumonia.1,2,6,7
Treatment
The treatment of influenza includes antiviral medications and supportive care. Initiating antiviral treatment within 36-48 hours of symptom onset for at-risk groups can lower the risk of influenza complications, such as otitis media in young children, pneumonia, and respiratory failure. It can also shorten the duration of illness in acutely ill patients and reduce morbidity, hospitalisation, and mortality in those with severe infections.
Symptomatic treatment, however, is the recommended approach for previously healthy individuals, excluding pregnant women, unless the clinician believes the patient is very ill or at high risk for influenza complications.8
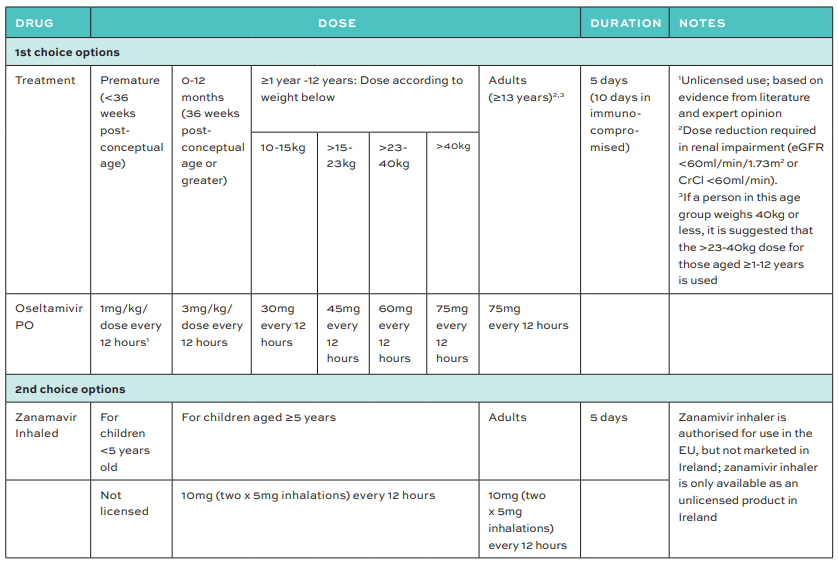
Two antiviral medications are recommended for use in Ireland during the influenza season – oral oseltamivir and inhaled zanamivir. These antiviral NA inhibitors exert activity against seasonal influenza A and B. NA inhibitors block the release of new virions from infected cells. Oseltamivir is the most used antiviral and is approved for treatment and prophylaxis of influenza in individuals aged one year and older. Zanamivir is recommended for patients who cannot take oral medications or for those with oseltamivir-resistant strains.
Antivirals are recommended for pregnant women due to the adverse clinical outcomes that have been observed for influenza in this group. Oseltamivir is the first-line option for most pregnant women with influenza, including during seasons that are dominated by influenza A (H1N1).8
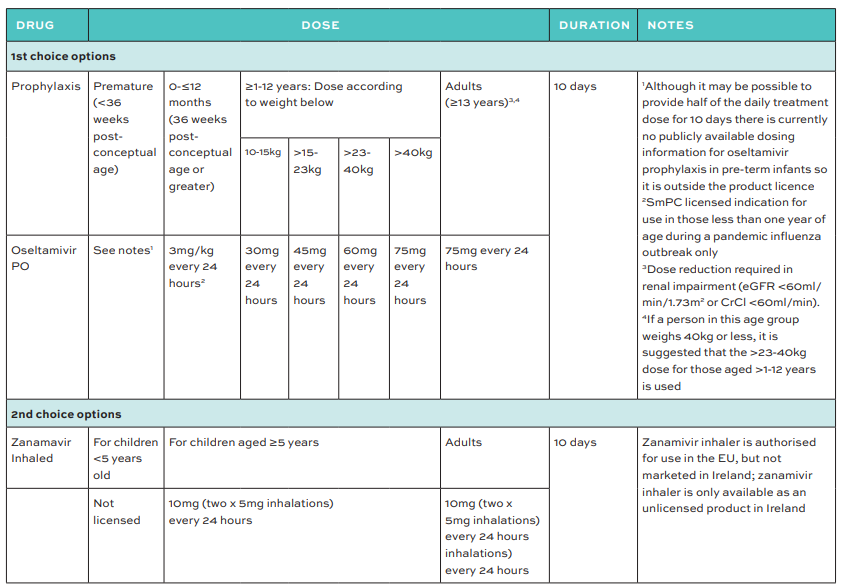
Chemoprophylaxis should be reserved for at-risk individuals who have recently been in close contact with someone with influenza or an influenza-like illness within the same household or residential setting. Prior influenza vaccination does not rule out the use of post-exposure prophylaxis, especially in cases of localised outbreaks in residential care facilities.
Supportive care includes maintaining adequate hydration, rest, and the use of over-the-counter medications to relieve symptoms. For severe cases, hospitalisation may be required, and supportive measures such as oxygen therapy, mechanical ventilation, and treatment of secondary bacterial infections may be necessary.
