







Reference: May-June 2025 | Issue 3 | Vol 18 | Page 18
Skin cancer has become the most common form of cancer in Ireland, with incidence rates rising significantly during the past two decades. According to the National Cancer Registry Ireland,1 the number of skin cancer cases has nearly doubled in the last 20 years, driven by both an ageing population and increased exposure to ultraviolet radiation from outdoor activities and artificial sources like sunbeds. Non-melanoma skin cancers (NMSC), particularly basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), account for the majority of cases, while melanoma, though less common, remains the deadliest form of skin cancer.1
This sharp rise in skin cancer diagnoses has placed substantial pressure on an already burdened
Irish healthcare system. Hospitals, general practice, and specialist clinics are experiencing increasing demand for services, leading to growing waiting lists for consultations, biopsies, and treatments.
These delays can negatively affect both diagnosis and treatment outcomes for patients.1,2 The HSE has acknowledged these challenges and has emphasised the need for targeted interventions to reduce waiting times, increase service capacity, and optimise patient outcomes.
While public awareness of sun safety and enhanced early detection of skin cancer are vital elements for improving skin cancer outcomes in Ireland, optimal curative treatment of the disease is surgical excision.3 The advanced nurse practitioner (ANP) is ideally placed to deliver all of these targeted strategies. This article provides an overview of an ANP-led service based on the ‘see-and-treat’ model of care for skin cancer, following the success of a see-and-treat model of skin cancer management in Roscommon University Hospital (RUH).
The see-and-treat model
A see-and-treat model for skin cancer is an innovative approach aimed at improving the efficiency and effectiveness of disease management.4,5 It involves the examination, possible biopsy, and excision of the affected area under local anaesthesia – providing patients with a consultation, diagnosis, and, where appropriate, treatment in a single visit. Given the rising incidence of skin cancer in Ireland, the see-and-treat model has become an integral component of optimal patient care both nationally and internationally.
The UK and other parts of Europe have implemented the model with notable success. Data suggests the see-and-treat approach significantly reduces waiting times, improves patient outcomes, optimises healthcare resources, and offers a sustainable solution to the increasing burden of skin cancer – particularly in countries like Ireland, where the demand for skin lesion management services continues to grow.4,6
The see-and-treat model of care was implemented successfully at RUH in 2011 and has expanded exponentially since then in view of its positive impacts.
Background
In 2019, a pilot see-and-treat clinic was established by the plastic surgery service at Merlin Park University Hospital Galway to deal with the ever-increasing waiting lists for plastic surgery services. Staffing of the pilot clinic at that time consisted of a consultant plastic surgeon, a plastic surgery ANP, and either a plastic surgery registrar or senior house officer. Patients were assessed and surgery was undertaken if required under local anaesthetic all in the same day, which in some cases completed the entire episode of care for the patient.
The pilot clinic at that time demonstrated positive results, but due to the impact of Covid-19, progression of the initiative was halted and the unit was used to meet pandemic demands. Following a return to normal hospital activity, the clinic became both operational again, and ANP-led.
The number of plastic surgery ANPs in the see-and-treat service at Galway University Hospital (GUH) was increased from one to three, and qualified plastic surgery ANPs from RUH would attend the clinic alongside GUH ANPs to operate as an ANP-led service – affording the opportunity to train the new ANP recruits and provide experienced practitioners to oversee the service.
ANP-led services
The ANP-led see-and-treat clinic formally commenced in June 2023, operating on a one-day-a-week basis. The service is operated by two ANPs and a candidate ANP on one day, and three ANPs and two ANP candidates on the second day. It is further supported by two RGNs, as well as one healthcare assistant, and one clerical staff.
Referrals to the clinic come via triaged referral letters from the consultant plastic surgeons. The ANPs complete the episodes of care for the patients independently, from assessment and diagnosis to performing the surgical excisions if needed. Patients are seen and treated in one single visit, significantly reducing the number of visits required for each patient as well as waiting times for review and management.
Patients receive a holistic, in-depth consultation from the ANP. A history is taken and full body examinations using dermoscopy are carried out where deemed appropriate, for example, patients with a known history of skin cancer, patients with multiple naevi, a history of previous NMSCs, or a history of excessive sun exposure or sunbed use. With the aid of dermoscopy, a clinical diagnosis is made and a decision on appropriate treatment is formulated with the patient, whether that means no treatment, topical therapies, or surgical intervention.
Suspicious lesions are excised on the same day under local anaesthetic with patient consent. In cases where the lesion is too large for excision under local anaesthetic or if the specific procedure falls outside the scope of the ANP, a biopsy is taken and the patient is referred back to the consultant for further management.
