






General practice nursing is a cornerstone of primary care delivery in Ireland, with general practice nurses (GPNs) playing an increasingly autonomous and collaborative role in chronic disease management, immunisation, cervical screening, health promotion, and preventative care.
The publication of the Nursing and Midwifery Board of Ireland (NMBI) Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives (2025) provides an updated professional framework that integrates scope of practice and record-keeping within a broader ethical and accountability context.
This second article in our series examining the practical application of the 2025 Code in general practice focuses on scope of practice, professional accountability, multidisciplinary collaboration, and robust clinical documentation. Scope of practice is not a restriction, but a professional framework that supports us as GPNs in delivering safe, evidence-based, person-centred care while safeguarding our professional registration.
Introduction
General practice nursing is an integral component of primary care delivery. GPNs work in a dynamic environment shaped by national policy, multidisciplinary teams, and collaborative models of service delivery. The GPN role is broad, autonomous, and continuously evolving. Sláintecare’s emphasis on reducing unnecessary hospital admissions and increasing community-based, integrated care1 has contributed to the continued development of roles in primary care, particularly the GPN role.
The Irish College of GPs estimates that GPNs conduct approximately 7.75 million consultations annually in Ireland,2 demonstrating the substantial contribution of GPNs to primary care delivery and supporting the objectives of Sláintecare.
GPNs play a key role in delivering complex, autonomous care across chronic disease management, preventative health, women’s health, immunisation, wound management, and health promotion. This expanded remit, which aligns closely with Sláintecare’s objectives, raises important questions regarding our professional boundaries, education, competence, accountability, delegation, inter-professional dynamics, and governance. In other words, our scope of practice.
“Scope of practice is the range of roles, functions, responsibilities, and activities which a registered nurse or registered midwife is educated, competent, and has authority to perform. Your scope of practice is fully linked to the Code, which are the overarching principles that guide you in your professional practice.”
– NMBI (2025)3
The 2025 Code of Professional Conduct and Ethics from NMBI embeds scope of practice directly into professional standards. Therefore, we are required, as nurses, to actively determine whether our education, competence, experience, collaborative practice, and practice context support the activities we undertake.
Our scope of practice is not determined by our job title, convenience, our employer’s expectations, or service pressure. Our overarching priority as registered nurses and midwives is safe, effective, and person-centred care, with clear personal accountability for our professional actions at all times. We must also protect our NMBI registration as it is our passport to work, and we worked hard to gain it.
Enacting scope in general practice
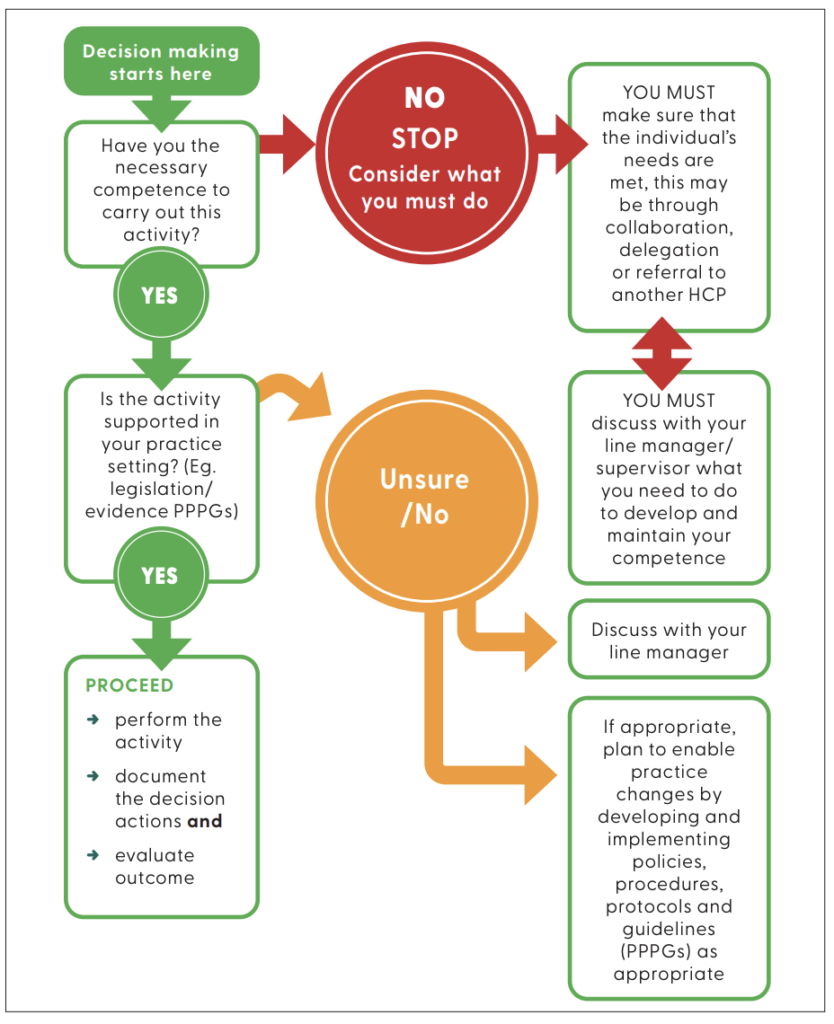
NMBI present several factors that they deem to influence our individual scope of practice:3
✽ Education preparation, professional practice, and competence
Your initial education sets the foundation for your scope of practice. Additional education and practice experience further develop your knowledge and skills that may broaden the range of activities you are competent to undertake.
