NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Jurie Mostert and Prof Glen Doherty
- 18th Aug 2025
iStock.com/wildpixel
This module gives a detailed overview of the latest diagnosis and medical treatment approaches to the management of Crohn’s disease, alongside a typical case study to illustrate the presentation of the disease
Case study
A 22-year-old male university student presents with a three-month history of intermittent abdominal pain, non-bloody diarrhoea occurring four to five times daily, unintentional weight loss of 6kg, and fatigue. There is no significant past medical history, but he mentions a family history of Crohn’s disease affecting his mother. He is a smoker of approximately five-10 cigarettes a day. There is no recent travel history of note.
Physical examination reveals a pale, underweight patient with mild tenderness in the right lower quadrant of the abdomen. No perianal disease is noted.
Initial blood tests show anaemia (Hb 10.2 g/dL), elevated CRP, and hypoalbuminaemia. Faecal calprotectin is elevated. Stool tests are negative for infectious causes, including Clostridium difficile.
A colonoscopy reveals areas of patchy inflammation with aphthous ulcers and skip lesions, particularly in the terminal ileum.
Crohn’s disease (CD) is a chronic, immune-mediated inflammatory disorder that can affect any part of the gastrointestinal (GI) tract and may present with extraintestinal manifestations. Gastrointestinal involvement can lead to complications such as fibrotic strictures, fistulas, and abscesses. Along with ulcerative colitis (UC), it is considered one of the two major types of inflammatory bowel disease (IBD).
Epidemiology
IBD is a global disease, with Western nations exhibiting the highest prevalence rates. Newly industrialised nations are experiencing the largest increases in incidence. More than 1.5 million people in North America and two million people in Europe are affected by IBD, while the burden of the disease outside Western countries, including Sub-Saharan Africa, remains unclear.
There are no validated data on the current incidence and prevalence of IBD in Ireland, but based on recent studies in the Scottish population (who share similar genetic and dietary/environmental characteristics), we can estimate population prevalence of IBD now exceeds 0.8 per cent of the population and will likely reach 1 per cent by 2030.
CD shows a bimodal incidence pattern, with a median onset of disease between 20-30 years and a smaller peak at the age of 50 years. Over 80 per cent of CD patients are diagnosed before the age of 40 years. It appears to be slightly more common in women.
Aetiology
The aetiology of CD is complex, involving an interaction between genetic, environmental, microbial, and immune factors that trigger the disease process.
Genetic: Studies have shown a significant heritable risk, particularly in twin studies, where a sibling with CD confers a 26-fold increased risk of developing the disease.
Microbiota: Alterations in the intestinal microbiome have been implicated in the development of IBD.
Environmental: Smoking is a well-established risk factor for CD onset and is the most studied risk factor. Both current and former smokers are at increased risk. Smoking can influence disease phenotype, leading to a higher incidence of stenosing, penetrating, and perianal disease, as well as ileal disease compared to colonic disease. It also negatively impacts treatment response, with smokers having a higher risk of requiring steroids and immunosuppressive treatments, as well as a decreased response to infliximab. Smokers are also more likely to present with extraintestinal manifestations (EIMs) than non-smokers.
Other risk factors: Non-steroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, and hormone replacement therapy may increase the risk for IBD, with NSAIDs being particularly significant among women. Diets high in fats, omega-6 fatty acids, meat, and ultra-processed foods are associated with an increased risk, while diets rich in fibre and fruits are linked to a decreased risk.
Disease classification and course
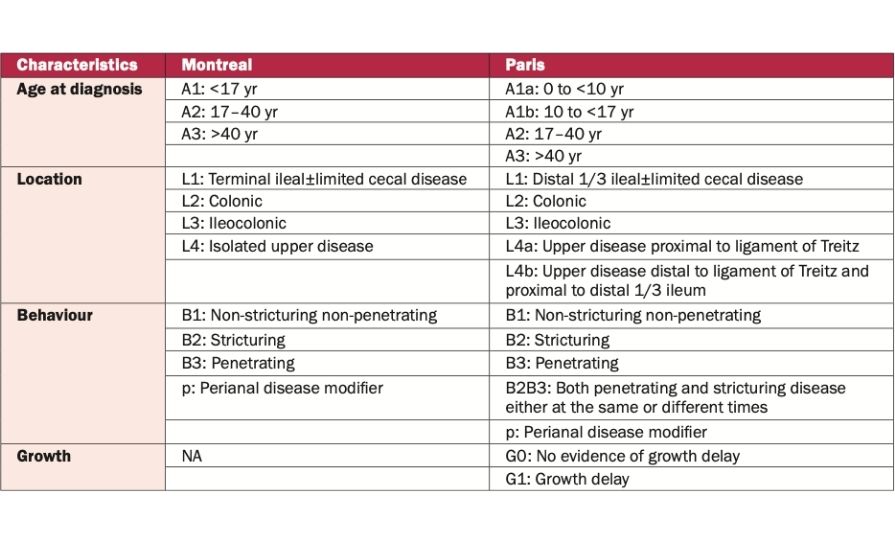
The clinical phenotype of CD is classified according to the Montreal and Paris classification systems (see Table 1).
