







Reference: March-April 2025 | Issue 2 | Vol 18 | Page 11
Start this Module
Module Title
The presentation, diagnosis, and treatment of opioid dependenceModule Author
Dr Garrett McGovernCPD points
2Module Type
TutorialThis module gives an expert overview of the presentation, diagnosis, and treatment of opioid dependence, with the latest Ireland-specific treatment guidelines and protocols
Opioid use disorder (OUD) defines the chronic use of opioid drugs (commonly heroin or opioid analgesic drugs) leading to clinically significant stress or impairment. People with OUD are at an increased risk of morbidity, mortality, and other adverse health and social conditions.1 The condition affects over 16 million people worldwide with over 120,000 deaths annually attributed to opioids,2 and many other negative societal outcomes.3,4
OUD results in a strong compulsion to take opioids, an increase in opioid tolerance over time, and withdrawal symptoms when opioids are discontinued. In Ireland, the main opioid necessitating treatment from addiction services is heroin, but in the past 10-15 years there has been an increase in opioid analgesic dependence and the numbers seeking treatment.
Whilst exact prevalence data remains elusive, it is estimated that from 2006 to 2016 codeine use in Ireland increased 208 per cent.5 Because analgesic preparations containing codeine can be sold over-the-counter (OTC) the public perception often underestimates the potential harms of using these drugs regularly. The mainstay of treatment for OUD is opioid substitution treatment (OST). As of 2021, there were 12,657 people in receipt of OST in Ireland.6
| DSM-5 CRITERIA FOR DIAGNOSIS OF OPIOID USE DISORDER | |
|---|---|
| 1 | Opioids are often taken in larger amounts or over a longer period of time than intended |
| 2 | There is a persistent desire or unsuccessful efforts to cut down or control opioid use |
| 3 | A great deal of time is spent in activities necessary to obtain the opioid, use the opioid, or recover from its effects |
| 4 | Craving, or a strong desire to use opioids |
| 5 | Recurrent opioid use resulting in failure to fulfill major role obligations at work, school, or home |
| 6 | Continued opioid use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of opioids |
| 7 | Important social, occupational, or recreational activities are given up or reduced because of opioid use |
| 8 | Recurrent opioid use in situations in which it is physically hazardous |
| 9 | Continued use despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by opioids |
| 10 | *Tolerance, as defined by either of the following: (a) A need for markedly increased amounts of opioids to achieve intoxication or desired effect (b) Markedly diminished effect with continued use of the same amount of an opioid |
| 11 | *Withdrawal, as manifested by either of the following: (a) The characteristic opioid withdrawal syndrome (b) The same (or a closely related) substance is taken to relieve or avoid withdrawal symptoms |
| Severity: Mild: 2-3 symptoms Moderate: 4-5 symptoms Severe: 6 or more symptoms | |
FIGURE 1: DSM-5 criteria for OUD. Source: www.emergencymedicinecases.com
Identifying OUD
Identifying patients who may potentially suffer from OUD is difficult because of the stigma associated with the condition. For this reason many sufferers find it difficult to present to their healthcare provider (HCP) and discuss options for treatment. It is important to adopt an empathic, non-judgemental approach to any patient who may present for treatment of an issue relating to addiction.
Given heroin is particularly demonised by society, it can often be difficult for patients to open up and talk about the issue. It is also important that any HCP encountering patients with potential OUD is in a position to either treat the problem or make an onward referral.
For HCPs, it is important that they are in a position to identify patients who present with potential opioid problems, particularly where the main reason for the consultation is seemingly unrelated to a potential addiction issue. As outlined, the two main opioids likely to result in problematic use are heroin and opioid analgesics (often codeine). Whilst there are commonalities to the pattern of use and sequelae of both types of opioid problem, the presentation and course of each addiction is often quite distinct.