✽ Guidelines, policies, and evidence-based research
Local, national, and international practice policies, procedures, protocols and guidelines, and evidence-based research inform and guide your practice. Adhering to these helps align with legal and ethical requirements and reflects current best practices in healthcare.
✽ Practice setting
Your workplace environment – whether in the acute, community, or other practice settings – affects your scope of practice. Each setting may require distinct skills, knowledge, and influence the specific competencies required.
✽ Collaborative practice
This involves shared responsibilities, interprofessional learning, and a holistic approach to care. It involves practitioners working with other professionals to provide comprehensive, person-centred care.
These factors underpin the scope of practice framework, which serves as our guide for delivering safe, high quality, patient-centred care. It supports clinical decision-making, helps identify continuing professional development (CPD) needs, clarifies professional roles, and promotes reflective practice to enhance learning and maintain safe, effective care.
Our scope of practice is not passive. It demands reflective professional judgement, supported by recognised education, demonstrable competence, appropriate governance, ongoing continuing professional development, clinical audit, and accurate documentation. In general practice, where, as nurses, we often work autonomously, this framework safeguards patients, strengthens our practice, and advances the GPN discipline.
We must be accountable for our professional decisions and actions in delivering patient care. Accountability extends beyond completing tasks; it includes clinical, rational, and ethical decision-making.
As a GPN, interpreting HbA1c results, for example, we must not only understand the numerical value, but also consider the result in the context of the patient’s overall health profile. Failure to recognise deteriorating glycaemic control could result in delayed intervention and adverse outcomes. Thus, accountability in this context is fundamentally linked to clinical competence and reflective practice.
Recognising and practising within our professional scope requires us to continually reflect on our daily roles as GPNs and on the care we are asked to provide. This must be evidence-based care. Our clinical practice should be guided by authoritative national and international guidelines, such as those issued by the National Immunisation Advisory Committee (NIAC) and the Professional Development Coordinator (PDC) written guidelines to support the National Immunisation Office (NIO) programmes.
Others include the Global Initiative for Asthma,6 the European Society of Cardiology,7 and the relevant contractual frameworks, including GP Chronic Disease Management (CDM) and CervicalCheck programmes.8 We must never rely on a ‘see one, do one’ approach to care delivery. No nurse should undertake any task or provide care for which they have not received the appropriate education or training, or demonstrated competence.
Core practice areas
CDM
In general practice, CDM is a central and well-established component of the GPN role. CDM significantly expands patients’ access to care and directly supports Sláintecare’s shift toward care closer to home. GPNs frequently lead structured care for patients with long-term conditions, involving regular reviews, monitoring, and education, supporting GPs in delivering evidence-based preventive care. This GPN-led CDM activity enhances service efficiency and patient outcomes while reducing demand on GP appointments.