In cases of benign lesions, patients are educated about the risks and benefits of surgery or no surgery, and are encouraged to take time to consider future options. These patients can be booked back on another day for surgery. In cases where lesions are benign, but interfering with a patient’s quality of life, excision can take place on the same day. Follow-up is offered to patients when indicated and close liaison with the consultant is maintained.
Results
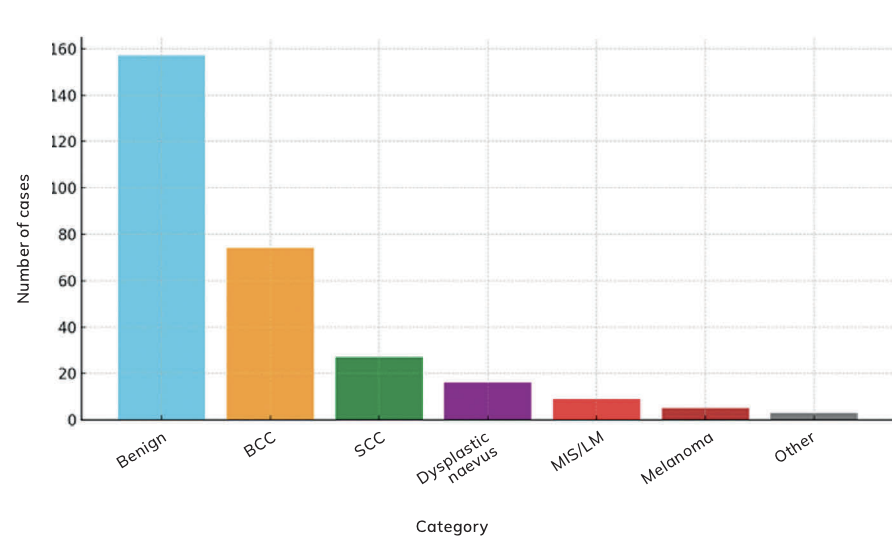
From June 2023 to June 2024, 760 new patients attended the see-and-treat service. A total of 291 patients underwent excision of lesions. Some patients had more than one lesion excised. Benign lesions made up 157 of these, while 134 were either skin cancer or an in situ carcinoma – 74 were BCCs, 27 were SCCs, nine were melanoma in situ (MIS) or lentigo maligna (LM), five were melanoma, 16 were dysplastic naevi, and three were other skin cancers (Figure 1).
In total, five skin cancers were incompletely excised, giving a histological clearance rate of 94 per cent. Overall, patients report high levels of satisfaction with the service and the next step in the evaluation process is to obtain a formal patient satisfaction survey.
Discussion
In conventional care pathways, patients with suspected skin cancer often face long waits for specialist referrals, diagnostic procedures, and treatment. This delay can increase anxiety and, in some cases, allow cancer progression.7,8 The ANP-led clinic addresses these issues by providing same-day consultations, diagnostics, and interventions. Patients are seen promptly, diagnosed, and treated on the same day where possible. This streamlined approach ensures that even one-day-a-week operations can address high patient volumes effectively, while increasing the number of clinic days could substantially amplify the positive impacts.
Traditional models rely heavily on specialist availability, often creating bottlenecks in services. By empowering ANPs to lead clinics, healthcare systems can alleviate pressure on plastic surgery consultants, freeing them to handle more complex cases and promoting more efficient use of existing resources.5
The success of this ANP-led clinic highlights the potential for scaling the model across different regions or specialties. Operating just one day per week, the clinic achieved impressive results, which suggests that increasing the number of clinic days could substantially amplify its impact. Furthermore, this model can be adapted to underserved areas, improving healthcare equity by offering accessible and timely care.
This clinic also demonstrates how ANPs can perform diagnostic procedures and minor surgical treatments competently, provide patient education, and manage non-surgical treatments – thus enhancing continuity and quality of care.
Early detection and treatment of skin cancers is critical to improving survival rates and reducing morbidity.4,7,9 The clinic’s ability to confirm 134 cancers in its first year underscores its role in facilitating early intervention, particularly in high-risk populations.
Compared to traditional models, nurse-led clinics may reduce overall healthcare costs by:
- Minimising unnecessary referrals;
- Reducing the number of appointments per patient;
- Lowering hospital admissions due to delayed diagnoses.
The success of this ANP-led service in its first 12 months has led to the clinic being opened for a second see-and-treat day in the week. Additionally, there are two days allocated for reviews and dressing clinics and the option for plastic surgery consultants to send urgent referrals from the outpatient department for biopsy or excision.