Heroin addiction
The most common routes by which heroin is taken include injecting, snorting, and smoking (‘chasing’ or ‘chasing the dragon’). The physical consequences of injecting tend to be more severe than smoking or snorting, although the extent and impact of the addiction can be devastating regardless of route of use. Injecting exposes users to a higher risk of fatal overdose, soft tissue infections, deep vein thrombosis (DVT), and viral hepatitis and human immunodeficiency virus (HIV) transmission.
There may be evidence of track marks on arms, but unless the patient specifically reports a history of heroin use and their arms are not visible then it is difficult to pick this sign up. Respiratory complications of smoking heroin include tuberculosis and pneumonia and worsening pre-existing conditions such as asthma and chronic obstructive pulmonary disease.
Heroin addiction, like other chronic addictions, can result in debt, loss of employment and relationships, theft, and contact with the criminal justice system. When an addiction becomes overwhelming, sufferers become prone to various forms of exploitation to pay back drug debts (eg, prostitution, drug dealing, or drug ‘muling’).
Codeine analgesic addiction
Codeine analgesic formulations (mainly codeine-ibuprofen and codeine-paracetamol) are commonly sold OTC in Ireland. In response to growing concerns about the rising use of these medications and problems associated with long-term use, tighter restrictions have been implemented in the past decade.
The medication was once sold ‘front-of-shop’ and consumers could purchase the drug with little scrutiny. A change in the law moved the medication behind the counter so that people buying them had to request them from the pharmacist, while being asked a number of questions relating to safe and short-term use.
Long-term, excessive use of these medications exposes the user to some very serious complications such as stomach ulceration, perforation and bleeding, and renal damage (non-steroidal anti-inflammatory drugs), as well as liver damage (paracetamol).
Pathognomonic of this addiction is the need to travel to different pharmacies in order to secure the medication and stave off withdrawal symptoms. These medications are also not cheap. A severe addiction can cost a lot of money to maintain and push people into debt.
Screening and assessment
There are many different screening tools that can help identify potential opioid problems. One of the most well established, simple, and easy to administer tools is the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), criteria for opioid dependence. This is an 11-item questionnaire examining various symptoms and patterns related to opioid use. The presence of two symptoms or more denotes the presence of OUD (see Figure 1) with greater number of symptoms being associated with increasing severity.
A thorough assessment is essential when patients are being commenced on OST. There are a number of internationally validated assessment tools. The National Addiction Centre, King’s College London, has developed a patient assessment guide which consists of 18 headings, covering various important aspects of the history including demographic information, current opioid/other drug/alcohol use, medical/psychiatric history, personal/social/family history, mini mental state examination, differential diagnosis, aetiology, and concluding with a formulation where a plan is made for management and treatment.
A urine test is helpful to establish the presence (or absence) of opioids such as methadone or heroin (morphine). Patients will often access methadone sold illicitly in the period before they commence treatment.
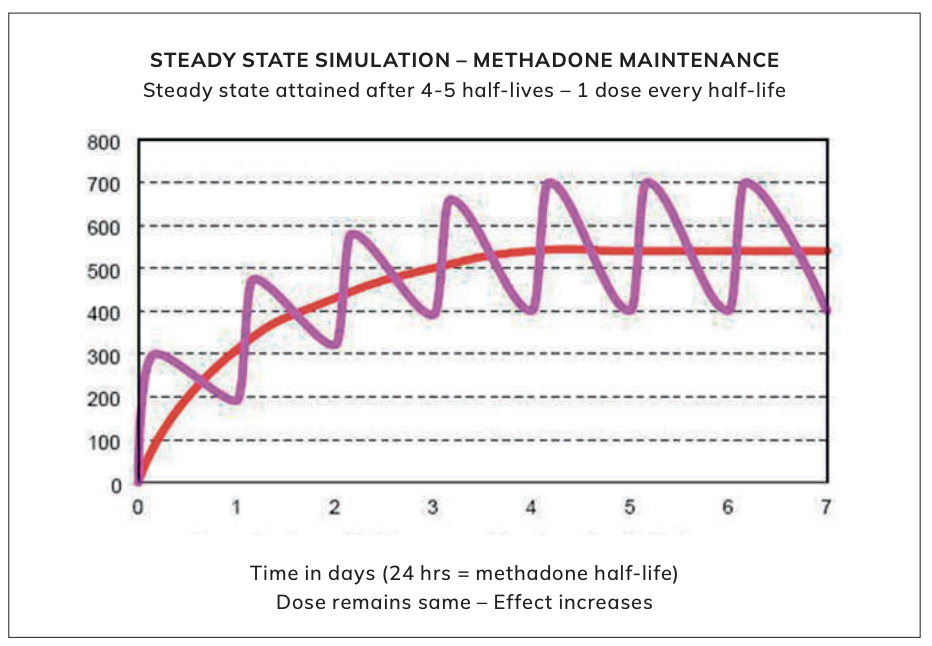
FIGURE 2: Steady state simulation. Source: Methadone-steady-state, Janaburson’s Blog (wordpress.com)
Induction of OST
When a diagnosis of OUD is made and an agreement arrived at to start OST, it is imperative that the induction is carried out safely. Methadone and buprenorphine induction are quite different processes, each medication presenting unique risks to the patient.