Table 1: Montreal and Paris Classification of CD
CD tends to take a more aggressive course in children and adolescents compared to adults and the elderly, with EIMs being more common in younger patients.
The clinical course can be categorised into stricturing disease, aggressive fistulising disease, or indolent disease, where none of the subtypes develop over a long period of observation. It is important to note that a patient can exhibit both stricturing and fistulising disease simultaneously.
CD disease course:
50 per cent of CD patients have both terminal ileal and colonic involvement.
30 per cent have small bowel involvement.
20 per cent of cases are isolated to the small bowel.
25 per cent of patients experience perianal complications.
Clinical features
The clinical features of CD are diverse, and symptoms may be present for an extended period before a diagnosis is made.
The most common symptoms are diarrhoea and/or abdominal pain. These may be accompanied by systemic symptoms such as weight loss, low-grade fever, and fatigue.
Fatigue affects 30-50 per cent of IBD patients in clinical remission and more than 80 per cent of those with active disease.
In less than 10 per cent of patients, extraintestinal manifestations, isolated perianal complications such as fistulas and abscesses, or upper GI disease may be the presenting features.
Complications can lead to various initial complaints. Intestinal strictures can cause symptoms of bowel obstruction (eg, abdominal pain, nausea, and vomiting) or less severe symptoms like hyperactive bowel sounds. Penetrating disease may result in fistula formation.
Extraintestinal manifestations
EIMs can present before or after the diagnosis of IBD and may be dependent or independent of disease activity.Recognising these EIMs is important as it can shorten the diagnostic delay of IBD.
Most EIMs are associated with disease activity, except for axial arthropathy, primary sclerosing cholangitis (PSC), uveitis, and pyoderma gangrenosum. These manifestations can occur without significant abdominal symptoms.
Musculoskeletal: Musculoskeletal manifestations are the most common EIMs and are classified as spondyloarthropathies (formerly known as seronegative arthritides). Arthritis affects up to 25 per cent of patients with CD. It can affect both the axial skeleton and peripheral joints. Peripheral joint involvement can be classified into type 1 and type 2 arthropathy:
●Type 1: Oligoarticular (less than five joints), typically involving large joints, and associated with disease activity.
●Type 2: Symmetrical polyarticular involvement, unrelated to disease activity.
●Axial arthritis: Includes ankylosing spondylitis and sacroiliitis and can be either symptomatic or asymptomatic.
Skin: Skin involvement is the second most common EIM in IBD, affecting 5-15 per cent of patients.
●Erythema nodosum: Tender nodules on the anterior tibia, linked to active disease, and resolves without scarring.
●Pyoderma gangrenosum: Begins as pustules or nodules that progress to ulcers, usually on the legs, and is not linked to disease activity.
●Other skin manifestations include Sweet’s syndrome and cheilitis granulomatosa.
Eyes: Eye involvement is the third most common EIM in IBD.
●Episcleritis is the most common and linked to disease activity.
●Scleritis is rare, but can lead to vision loss.
●Uveitis is more common in CD and is unrelated to disease activity.
Vascular: There is a three-fold increased risk of venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and splanchnic thrombosis.
Hepatobiliary: Less commonly, CD can be associated with pancreatitis and hepatitis, which should be differentiated from drug-induced causes. PSC is more common in patients with UC, but can also occur in CD with colonic involvement.
Diagnosis
There is no single diagnostic test for CD. Diagnosis relies on a combination of clinical, biochemical, stool, endoscopic, radiological, and histological findings.