Structured reviews for patients with long-term conditions include:
✽ Adults with type 2 diabetes
✽ Hypertension
✽ Chronic obstructive pulmonary disease (COPD)/ asthma
✽ Cardiovascular disease
✽ Chronic kidney disease
✽ Obesity management.
Within the NMBI 2025 framework, this area reflects autonomous yet collaborative nursing practice. Examples of activities within scope of practice include:
✽ Blood pressure review
✽ HbA1c and blood glucose monitoring
✽ Spirometry (if trained by IARS or similar and competent)
✽ Diabetic foot assessments
✽ Medication reviews
✽ Immunisation
✽ Lifestyle counselling
✽ Risk factor screening
✽ Call, recall, and follow-up systems.
Crucially, the CDM role sits within the GPN’s scope of practice when the necessary training, competence in clinical assessment, interpretation of findings, and escalation pathways are in place. From a scope of practice perspective, as GPNs, we must be capable not only of performing technical tasks such as those listed above, but also of applying clinical judgement and awareness of the boundaries of independent decision-making. This applies, for example, in abnormal findings, deterioration or deviation from expected treatment outcomes that require GP review or onward referral, resulting in collaborative engagement with the GP or specialist colleagues.
For example, identifying:
✽ Worsening glycaemic control
✽ Uncontrolled hypertension
✽ Acute exacerbation of COPD
✽ Non-adherence risks
✽ Red flag symptoms requiring GP or specialist review.
This approach to care aligns strongly with NMBI’s emphasis on safe, person-centred, evidence-based care and accountability for decision-making.
IMMUNISATION AND VACCINE DELIVERY
Immunisation is a core area of GPN practice and must be grounded in formal, evidence-based guidance from NIAC and the NIO.4,5 Using non-authoritative sources could place you as a GPN outside safe professional practice and potentially outside defensible scope if an adverse event occurred.
From a scope of practice perspective, social media is not an acceptable source for clinical decision-making and could result in errors in practice or data protection risks. Maintaining competence in immunisation technique, vaccine ordering, receipt, storage and handling, emergency preparedness, and updated schedules through formal CPD is mandatory.
Immunisation is only within the NMBI scope of practice framework when supported by:
✽ Education/formal training
✽ Current competence
✽ Local policy for administering, documenting, ordering, and storage
✽ Emergency preparedness.
This is particularly important in a general practice setting, where the nurse may independently run vaccine clinics, such as:
✽ National Childhood Immunisations Programme
✽ Seasonal Immunisation Programme: Influenza, pneumococcal
✽ Covid-19 boosters
✽ Travel vaccines.
The NMBI 2025 competence requirements place strong emphasis on maintaining up-to-date knowledge and safe decision-making.3
This means that as GPNs we must work in accordance with:
✽ NIAC guidance
✽ NIO schedules and guidance
✽ GP practice policy and protocols (your PDCGPN will assist with policies, procedures, protocols, and guidelines)
✽ Anaphylaxis and emergency response procedures.
Key scope requirements in immunisation include competence in:
✽ Cold chain management
✽ Consent processes
✽ Contraindications screening
✽ Documentation
✽ Batch number recording
✽ Adverse event management
✽ Anaphylaxis response
✽ Advising vaccine-hesitant parents and adults.
These competencies align with NMBI’s 2025 standards on professional competence, accountability, and record integrity.
Cervical screening
Cervical screening via the national CervicalCheck Programme is a good example of expanded scope of practice for GPNs. The programme has transitioned to human papillomavirus (HPV)-based primary testing in 2020, and clinical practice must be under the governance framework of the general practice CervicalCheck contract and the national screening programme requirements.
Cervical screening is not part of pre-registration or undergraduate training and must not be allocated or undertaken as a routine task or in the absence of training. The NMBI scope of practice framework would classify this as requiring role expansion through additional education and competence achievement.
As a GPN undertaking CervicalCheck sampling you must be able to demonstrate:
✽ Formal accredited training
✽ Programme-specific competence
✽ Supervised practice
✽ Ongoing audit participation
✽ Familiarity with CervicalCheck standards
✽ Understanding of HPV primary screening pathways.
The transition to HPV primary testing means competence must include:
✽ Understanding the rationale for HPV-based screening
✽ Age-based eligibility
✽ Recall intervals
✽ Result interpretation pathways
✽ Referral processes.
