







Reference: May-June 2026 | Issue 3 | Vol 19 | Page 19
Start this Module
Module Title
Male LUTS: Assessment and managementModule Author
Lynn CaseyCPD points
2Module Type
Clinical ArticleLower urinary tract symptoms (LUTS) are a common complaint in adult men. They often have a major impact on quality of life (QoL) and carry a substantial economic burden. The understanding of the lower urinary tract as a functional unit, and the multifactorial aetiology of associated symptoms, means that LUTS now constitute the main focus, rather than the former emphasis on benign prostatic hyperplasia (BPH).1
The term BPH is now regarded as inappropriate as it is benign prostatic obstruction (BPO) which is treated if the obstruction is a significant cause of a man’s LUTS.1
In this module, you will receive best practice guidance on:
✽ Causes and symptoms of LUTS
✽ Clinical assessment
✽ Diagnostic evaluation
✽ Disease management.
Symptoms and causes
LUTS can be divided into storage, voiding, and post-micturition symptoms (Table 1), and are prevalent, cause bother, and impair QoL. LUTS are strongly associated with ageing. Associated costs and burden are therefore likely to increase with future demographic changes.2
| STORAGE SYMPTOMS | VOIDING SYMPTOMS |
|---|---|
| Urgency | Weak urinary stream |
| Frequency | Intermittent urinary stream |
| Urgency incontinence | Straining |
| Nocturia | Hesitancy |
| Terminal dribbling | |
| Incomplete emptying |
TABLE 1: Classification of LUTS
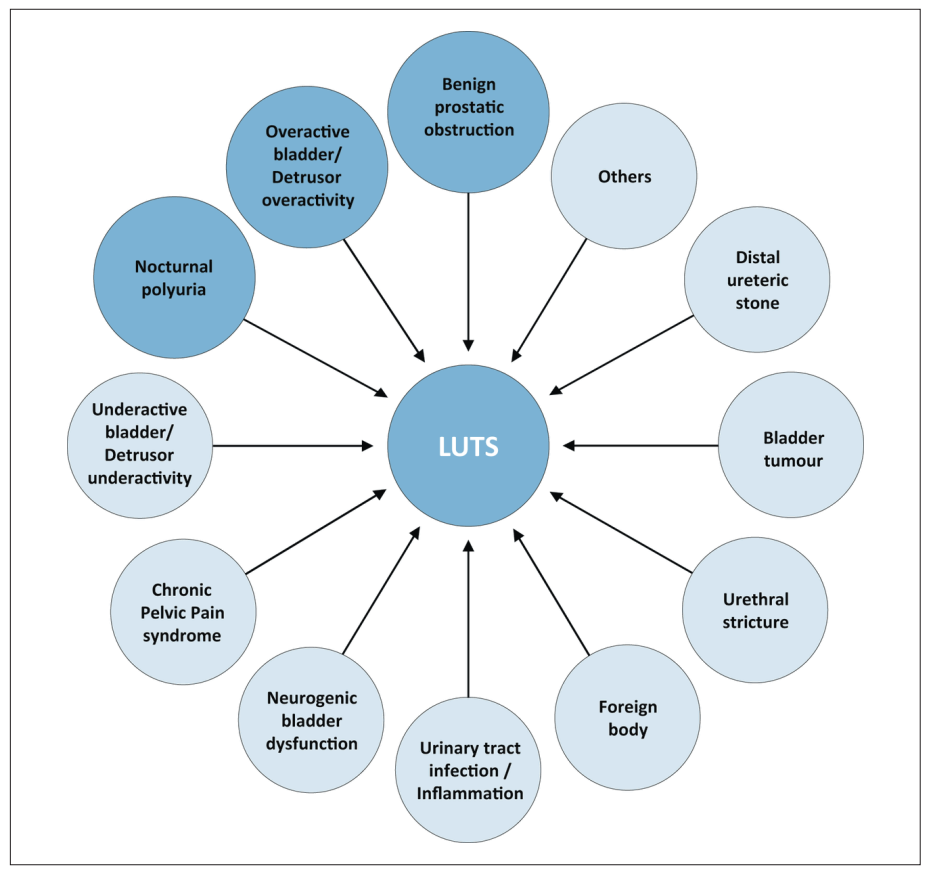
Figure 1 illustrates the potential causes of LUTS. It is common for more than one of these factors to
be present.1 Some of the more common conditions related to male LUTS include:
✽ Acute retention of urine is defined as a painful, palpable, or percussible bladder when the patient is unable to pass any urine.2,3
✽ Chronic retention of urine is defined as a non-painful bladder which remains palpable or percussible after the patient has passed urine. Such patients may be incontinent.2,3
✽ Bladder outlet obstruction (BOO) is the generic term for obstruction during voiding and is characterised by increasing detrusor pressure and reduced urine flow rate. It is usually diagnosed by invasive urodynamic or pressure/flow studies.2,3
✽ Benign prostatic obstruction is a form of BOO and may be diagnosed when the cause of outlet obstruction is known to be benign prostatic enlargement.2,3
✽ BPH is a term used (and reserved) for the typical histological pattern which defines the disease.