The addition of these extra days will ultimately allow for an increase in numbers that can be seen and treated each week. This should lend to an increase in the capacity for the ANPs to see and treat new patients on an ongoing basis, further contributing to a reduction in the waiting lists for plastic surgery patients and those with skin cancer.
While the benefits of the see-and-treat model are evident, challenges do remain and have been highlighted throughout the literature. One concern is the potential for overtreatment, where benign lesions are excised unnecessarily in the effort to expedite care.8 Additionally, the model requires significant initial investment in training healthcare professionals and ensuring that appropriate diagnostic tools and surgical equipment are available.8
Another challenge is the potential for incomplete excisions when cases are treated too quickly, though studies from UK clinics have shown that incomplete excision rates in these settings are comparable to traditional pathways,8,10 and the results locally indicate that this is not a concerning risk.
Additionally, the literature suggests that the model may not always provide patients sufficient time to process information and consider their options before consenting to treatment. This could lead to ethical and legal challenges if patients later feel they were pressured into making quick decisions without adequate understanding.6,8
Furthermore, evidence illustrates that although the model aims to reduce anxiety by addressing issues promptly, some patients may find the immediacy of treatment stressful, and may prefer additional time to consult with family or seek second opinions.8 Therefore, we acknowledge the application of see-and-treat must be carefully balanced with considerations of clinical accuracy, patient autonomy, and ethical standards.
Contextual adaptations and safeguards, like initial diagnostic consultations for benign lesions, can mitigate some of these concerns. Scheduling surgery at a later date for benign lesions also allows patients time to understand their condition fully and make informed decisions about their treatment options.4,8 This is critical for ensuring informed consent, reducing anxiety, and affording opportunities to explore alternative treatments or lifestyle modifications.
However, same-day surgery is highly beneficial for malignant lesions as it minimises delays in treatment, which can reduce the risk of tumour progression, improve survival outcomes, and alleviate patient stress associated with waiting.4,8 This approach also enhances healthcare efficiency by reducing the need for multiple appointments, saving resources, and improving access for other patients.
Conclusion
Overall, see-and-treat models can improve patient satisfaction and clinical outcomes when appropriately tailored to the urgency of the condition and patient wishes. The first-year outcomes of the ANP-led see-and-treat clinic in plastic surgery demonstrate a highly effective and patient-centred approach to skin cancer care.
By combining accessibility, efficiency, and high-quality clinical care, this model has set a new standard for addressing a growing public health challenge, and played a critical role in early detection and treatment for many patients. Its scalability and resource efficiency make it a valuable template for broader healthcare reform.
This achievement underscores the efficiency and quality of care provided by the ANPs, contributing
to better patient outcomes and a streamlined pathway for skin cancer management.
References
- National Cancer Registry Ireland. Annual Report on Cancer Incidence in Ireland. Ireland: NCRI; 2021. Available at: www.ncri.ie/publications/statistical-reports.
- Health Service Executive. Dermatology Services and Waiting List Reduction Strategy. Dublin: HSE; 2023. Available at: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.hse.ie/eng/about/who/acute-hospitals-division/waiting-list-action-plans/2023-waiting-list-action-plan-end-of-year-report.pdf.
- British Association of Dermatologists. Guidelines for Skin Cancer Management. UK: BAD; 2023. Available at: www.bad.org.uk/guidelines-and-standards/clinical-guidelines/.
- Nolan K, O’Donnell K, Moloney FJ, Kelly CM, Potter S. The impact of a see and treat clinic on skin cancer treatment time. J Plast Reconstr Aesthet Surg. 2022;75(2):893-939.
- University Hospital of Heidelberg, 2021. Innovations in nurse-led dermatology care: The see and treat model. Available at: www.heidelbert-university-hospital.com.
- Karolinska University Hospital, 2019. Early Skin Cancer Detection and Treatment Programme. Available at: www.karolinskahospital.com.
- Department of Health. National Cancer Strategy 2017-2026. Available at: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://assets.gov.ie/9315/6f1592a09583421baa87de3a7e9cb619.pdf.
- Guy’s and St Thomas’ NHS Foundation Trust, 2018. Skin Cancer See and Treat Service: Annual Report. Available at: www.guysandstthomas.nhs.uk.
- Irish Cancer Society. Skin Cancer Awareness and Prevention. Ireland: ICS; 2022. Available at: www.cancer.ie
- O’Hare C, McKeough M, Hickson M, Ferris R, Wiper J, Wagels M. Skin lesion assessment and management model: Optimising existing resources in the management of non-melanoma skin cancer. AJOPS. 2022;5(1):88-95.










Leave a Reply
You must be logged in to post a comment.