Methadone
Methadone is a full mµ opioid agonist with a half-life of 15-60 hours (mean 22 hours). It works by occupying opioid receptors and reduces withdrawal symptoms and craving. The optimum dose range is 60-120mg daily for most patients. A small subset will stabilise on doses smaller than 60mg and some will need greater than 120mg.
It is an oral solution usually containing a methadone concentration of 1mg/ml (although more concentrated versions are used in exceptional circumstances). The usual starting dose is 20-30mg with no more than a gradual 20-30mg dose increase in the first week of treatment. It takes about four to five half-lives to attain steady state serum methadone levels, so that the elimination of the drug is in balance with the amount of drug left in the body.7
In some cases, however, it can take much longer, making the person more susceptible to overdose if the methadone dose is inappropriately increased in that first week of treatment.8,9
Once steady state is reached the person becomes opioid tolerant and this is protective against overdose, rendering heroin relatively ineffective if taken ‘on-top’ of methadone. Methadone treatment is often seen as the gold standard and has decades of research demonstrating its effectiveness in reducing overdose mortality.10,11 It also reduces injecting and the transmission of bloodborne viruses such as hepatitis C and HIV.12
| FOR BUPRENORPHINE/NALOXONE INDUCTION: | |||
|---|---|---|---|
| Enter scores at time zero, 1-2 hours after first dose, and at additional times that buprenorphine/naloxone is given over the induction period | |||
| DATE/TIME | DATE/TIME | ||
|
Resting pulse rate: (record beats per minute) Measured after patient is sitting/lying for one minute 0 pulse rate 80 or below 1 pulse rate 81-100 2 pulse rate 101-120 4 pulse rate greater than 120 |
Runny nose or tearing: Not accounted for by cold symptoms or allergies 0 not present 1 nasal stuffiness or unusually moist eyes 2 nose running or tearing 4 nose constantly running or tears streaming down cheeks |
||
|
Sweating: Over past ½ hour not accounted for by room temperature or patient activity 0 no report of chills or flushing 1 subjective report of chills or flushing 2 flushed or observable moistness on face 3 beads of sweat on brow or face 4 sweat streaming off face |
GI upset: Over last ½ hour 0 no GI symptoms 1 stomach cramps 2 nausea or loose stool 3 vomiting or diarrhea 5 multiple episodes of diarrhea or vomiting |
||
|
Restlessness: Observation during assessment 0 able to sit still 1 reports difficulty sitting still, but is able to do so 3 frequent shifting or extraneous movements of legs/arms 5 unable to sit still for more than a few seconds |
Tremor: Observation of outstretched hands 0 no tremor 1 tremor can be felt, but not observed 2 slight tremor observable 4 gross tremor or muscle twitching |
||
|
Pupil size: 0 pupils pinned or normal size for room light 1 pupils possibly larger than normal for room light 2 pupils moderately dilated 5 pupils so dilated that only the rim of the iris is visible |
Yawning: Observation during assessment 0 no yawning 1 yawning once or twice during assessment 2 yawning three or more times during assessment 4 yawning several times/minute |
||
|
Bone or joint aches: If patient was having pain previously, only the additional component attributed to opiate withdrawal is scored 0 not present 1 mild diffuse discomfort 2 patient reports severe diffuse aching of joints/muscles 4 patient is rubbing joints or muscles and is unable to sit still because of discomfort |
Anxiety or irritability: 0 none 1 patient reports increasing irritability or anxiousness 2 patient obviously irritable or anxious 4 patient so irritable or anxious that participation in the assessment is difficult |
||
|
Gooseflesh skin: 0 skin is smooth 3 piloerection of skin can be felt or hairs standing up on arms 5 prominent piloerection |