LUTS can progress dynamically – for some they persist and progress, for others they remit. Given the many potential causes, an individual assessment is paramount. No one solution fits all.
Clinical assessment
Clinical assessment has two main objectives:
1. Identify differential diagnosis, noting the origin of LUTS is often multifactorial.
2. To define the clinical profile of men with LUTS in order to decide on appropriate care.
A thorough medical history aims to identify potential causes and relevant co-morbidities and must include current medications, lifestyle habits, emotional, and psychological factors. Physical examination focusing in particular on the suprapubic area, the external genitalia, the perineum, and lower limbs should be performed. Urethral discharge, meatal stenosis, phimosis, and penile cancer must be excluded.1
Digital rectal examination (DRE) is the simplest way to assess prostate volume, but the relationship to prostate volume is poor. It may help to differentiate BPO from prostate cancer, prostatitis, or other conditions. It is relatively subjective and examiner dependant – despite this, it is a strong recommendation in the European Association of Urology guidelines that a DRE is performed as part of the physical examination in the assessment of male LUTS.
Urinalysis must be included in the primary evaluation of any patient presenting with LUTS to identify conditions such as urinary tract infections (UTI), microhaematuria, and diabetes mellitus. In most guidelines, urinalysis is recommended in the primary management of patients with LUTS.4 Limited evidence is available, but general expert consensus suggests that the benefits outweigh the costs.5
All published guidelines recommend using a validated symptom score questionnaire1 and there are many available: The International Prostate Symptom Score (IPSS), the International Consultation on Incontinence Questionnaire for Male Luts, and Danish Prostate Symptom Score. The IPSS is probably the most widely used questionnaire (Figure 2).
The IPSS is an eight-item questionnaire consisting of seven symptom questions and one QoL question.6 The score is categorised as ‘asymptomatic’ (0 points), ‘mildly symptomatic’ (1-7 points), ‘moderately symptomatic’ (8-19 points), and ‘severely symptomatic’ (20-35 points). Limitations include lack of assessment of incontinence, post-micturition symptoms, and bother caused by each separate symptom.
Bladder diaries/ frequency volume charts are also useful tools to aid assessment, and there are many available on the internet for use. Volumes in, out, and urine leakage (+/- activity) can be recorded. The recording duration needs to be long enough to avoid sampling error, but short enough to avoid non-compliance; most literature recommends three days.7
The European guidelines also suggest a prostate-specific antigen (PSA) blood test, but only after the patient is counselled, as well as a renal profile if renal impairment is suspected based on history and clinical exam. Radiological imaging is not suggested in the initial phase of assessment.1
Diagnostic assessment
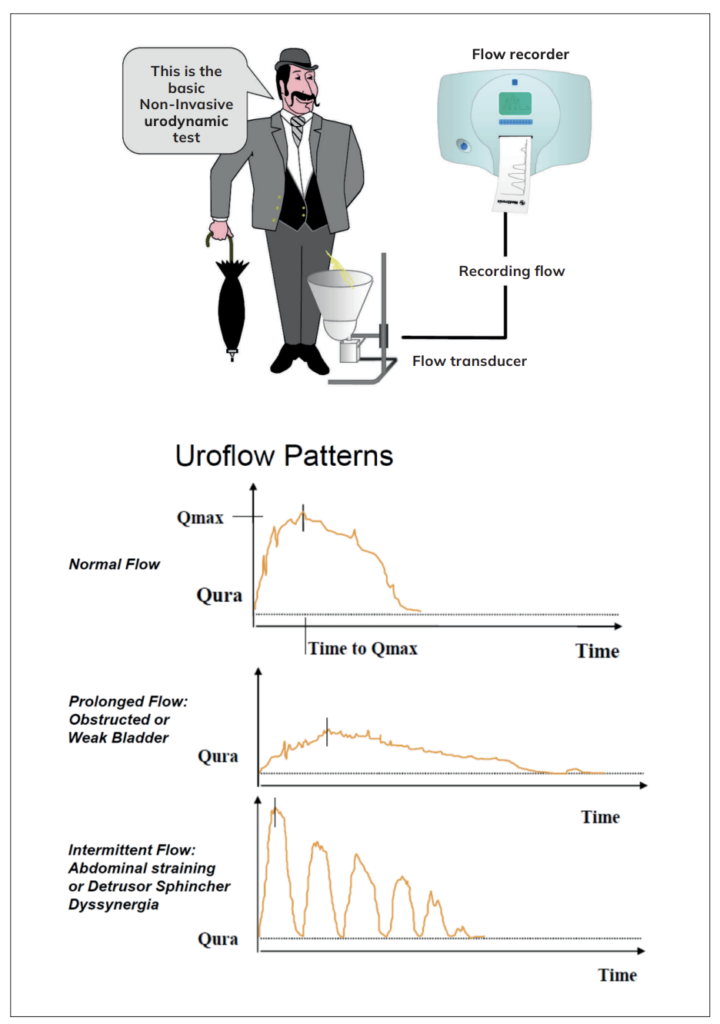
Urinary flow rate assessment is a widely used non-invasive urodynamic test. Key parameters are Qmax, voided volume, and flow pattern. Uroflowmetry parameters should preferably be evaluated with voided volume >150mL. It is also an excellent baseline test to assess treatment effect. It should always be followed by a post void residual bladder scan.