Prevention
Preventing influenza relies on vaccination, good respiratory hygiene, and public health measures. The most effective way to prevent influenza is through annual vaccination. The seasonal flu vaccine is updated each year to match circulating strains based on recommendations from the WHO. The vaccine is available in two forms: Inactivated influenza vaccine (IIV) and live attenuated influenza vaccine (LAIV).2,6
In Ireland, the HSE provides free flu vaccines to high risk groups, including individuals aged 60 and over (2024/2025 season), pregnant women, healthcare workers, and people with chronic medical conditions. Children aged two to 17 years are eligible for a free nasal spray flu vaccine, recognising the significant role children play in the transmission of influenza. As mentioned, individuals with a BMI over 40, residents of long-term care facilities, and carers or household contacts of vulnerable individuals are also included in the free vaccination programme.4
Other preventive measures include good respiratory hygiene, such as covering the mouth and nose with a tissue or elbow when coughing or sneezing, frequent hand washing with soap and water, and the use of alcohol-based hand sanitisers. During peak flu season, avoiding close contact with infected individuals and wearing masks in crowded or high-risk settings can further reduce the spread of the virus.2,6,8
Recent developments
The landscape of influenza management is continuously evolving, with several recent developments and ongoing challenges influencing public health strategies.2
The Covid-19 pandemic had a profound impact on influenza activity and surveillance. Public health measures implemented to control Covid-19 significantly reduced influenza transmission globally and in Ireland. However, the co-circulation of Covid-19 and influenza viruses posed substantial challenges for diagnosis, treatment, and vaccination efforts, therefore, the healthcare system had to adapt to managing both infections simultaneously, ensuring adequate resources and timely interventions for affected individuals.3
Improving vaccine uptake remains a critical goal. The 2020-2021 influenza season saw increased vaccination rates due to heightened awareness following the Covid-19 pandemic. Sustaining high vaccination rates in subsequent seasons is essential to protect vulnerable populations and prevent severe influenza outcomes.
Public health campaigns emphasising the importance of annual flu vaccination and addressing vaccine hesitancy are vital. The expansion of free vaccination criteria aims to increase coverage, particularly among high risk groups.3,4
Antiviral resistance
The emergence of antiviral-resistant influenza strains is a growing concern. Continuous monitoring and research are necessary to identify resistant strains and develop new antiviral agents. Potential strategies include combination antiviral therapy and the development of broad-spectrum antivirals to enhance treatment efficacy and reduce the risk of resistance.2,9
Universal flu vaccine
Research is ongoing to develop a universal influenza vaccine that provides long-lasting protection against multiple strains. Such a vaccine would significantly enhance the ability to prevent influenza and reduce the need for annual vaccination. Advances in understanding the immune response to influenza and novel vaccine technologies hold promise for the future, and could potentially revolutionise influenza prevention.
Promising strategies involve targeting conserved influenza virus regions such as HA, NA, the M2 extracellular domain, and internal proteins. The discovery of broadly neutralising antibodies against conserved HA regions has provided important insight into novel vaccine designs and platforms.9,10
Conclusion
Influenza remains a significant public health concern, causing substantial morbidity and mortality each year. In Ireland, the HPSC plays a significant role in monitoring and responding to influenza activity. Efforts to enhance surveillance, increase vaccination rates, and educate the public on preventive measures are important to mitigate the impact of influenza.
The expansion of free vaccination is a positive development, aimed at protecting more high-risk individuals from the disease. Ongoing research and international collaboration are essential to address the evolving challenges posed by influenza and improve public health outcomes.
References
- Boktor SW, Hafner JW. Influenza. [Updated 2023 Jan 23]. In: StatPearls [Internet]. Treasure Island: StatPearls Publishing; 2024. Available at: www.ncbi.nlm.nih.gov/books/NBK459363/.
- World Health Organization. Influenza (Seasonally). Geneva: WHO; 2024. Available at: www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
- Health Protection Surveillance Centre. Influenza surveillance. Ireland: HPSC; 2024. Available at: www.hpsc.ie/az/respiratory/influenza/seasonalinfluenza/surveillance/.
- Department of Health. Minister for Health announces expanded seasonal flu vaccination programme for 2024/2025. Roinn Sláinte. Available at: www.gov.ie/en/press-release/d3659-minister-for-health-announces-expanded-seasonal-flu-vaccination-programme-for-20242025/.
- Uyeki T, Hui D, Zambon M, et al. Influenza. The Lancet. 2022; 400(10355):693-705.
- Health Service Executive. Influenza. Ireland: HSE; 2023. Available at: www2.hse.ie/conditions/flu/symptoms-diagnosis/.
- Medscape [internet]. Influenza: Clinical presentation. 2024. Available at: https://emedicine.medscape.com/article/219557-clinical.
- HSE antiobiotic prescribing (2024). Influenza (Seasonal). Health Service Executive, Ireland. Available at: www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/influenza/.
- Duncan D. Influenza, vaccines, and new developments. Practice Nursing. 2024;35(5).
- Lim CML, Komarasamy TV, Adnan NAAB, et al. Recent advances, approaches, and challenges in the development of universal influenza vaccines. Influenza Other Respir Viruses. 2024;18(3):e13276. doi: 10.1111/irv.13276.