|||
| Total Score: | |||
| Observer’s initials: | |||
| Blood pressure/pulse: | |||
| Dose of buprenorphine/naloxone given: | |||
| Note: Give first dose when COWS score > 7 | |||
| Score: 5-12 = Mild; 13-24 = Moderate; 25-36 = Moderately Severe; More than 36 = Severe Withdrawal | |||
FIGURE 3: Clinical Opiate Withdrawal Scale. Source: Clinical Opiate Withdrawal Scale: Juno EMR Support Portal
Buprenorphine
Buprenorphine is a semi-synthetic opioid derived from thebaine, a naturally occurring alkaloid of the opium poppy, Papaver Somniferum. It is a partial mµ opioid agonist. It is also a weak kappa receptor antagonist. It reaches a ‘ceiling’ effect at higher doses where escalating doses do not lead to a greater opioid effect. This is important because it results in less adverse effects (eg, respiratory depression) than full mµ agonists (eg, methadone).
Buprenorphine has high affinity for, but low intrinsic activity at, mµ opioid receptors and the high affinity is dose related. Buprenorphine displaces other full mµ opioid agonists from opioid receptors such as morphine and methadone, causing precipitated withdrawal if there is not a washout period of the current opioid prior to switching to buprenorphine.
Methadone to buprenorphine is a particularly tricky conversion as methadone takes a considerable length of time to clear from the system. It is advised that the dose of methadone should be reduced down to as low a dose as possible and no higher than 30mg, with this last dose been taken at least 24-48 hours before the first dose of buprenorphine. If the patient has been taking heroin, they should be advised to use it for the last time six to 12 hours before starting buprenorphine.
In practice, the use of the Clinical Opioid Withdrawal Scale (COWS) is a useful aid to check for objective signs of withdrawal, which should be present before commencing buprenorphine (Figure 3). In recent years microdosing with buprenorphine has allowed an uncomplicated conversion to take place on higher doses of methadone. This practice, however, has not reached Ireland yet.
In Ireland there are two buprenorphine/naloxone formulations licensed for use. Since 2007, suboxone has been used, and recently zubsolv has been made available. There are slight differences in the way the doses are delivered between the two formulations. Equivalent doses are shown in Figure 4.
Naloxone is added to buprenorphine to reduce the risk of misuse. When these products are taken as prescribed, sublingually, buprenorphine’s opioid effects do not allow naloxone to exert its opioid withdrawal effects. However, if the sublingual tablets are crushed and injected, naloxone dominates and can cause opioid withdrawal symptoms.13
Once satisfied the COWS score is at least seven, and there are some objective signs of opioid withdrawal present, then the first dose of buprenorphine can be given. Usually the first dose will be 4-8mg on the first day and this can be increased to 12-16mg on day two. Most patients will require doses in the 12-24mg range. Some may need more and some will require less.
Precipitated withdrawal
Precipitated opioid withdrawal results in the rapid onset of opioid withdrawal symptoms (which include aches and pains, nausea and vomiting, diarrhoea and abdominal cramps, dilated pupils, increased lacrimation, rhinorrhoea, yawning, piloerection, goosebumps on skin, etc) within an hour or two of taking the first dose of buprenorphine. The symptoms gradually subside over the next six to 24 hours. This occurs in about 9 per cent of cases of buprenorphine induction.14
Whilst good assessment and use of the COWS will reduce the risk of precipitated withdrawal, there can be cases where, despite a moderately high COWS score, withdrawal symptoms occur in the hours after taking the fist dose of buprenorphine.