Gastrointestinal infections, particularly Clostridium difficile (C difficile) and parasites, must first be excluded. Intestinal tuberculosis should also be ruled out, especially in patients with a history of recent travel to TB-endemic countries, as its symptoms overlap significantly with CD.
Biochemical markers include elevated C-reactive protein (CRP), leukocytosis, anaemia, thrombocytosis, and low albumin. Faecal calprotectin (FCAL) is helpful for both diagnosis and monitoring disease activity. While serological markers such as ASCA and pANCA have some value, they are not diagnostic for CD.
Endoscopy
Ileocolonoscopy remains a key diagnostic tool in CD. At least two biopsies should be taken from any inflamed regions. Findings suggestive of CD include areas of inflammation such as aphthous erosions, discrete linear ulcers, and mucosal oedema, often interspersed with areas of normal-appearing mucosa, known as ‘skip lesions’. Depending on the disease behaviour, luminal narrowing due to strictures or fistulas may also be observed.
Upper GI endoscopy should be performed in patients with CD who have upper GI symptoms, those in whom lower endoscopy is inconclusive, or when concomitant Coeliac disease is suspected.
Small bowel disease
Small bowel disease is often more difficult to diagnose. In suspected cases, imaging modalities such as intestinal ultrasound, CT enterography, and magnetic resonance enterography are useful. These imaging techniques allow visualisation of the bowel wall, identification of extraluminal complications, and monitoring of treatment efficacy. While sensitivity is generally similar among these modalities, magnetic resonance enterography and intestinal ultrasound are preferred due to their lower radiation exposure.
Capsule endoscopy is highly sensitive in detecting abnormal mucosa, but has low specificity for diagnosing CD.
Histology
Histological findings may include non-caseating granulomas, but more commonly include inflammatory infiltrates, crypt distortion, and Paneth cell metaplasia.
Treatment
The treatment of CD involves both medical and surgical management. The primary goals of treatment are to induce and maintain steroid-free remission while preventing complications and the need for surgery. Surgical intervention is generally reserved for patients who fail to respond to medical treatment or those who develop complications that can only be treated surgically.
In 2024 the European Crohn’s and Colitis Organisation published updated evidence-based consensus guidelines on the management of CD. The first document covers medical management and the second addresses surgical management, including preoperative aspects and drug management before surgery. It also provides technical advice for a variety of common clinical situations.
Corticosteroids
Steroids are reserved for induction therapy and have no place in maintenance due to their adverse effects. Two steroid options are available: Locally-acting budesonide and systemic steroids. Locally-acting steroids have a more favourable side-effect profile, but are typically used for active disease involving the ileum and ascending colon.
Immunomodulators
5-Aminosalicylates have no role in the management of CD due to consistent evidence of lack of efficacy.
Methotrexate was once used for both induction and maintenance therapy, but has fallen out of favour due to the availability of more effective drugs.
Thiopurines are still used in maintenance therapy, often in combination with infliximab. This combination has the added benefit of reducing the risk of developing drug antibodies, which can impair treatment efficacy.
Biologic therapy
Anti-TNF agents
●Infliximab, a monoclonal antibody against TNF-α, was the first biologic approved for CD treatment. It is available in both intravenous and subcutaneous forms and is approved for both induction and maintenance therapy. Combination therapy with azathioprine has been shown to be more effective.
●Adalimumab is a fully humanised IgG1 antibody against TNF-α. It is available in intravenous and subcutaneous forms and is approved for both induction and maintenance therapy in CD.
●Certolizumab is another anti-TNF agent licensed in some countries for treatment.
IL-12/IL-23 inhibitors
●Ustekinumab is approved for both induction and maintenance therapy in CD.
●Risankizumab, an IgG1 antibody that binds to the P19 subunit of IL-23, is now approved for induction and maintenance in CD.
●Guselkumab, an IgG1 antibody that binds to the P19 subunit of IL-23, is now approved for induction and maintenance in CD.
Anti-integrin
●Vedolizumab, a monoclonal antibody against the α4β7 integrin, is used for treating CD.
JAK inhibitors
● Upadacitinib is the only JAK inhibitor approved for treatment in CD.
Clinical nutrition in IBD
Nutritional management in IBD aims to optimise intake, prevent malnutrition, and avoid symptom-triggering foods. While malnutrition can occur in both UC and CD, it is more common in CD due to its potential to affect any part of the GI tract. Malnutrition may result from reduced intake, increased nutrient loss, and heightened metabolic demands, particularly during active inflammation. CD patients remain at risk even in remission.