A post-void residual (PVR) scan uses ultrasound to measure how much urine is left in the bladder post void. It is a quick, painless, non-invasive test. High PVRs signal incomplete emptying, pointing to issues like obstruction, nerve damage, or weak bladder muscles, and can lead to UTIs if untreated.
Monitoring of changes in PVR over time may allow for identification of patients at risk of acute urinary retention (AUR) and in both the MTOPS and ALTESS studies, a high baseline PVR (PVR of ≥350mL) was associated with an increased risk of symptom progression.8,9
The European guidelines also suggest a PSA blood test, but only after the patient is counselled and a renal profile, if renal impairment is suspected based on history and clinical exam. Radiological imaging is not suggested in the initial phase of assessment.1
| International Prostate Symptom Score (I-PSS) | |||||||
|---|---|---|---|---|---|---|---|
| Patient Name: ___________________ Date of birth: ___________________ Date complete: ___________________ | |||||||
| In the past month: | Not at all |
Less than 1 in 5 times |
Less than half the time |
About half the time |
More than half the time |
Almost always |
Your score |
| 1. Incomplete emptying. How often have you had the sensation of not emptying your bladder? | 0 | 1 | 2 | 3 | 4 | 5 | |
| 2. Frequency. How often have you had to urinate less than every two hours? | 0 | 1 | 2 | 3 | 4 | 5 | |
| 3. Intermittency. How often have you found you stopped and started again several times when you urinated? | 0 | 1 | 2 | 3 | 4 | 5 | |
| 4. Urgency. How often have you found it difficult to postpone urination? | 0 | 1 | 2 | 3 | 4 | 5 | |
| 5. Weak stream. How often have you had a weak urinary stream? | 0 | 1 | 2 | 3 | 4 | 5 | |
| 6. Straining. How often have you had to strain to start urination? | 0 | 1 | 2 | 3 | 4 | 5 | |
| None | 1 time | 2 times | 3 times | 4 times | 5 times | ||
| 7. Nocturia. How many times did you typically get up at night to urinate? | 0 | 1 | 2 | 3 | 4 | 5 | |
| Total I-PSS Score | |||||||
| Score: 1-7: Mild, 8-19: Moderate, 20-35: Severe | |||||||
| Quality of Life Due to Urinary Symptoms |
Delighted | Pleased | Mostly Satisfied |
Mixed | Mostly Dissatisfied |
Unhappy | Terrible |
|---|---|---|---|---|---|---|---|
| If you were to spend the rest of your life with your urinary condition just the way it is now, how would you feel about that? | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
FIGURE 2: IPSS Questionnaire
Management
Management of male LUTS is stepwise and generally depends on symptom severity, bother, and complications. A sufficient clinical and diagnostic assessment (as described) prior to any allocation of treatment to establish symptom severity and potential risks is essential. The three types of management are conservative management, pharmacological management, and surgical management.
Conservation management can be split into two categories:
1. Watchful waiting: Many men with LUTS are not troubled enough by their symptoms to require drug treatment or surgical intervention. Watchful waiting is a viable option for many men with non-bothersome LUTS, as few will progress to AUR and complications (eg, renal insufficiency or stones)1 whilst others can remain stable for years.