An interesting case study in the Drug and Alcohol Review in 2021 discussed a buprenorphine induction where the patient presented in moderate opioid withdrawal (COWS score 16) and developed precipitated withdrawal. The culprit in this case was thought to have been a single dose of methadone taken a few days previously. The patient did not mention this in the history and said they had only been taking heroin. The precipitated withdrawal symptoms were successfully managed as an inpatient by monitoring symptoms and increasing the buprenorphine dose.15
Loss of tolerance
Tolerance describes the diminished response to a drug over the course of repeated or prolonged exposure. This mechanism allows physiological processes to achieve stability in a constantly changing environment. In the management of patients with OUD, the importance of opioid tolerance cannot be overstated.
| SUBOXONE sublingual tablets, including generic equivalents | Corresponding dosage strength of ZUBSOLV sublingual tablets |
|---|---|
| One 2mg/0.5mg buprenorphine/naloxone sublingual tablet | One 1.4mg/0.36mg zubsolv sublingual tablet |
| One 8mg/2mg buprenorphine/naloxone sublingual tablet | One 5.7mg/1.4mg zubsolv sublingual tablet |
|
12mg/3mg buprenorphine/naloxone taken as: ► One 8mg/2mg sublingual buprenorphine/naloxone tablet AND ► Two 2mg/0.5mg sublingual buprenorphine/naloxone tablets |
One 8.6mg/2.1mg zubsolv sublingual tablet |
|
16mg/4mg buprenorphine/naloxone taken as: ► Two 8mg/2mg sublingual buprenorphine/naloxone tablets |
One 11.4mg/2.9mg zubsolv sublingual tablet |
FIGURE 4: OST dosing guide. Source: buprenorphine Quick Start Guide (samhsa.gov)
► Up to two days missed – no change in dose
► Three days missed – dose reduced by 10mg and increased to normal dose the following day
► Four days missed – dose reduced by 20mg and increased by 10mg a day up to normal dose over the following days
► Five days missed – dose reduced by 30mg and increased by 10mg a day up to normal dose over the following days
► Six days or more missed – no dose given. Patient advised to attend the next available clinic for review by doctor
FIGURE 5: Methadone dosing algorithm
Opioid tolerance differs for different opioids. For example, one of the great benefits of methadone is that within a couple of weeks of commencing treatment it will confer good opioid tolerance, which in turn will make heroin use less effective and reduce the risk of overdose.
There are a number of well-established times in the treatment journey of patients where they are at a significantly heightened risk of fatal overdose due to reduced opioid tolerance. The first occurs at the commencement of methadone treatment and in that period (7-10 days) until steady state is reached and tolerance is uncertain.16,17
The second is when a patient leaves treatment (or any facility where they have been prescribed OST, eg, hospital or prison) and they have discontinued opioids. With reduced or lost tolerance they may not appreciate that they will be more sensitive to the respiratory depressant effects of heroin should they lapse. Injecting drug users are at a particularly high risk of fatal overdose in these circumstances.
The third circumstance where tolerance can fall is where patients on OST miss doses (usually due to non-attendance). The greater the number of days of OST missed, the greater the tolerance falls. This creates a problem when a pharmacist or doctor is faced with what re-starting dose to give. This tends to be more of an issue with methadone than buprenorphine as it has a greater propensity to cause respiratory depression.
Figure 5 is an algorithm that I formulated following discussion with many overseas addiction medicine colleagues and on the available experiences from a trawl of the literature. The key here is cautious re-induction of methadone doses and each case must be examined on its merits. A good knowledge of the patient’s history and clinical care is essential.
Measuring progress
As outlined earlier, OST has a well-established evidence-base in terms of improving the health of patients with OUD on a number of levels. As a patient progresses through treatment their progress should be assessed in a holistic way and with a view to making treatment accessible and not impeding their opportunity to progress in their life and seek educational and employment opportunities.