There is no universal diet to induce CD remission, but adequate calorie and protein intake (especially during active disease) is important. The Crohn’s Disease Exclusion Diet is currently the most studied approach with accumulating supportive data for its use in adult patients with CD, while there has also been positive data on the benefits of the Mediterranean diet.
Iron supplementation is advised in cases of iron deficiency anaemia – oral iron for mild, inactive cases, and parenteral for active disease. Calcium and vitamin D levels should be monitored and supplemented, especially in steroid-treated patients. Patients with significant diarrhoea or high-output stomas require fluid and electrolyte monitoring. In CD with strictures or obstructive symptoms, a low-fibre, modified-texture diet may help.
Exclusive enteral feeding: An exclusive liquid formula diet may be used for induction of remission in mild-to-moderate disease. However, strict adherence is required, and this approach is often not feasible for all patients.
Multidisciplinary approach
An integrated care approach is essential in managing IBD. This approach should involve a team of specialists, including gastroenterologists, colorectal surgeons, pathologists, radiologists, GPs, pharmacists, IBD nurses, and psychologists.
Treatment monitoring
The Harvey-Bradshaw Index (HBI) is commonly used to monitor disease activity, with a score of ≤4 indicating clinical remission. Additionally, patient-reported outcome measures (PROMs), such as the eight-item IBD-control PROM, can provide valuable information. However, neither the HBI nor PROMs correlate strongly with objective markers of inflammation, as they are influenced by subjective factors. Previously used tools like the Crohn’s Disease Activity Index are used in clinical trials, but are not suitable for disease monitoring in clinical practice.
The STRIDE II consensus emphasises the importance of monitoring and achieving symptom control, but sets out short, intermediate, and longer-term targets when treating patients with CD, including initial normalisation of inflammatory biomarkers and subsequent on mucosal healing with a view to reducing disease-related complications and disability.
CRP and FCAL are the most commonly used biomarkers for monitoring CD. Elevated CRP levels are associated with clinical disease activity and endoscopic inflammation, while normalisation typically indicates a positive treatment response. However, it is estimated that 20 per cent of CD flare-ups occur with normal CRP levels. FCAL may be normal in patients with isolated small bowel CD.
Further follow-up tests should encompass monitoring nutritional status including iron, vitamin B12, folate, and vitamin D levels every six months. Screening for anxiety and depression is also recommended, as these conditions are more prevalent in IBD patients compared to the general population.
Surveillance endoscopy should begin eight years after the diagnosis of CD in patients with colonic involvement. Surveillance intervals depend on the extent of the disease, presence of complications such as strictures, risk factors for malignancy, and coexisting diagnoses such as PSC.
Endoscopic scores, such as the Crohn’s Disease Endoscopic Index of Severity and the more easily calculated Simplified Endoscopic Activity Score for Crohn’s Disease, are used to assess disease severity and response to therapy, but are not widely used in everyday practice. The Rutgeerts Score is specifically used to assess recurrent disease in the neo-terminal ileum following surgery.
Potential adverse effects of CD therapy
Patients with CD face increased cancer risks, including small bowel adenocarcinoma, colonic cancer, and melanoma. Immunosuppressive treatments, such as thiopurines and biologics, raise the risk of non-melanoma skin cancer and lymphoma, with the highest lymphoma risk in patients aged 65+. Hepatosplenic T-cell lymphoma is a rare, but serious concern, particularly in young males on thiopurines.
There is also an elevated risk of serious infections, including pneumonia, shingles, and C difficile colitis, especially when on corticosteroids or biologics. Routine vaccinations (eg, pneumococcal, shingles) and surveillance are recommended.
Osteopaenia and osteoporosis are common, particularly with prolonged corticosteroid use; CD patients with >three months of corticosteroid exposure should undergo bone density screening.
References on request
Authors: Dr Jurie Mostert, Registrar in Gastroenterology, St Vincent’s University Hospital, Dublin; and Prof Glen Doherty, Consultant Gastroenterologist, St Vincent’s University Hospital, Dublin
To earn free CPD points, go to www.doctorCPD.ie and complete the quizzes based on this article












Leave a Reply
You must be logged in to post a comment.