In one study, approximately 85 per cent of men with mild LUTS were stable on watchful waiting at one year.10 Increasing symptom bother and PVR volumes are the strongest predictors of watchful waiting failure.
| RECOMMENDATIONS | STRENGTH RATING |
|---|---|
| Offer watchful waiting to men with mild/moderate LUTS who are minimally bothered by their symptoms. | Strong |
| Offer men with LUTS lifestyle advice and self-care information prior to, or concurrent with, treatment. | Strong |
TABLE 2: Recommendations from the European guidelines1
2. Behavioural and dietary modifications: From a nursing perspective, it is essential for this type of management to include education, reassurance, and periodic management. Lifestyle advice is essential on concerning topics such as:1,11
✽ Reduction of fluid intake at specific times aimed at reducing urinary frequency when most inconvenient (eg, at night or when going out in public).
✽ Avoidance/moderation of intake of caffeine or alcohol, which may have a diuretic and bladder irritant effect, thereby increasing fluid output and enhancing frequency, urgency, and nocturia.
✽ Use of relaxed and double-voiding techniques
✽ Urethral milking to prevent post-micturition dribble.
✽ Distraction techniques, like penile squeeze, breathing exercises, perineal pressure, and mental tricks to take the mind off the bladder and toilet and help control overactive bladder symptoms.
✽ Bladder retraining that encourages men to hold on when they have urgency to increase their bladder capacity and the time between voids.
✽ Reviewing the medication and optimising the time of administration or substituting drugs for others that have fewer urinary effects (these recommendations apply in particular to diuretics).
✽ Providing necessary assistance when there is impairment of dexterity, mobility or mental state.
✽ Treatment of constipation.
Pharmacological management is wide ranging and can be somewhat complex. What follows is a summarised version of available medications, all of which is based on European guidelines.1
Alpha 1-adrenoceptor antagonists (apha-blocker) – moderate to severe LUTS:
✽ Tamsulosin, silodosin, alfuzosin.
✽ Inhibit the effect of noradrenaline on smooth muscle cells in the prostate, reducing prostate tone and BOO.
✽ Typically reduce IPSS by 30-40 per cent, can reduce both storage and voiding LUTS.
✽ Most common side effects include weakness, dizziness, and orthostatic hypotension.
✽ ‘Floppy iris’ – higher risk with tamsulosin.
✽ Do not affect erectile function or libido.
✽ Decreased or absence of seminal fluid during ejaculation.
5-alpha reductase inhibitors – moderate to severe LUTS with an increased risk of progression:
✽ Dutasteride, finasteride.
✽ By preventing the intraprostatic conversion of testosterone to the more potent androgen dihydrotestosterone, these medications reduce prostate volume and relieve urinary outflow obstruction.
✽ Apoptosis of prostate cells leading to prostate size reduction.
✽ Reduce long-term risk of acute urinary retention.
✽ Most common side effects include reduced libido, erectile dysfunction, and less commonly gynaecomastia.
Muscarinic receptor antagonists – moderate to severe LUTS, mostly bladder storage symptoms:
✽ Solifenacin, tolterodine, oxybutynin
✽ Stimulates muscarinic receptors on the smooth muscle cells – bladder urothelial cell, epithelial cells of the salivary gland
✽ Do not use in PVR >150mls
✽ Most common side effects include dry mouth, constipation, and micturition difficulties.
Beta-3 agonist:
✽ Mirabegron
✽ Thought to induce detrusor relaxation through stimulation of smooth muscle cells, mode of action is not fully elucidated
✽ Most common side effects include hypertension, UTI, and headache.
Phosphodiesterase 5 inhibitors:
✽ Tadalafil is only licensed for the treatment of male LUTS
✽ Reduce muscle tone of the detrusor, prostate, and urethra. Longer treatment seems to increase blood perfusion and oxygenation in the lower urinary tract
✽ Contraindicated in patients using nitrates, severe cardiac disease, and/or recent myocardial infarction.
Combination therapies:
✽ Alpha blocker + 5 alpha reductase inhibitors
✽ Alpha blocker + muscarinic receptor antagonists
✽ Alpha blocker + beta 3 agonist.
Surgical intervention
Surgical treatment is one of the cornerstones of LUTS management and is usually considered when symptoms are moderate to severe, persistent, and do not respond to lifestyle modifications or pharmacological management.1
There are various surgical options and the treatment decision may depend on prostate size, symptom severity, patient’s age and health, and desired preservation of ejaculation/sexual function. Options may also depend on the hospital or urologist the patient attends. Below is a summary of the more common surgical options (not exhaustive).1
Transurethral resection of the prostate:
✽ Prostate gland of 30-80ml
✽ Endoscopically removes tissue from the transition zone of the gland in various degrees resulting
in a volume and PSA reduction of 25-58 per cent.1
✽ Possible post-operative complications can include urethral stricture, bladder neck contracture, retrograde ejaculation.