OST often gets criticised because patients seem to stay on the medication long-term (even though many patients with other chronic diseases remain on medication for many years, sometimes for life). Patients who wish to reduce their OST dose with a view to coming off their medication should be supported in doing so, but the risk of relapse following detoxification is high (72-88 per cent) and the overdose risk when tolerance is lost is significant. Patients need to be made aware of the risks and re-entry to OST should be seamless should they not succeed.18,19
Urine testing has a role in assessing progress, but it is over relied upon by many prescribers. A fact borne out by a review of HSE addiction services in 2010. The report was particularly critical of using the results of urine tests to assess take-home OST dose suitability.20 In any case, with the proliferation of newer psychoactive substances and other prescription drugs in the past 10 years, many of these substances will not be captured by a five panel drug screen, limiting the utility of urine testing even further.
Developing a good rapport with your patient, with honest, open dialogue makes it easier for patients to provide reliable information about their drug use. Key areas of assessment include regular attendance and good presentation and not being intoxicated or impaired. When patients are eligible for take-home OST doses, safe storage advice is essential, particularly where there are others in the home who are opioid-naïve (especially young children). Small amounts of methadone, taken unwittingly, can have fatal consequences.
Psychosocial support
Patients with OUD often suffer with comorbid psychiatric conditions. It is estimated that 65 per cent of patients have at least one mental health disorder. The risk is almost seven times higher than in the general population.21 There is also a high incidence of anxiety and affective disorders,22 sexual and physical abuse,23 as well as post-traumatic stress disorders.24 For this reason, it is particularly important to offer good wraparound psychosocial support with a multidisciplinary team approach from specialists in counselling, cognitive behavioural therapy, outreach, nursing, pharmacy, social care, psychology, and psychiatry.
Stigma
Heroin addiction is misunderstood by society. It is often viewed as a moral rather than a health issue. The treatment of heroin addiction (OST) is often as stigmastised and misunderstood as the addiction itself. OST is often depicted in a negative and a stereotypical way.
Pejorative descriptions such as ‘liquid handcuffs’, ‘substituting one addiction for another’ heap further stigma and shame on people who are trying to overcome addiction and usually a multitude of other issues.Labels such as ‘clean’ ‘dirty’ ‘junkie’ and ‘addict’ are degrading. We should view heroin addiction like any other chronic condition.
It is important to establish a good therapeutic alliance as you would when you approach patients suffering from any other condition. OUD should be no different. Punitive practices such as reducing OST doses or excluding patients from treatment for positive urine toxicology have no place in treatment.
Conclusion
Opioid use disorder is a chronic, relapsing, remitting condition which can be effectively treated with pharmacotherapy. The condition should be viewed like any other illness and not as a moral issue. Heroin addiction and the people suffering from it are often demonised by society and this prevents people from seeking treatment.
References
- Hser Y, Evans E, Grella C, Ling W, Anglin D. Long-term course of opioid addiction. Harv Rev Psychiatry. 2015;23(2):78-89.
- Chang HY, Kharrazi H, Bodycombe D, Weiner JP, Alexander GC. Healthcare costs and utilisation associated with high-risk prescription opioid use: A retrospective cohort study. BMC Med. 2018;16(1):69.
- Boutwell AE, Nijhawan A, Zaller N, Rich JD. Arrested on heroin: A national opportunity. J Opioid Manag. 2007;3(6):328-32.
- Teesson M, Marel C, Darke S, et al. Long-term mortality, remission, criminality, and psychiatric comorbidity of heroin dependence: 11-year findings from the Australian Treatment Outcome Study. Addiction. 2015;110(6):986-93.
- Cusack D. Assessing medical fitness to drive: Prescription medicines, alcohol, and illicit drugs – Practical update and assessment and prescribing guidelines for medical practitioners. Presentation at 2018 Irish College of General Practitioners Annual Conference, Dublin.