Failure to maintain CPD or programme audit involvement as GPNs could place this practice outside of defensible scope of practice.
Multidisciplinary collaboration: How the GPN adds value
GPNs contribute value across the multidisciplinary team, supporting the GP workload, improving access to care, enhancing chronic disease outcomes, and delivering national programmes. These contributions are central to achieving national health goals and realising Sláintecare’s vision.
Collaborative practice is highly relevant in general practice, and the GPN role is fundamentally collaborative, working closely with:
✽ GPs
✽ Practice managers
✽ Community/public health nurses
✽ Physiotherapists
✽ Dietitians
✽ Occupational therapists
✽ Pharmacists
✽ CDM hub and hospital specialists.
NMBI scope of practice principles support shared but clearly defined professional responsibilities, and the GPN must understand:3
✽ What is within the autonomous nursing scope
✽ What requires GP review
✽ When referral is necessary
✽ How to escalate concerns safely.
This includes safe boundaries around advice-giving, triage, and independent decision-making.
The added value of the GPN is often seen in:
✽ Reduced GP workload
✽ Improved and timely patient access
✽ Continuity of care
✽ Proactive prevention
✽ Patient education and health promotion
✽ Referral to support and self-management services such as the Living Well Programme.
Thus, directly supporting Sláintecare’s integrated community care model.
Nurse prescribing and advanced practice
Nurse medicinal product and radiological prescribing are clear examples of extended scope of practice. The number of GPNs who are registered nurse prescribers is increasing. This prescriptive authority requires recognised education, current competence, clear governance structures, prescribing-related CPD, clinical audit participation, and accurate record-keeping. Prescribing activity is auditable and may be subject to regulatory review, which underscores the need for meticulous documentation.
NMBI explicitly identifies prescribing as an expansion of scope beyond initial registration competence. For a GPN, nurse prescribing can significantly enhance autonomous practice in many areas:
✽ Chronic disease medications
✽ Wound care products
✽ Vaccinations
✽ Antibiotics within protocol
✽ Contraceptive prescribing.
However, this is prescribing practice is only within scope when the GPN:
✽ Has completed recognised education
✽ Is registered with NMBI on the RNP division
✽ Practises under agreed collaborative local governance
✽ Maintains competence
✽ Participates in audit.
The NMBI 2025 Code strongly emphasises clinical accountability and auditability and every prescribing decision must be supported by clear documentation of:3
✽ Assessment findings
✽ Rationale for prescribing
✽ Medication choice
✽ Dose
✽ Safety checks
✽ Patient education
✽ Follow-up plan.
This is particularly important in general practice, where prescribing decisions may be reviewed medico-legally. Meticulous documentation is, therefore, not optional – it is a core scope of practice requirement.
Professional development and discipline growth
Professional development enhances the GPN’s individual competence and strengthens the GPN discipline. Our scope of practice is dynamic, not static. Scope of practice evolves as competence evolves. This is especially important under the NMBI 2025 (p27) professional competence framework.
NMBI places clear responsibility on the nurse to identify competence gaps and address them through CPD. This means professional growth is not optional; it is part of maintaining safe practice. This is especially relevant in general practice, where the GPN role continues to expand in response to service demands and national policy developments. Role development not only enhances individual competence, but also contributes to the growth and recognition of the GPN discipline.
Many activities demonstrate expanded scope, and these help to build and strengthen professional leadership and advanced professional development. Examples include:
✽ Specialist diplomas/higher education
✽ Conference presentation
✽ Teaching students
✽ Quality improvement audits
✽ Publication
✽ Policy development
✽ Leadership roles.
Registration
GPNs should ensure their NMBI registration states general practice as the workplace to enable an accurate count of GPNs, supporting workforce intelligence and national planning. Support from GPs is critical for the professional development of GPNs, as effective teamwork enhances governance, clinical outcomes, and working within our scope of practice.
The NMBI 2025 framework makes clear that competence is continually evolving and must be supported through structured CPD.3 Securing time away from clinical practice for CPD and clinical updates can be difficult – however, these are necessary, and such time must be negotiated when required.