Open prostatectomy:
✽ Is the oldest surgical treatment, used mostly for substantially enlarged glands (>80ml).
✽ Adenomas are enucleated, approaching from within the bladder (Freyer procedure) or through the anterior prostatic capsule (Millin procedure).
Bipolar transurethral enucleation of the prostate:
✽ Following the principles of bipolar technology, the obstructive adenoma is enucleated endoscopically by the transurethral approach.
Holium laser enucleation:
✽ Is a pulsed solid-state laser that is absorbed by water and water-containing tissues. Tissue coagulation and necrosis are limited to 3-4mm which obtains adequate haemostasis.
Prostatic urethral lift: The UroLift device delivers tiny stainless-steel implants that lift or hold the enlarged prostate tissue out of the way so that it no longer blocks the urethra.
Intra-prostatic injections: These compounds are injected deep into the prostate to elicit either a chemical irritant response or initiate cellular apoptotic pathways that result in ablation of prostatic tissue. Transurethral ethanol ablation of the prostate is one such method involving injection of pure ethanol.
Follow-up for all management strategies
Watchful waiting/ behavioural modifications: Review at six months and then annually.
Medical treatment: Review four to six weeks after drug initiation, then at six months, and then annually. For 5-alpha reductase inhibitors, review at 12 weeks, then six months. Monitor PSA.
Surgical treatment: Review at four to six weeks and then discharge if appropriate.
Conclusion
In conclusion, management of male LUTS follows a stepwise approach based on symptom severity and patient impact. Conservative measures are appropriate for mild symptoms, while pharmacological therapies may be required for moderate cases. Surgical intervention remains an important option for severe or refractory symptoms, ensuring symptom relief and prevention of complications.
Nurses play key roles like assessing symptoms, aiding diagnosis, and monitoring treatment response. They provide patient education on lifestyle changes and medication management and also support patients post-intervention, identifying complications early, and promoting recovery.
References
- European Association of Urology. EAU Guidelines on the Management of Non-neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO). Arnhem, The Netherlands: EAU Guidelines Office; 2024. Available at: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts.
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167-178. doi:10.1002/nau.10052.
- Roehrborn CG. Male lower urinary tract symptoms (LUTS) and benign prostatic hyperplasia (BPH). Med Clin North Am. 2011;95(1):87-100. doi:10.1016/j.mcna.2010.08.013.
- Abrams P, Chapple C, Khoury S, et al. International Consultation on New Developments in Prostate Cancer and Prostate Diseases. Evaluation and treatment of lower urinary tract symptoms in older men. J Urol. 2013;189(1 Suppl):S93-S101. doi:10.1016/j.juro.2012.11.021.
- European Confederation of Laboratory Medicine. European urinalysis guidelines. Scand J Clin Lab Invest Suppl. 2000;231:1-86. Available at: www.ncbi.nlm.nih.gov/pubmed/12647764.
- Barry MJ, Fowler FJ Jr, O’Leary MP, et al. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992;148(5):1549-1564. doi:10.1016/s0022-5347(17)36966-5.
- Yap TL, Cromwell DC, Emberton M. A systematic review of the reliability of frequency-volume charts in urological research and its implications for the optimum chart duration. BJU Int. 2007;99(1):9-16. doi:10.1111/j.1464-410X.2006.06499.x.
- McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349(25):2387-2398. doi:10.1056/NEJMoa030656.
- Roehrborn CG. Alfuzosin 10mg once daily prevents overall clinical progression of benign prostatic hyperplasia but not acute urinary retention: Results of a two-year placebo-controlled study. BJU Int. 2006;97(4):734-741. doi:10.1111/j.1464-410X.2006.06110.x.
- Netto NR Jr, de Lima ML, Netto MR, D’Ancona CA. Evaluation of patients with bladder outlet obstruction and mild international prostate symptom score followed up by watchful waiting. Urology. 1999;53(2):314-316. doi:10.1016/s0090-4295(98)00475-0.
- Yap TL, Brown C, Cromwell DA, et al.
The impact of self-management of lower urinary tract symptoms on frequency-volume chart measures. BJU Int. 2009;104(8):1104-1108. doi:10.1111/j.1464-410X.2009.08497.x.










Leave a Reply
You must be logged in to post a comment.