- HSE National Drug Treatment Centre. Central treatment list. Available at: www.dtcb.ie/home/default.asp.
- Benet LZ, Kroetz DL, Sheiner LB. Pharmokinetics. In: Hardman JG, Limbird LE, (Eds). The Pharmacological Basis of Therapeutics. (9th ed) New York: McGraw-Hill; 1996.
- Eap CB, Buclin T, Baumann P. Interindividual variability of the clinical pharmacokinetics of methadone: Implications for the treatment of opioid dependence. Clin Pharmacokin. 2002;41(14):1153-1193.
- Payte JT, Khuri ET. Principles of methadone dose determination. In: Parrino MW. State Methadone Treatment Guidelines. Treatment Improvement Protocol (TIP) Series 1. Rockville, MD: U.S. Department of Health and Human Services; Centre for Substance Abuse Treatment; 1993:47-58 DHHS Pub# (SMA) 93-1991.
- Bell J, Zador D. A risk-benefit analysis of methadone maintenance treatment. Drug Saf. 2000;22(3)179-190.
- Humeniuk R, Ali R, White J, Hall W, Farrell M. Proceedings of the expert workshop on induction and stabilisation of patients onto methadone. Monograph series no 39. 2000. Adelaide, Australia. ISBN 0642415080.
- Willner-Reid J, Belendiuk KA, Schmittner JP, Epstein DH, Preston KL. Hepatitis C and HIV risk behaviours in heroin/cocaine users. Journal of Substance Abuse Treatment. 2008.
- Walsh L. Buprenorphine. Accessed August 1, 2019. Last updated 30 Jan 2024. Available at: www.samhsa.gov/medication-assisted-treatment/treatment/buprenorphine.
- Gowing L, Proudfoot H, Henry-Edwards S, Teeson M. Evidence supporting treatment. The effectiveness of interventions for illicit drug use. Woden: Australian National Council on Drugs, 2001.
- Oakley B, Wilson H, Hayes V, Lintzeris N. Managing opioid withdrawal precipitated by buprenorphine with buprenorphine. Drug Alcohol Rev. 2021;40:567-571.
- Perret G, Déglon JJ, Kreek MJ, Ho A, La Harpe R. Lethal methadone intoxications in Geneva, Switzerland, from 1994 to 1998. Addiction. 2000;95(11):1647-53.
- Zador D, Sunjic S. Deaths in methadone maintenance treatment in New South Wales, Australia 1990-1995. Addiction. 2000;95(1):77-84.
- Chalana H, Sachdeva J K, Kundal T, Malhari AS, Choudhary R. A double blind, placebo controlled, randomised study comparing Quetiapine with placebo, along with oral Naltrexone, in the treatment of opioid dependent patients. J Evol Med Dent Sci. 2015;4(53):9158-9167.
- Strain EC, Lofwall MR, Jaffe JH. Opioid related disorders. In: Sadock B J, Sadock V A, Ruiz P, editors. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry. 9th. Lippincott Williams & Wilkins; 2009.
- Farrell, M, Barry J. The introduction of the opioid treatment protocol. 2010. Dublin: Health Service Executive. Social Inclusion Unit. Available at: www.lenus.ie/bitstream/handle/10147/120849/IntrodoftheOpioidTreaTProtocol.pdf.
- Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse: Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264:2511-2518.
- Cole ES, DiDomenico E, Cochran G, et al. The role of primary care in improving access to medication-assisted treatment for rural Medicaid enrollees with opioid use disorder. J Gen Intern Med. 2019;34:936-943.
- Neumann AM, Blondell RD, Azadfard M, Nathan G, Homish GG. Primary care patient characteristics associated with completion of six-month buprenorphine treatment. Addict Behav. 2013;38:2724-2728.
- Marcovitz DE, McHugh RK, Volpe J, Votaw V, Connery HS. Predictors of early dropout in outpatient buprenorphine/naloxone treatment. Am J Addict. 2016;25:472-477.









Leave a Reply
You must be logged in to post a comment.