The PDCGPNs, appointed by the HSE, provide monthly webinars, expanded practice guidance, CPD planning support, and representation at educational and policy fora. Proactive engagement strengthens individual practice and multidisciplinary team development. We are here to support you. Please never hesitate to contact us.
Record-keeping and professional accountability
Accurate, contemporaneous record keeping is not simply an administrative task – it is an essential element of our scope3 and our professional practice. The updated NMBI Code significantly strengthens professional expectations around record keeping by embedding it within the broader ethical and legal framework of nursing and midwifery practice.
The 2025 Code replaces the former standalone Recording Clinical Practice (2015) guidance and integrates record-keeping standards directly into the Code itself. This integration highlights the importance of documentation as a core professional, ethical, and patient-safety obligation.
Documentation is evidence of our clinical care and consultations, capturing collaborative decision-making, informed consent, continuity of care, and audit readiness. There is no substitute for clear, accurate, and timely recording of care.
The Code places strong emphasis on records as legal documents that may be used in complaints, investigations, or fitness-to-practise proceedings. This is a particularly significant aspect because it reinforces that documentation is evidence of the care we deliver and of the GPNs clinical reasoning. We know the message: ‘If it’s not recorded, it can be presumed not to have happened.’ If care or consultations are not documented, it may be very difficult to defend professionally.
Documentation must be written to a high standard. The Code expects records to be:
✽ Accurate
✽ Clear and contemporaneous
✽ Objective and factual
✽ Timely
✽ Confidential and secure.
These standards reflect best practice documentation principles, aligning with legal standards around professional negligence and data governance. The Code discourages vague, judgmental, or emotive language and instead prioritises evidence-based entries that clearly distinguish observation from interpretation.
A notable development in the 2025 Code is its recognition of care delivered virtually and through digital platforms. This modernisation is especially relevant given the expansion of electronic health records, telehealth, and digital communication. General practice has been ahead of this trend for decades now. GPNs therefore have the advantage of robustly designed IT and record management systems that can enable timely, accurate, and clear recording of clinical practice.
Consultation templates should be considered for use to support best practice in recording clinical practice, especially in a pressured environment. GPN consultations are finite, and many of you report a requirement to reduce appointment times to meet the ever-growing demand.
Good practice in clinical record-keeping is the responsibility of every member of your team. Yes, general practice is busy and time pressures exist – however always make, and take, the time to ensure accurate and comprehensive recording of your clinical care.
Conclusion
As general practice nursing continues to grow in response to the strategic direction of Irish healthcare, clarity around scope of practice has never been more important. The growing autonomy and complexity of the GPN role bring significant opportunities for leadership, innovation, and enhanced patient outcomes, but also demand a dedicated commitment to professional accountability, competence, and evidence-based care.
Understanding and actively applying our scope of practice as GPNs is fundamental to safeguarding patients, protecting professional standards, and strengthening confidence in the role within primary care. It is through reflective practice, ongoing education, robust governance, and collaborative working that we can continue to develop the discipline and fully realise the ambitions of Sláintecare.
Scope of Practice is not a restriction; it is a professional foundation and a professional framework that enables safe, autonomous, and progressive nursing care, while also safeguarding our own NMBI registration. When applied with reflective judgement, evidence, education, governance, and collaboration, it enables us as GPNs to deliver safe, effective care and contribute strategically to the evolution of primary care in Ireland. As the GPN role continues to evolve, it will remain central to the delivery of high-quality, person-centred care in communities across Ireland.
Contact Details for PDCs
Marie Courtney
marie.courtney@hse.ie
086 787 2408
Integrated Health Areas of Cork and Kerry
Marie Cantwell
marie.cantwell@hse.ie
087 607 8925
Integrated Health Areas of Dublin North County and Dublin North City and West
Kathy Taaffe
kathy.taaffe@hse.ie
087 132 1424
Integrated Health Areas of HSE West and Northwest
Elizabeth Carroll
elizabeth.carroll2@hse.ie
087 491 2159Integrated Health Areas of Carlow, Kilkenny, South Tipperary, and Wexford/ Waterford
Mairead Murphy
mairead.murphy11@hse.ie
087 120 6184Integrated Health Areas of HSE West and Northwest








Leave a Reply
You must be logged in to post a comment.