






A recent decision on the location of a major trauma centre in Dublin has generated controversy, but was a big step in the reorganisation of the national trauma service. David Lynch examines what happens next
Change can sometimes be traumatic, but supporters of the national trauma strategy believe the restructuring of the system will prove significantly beneficial to patients.
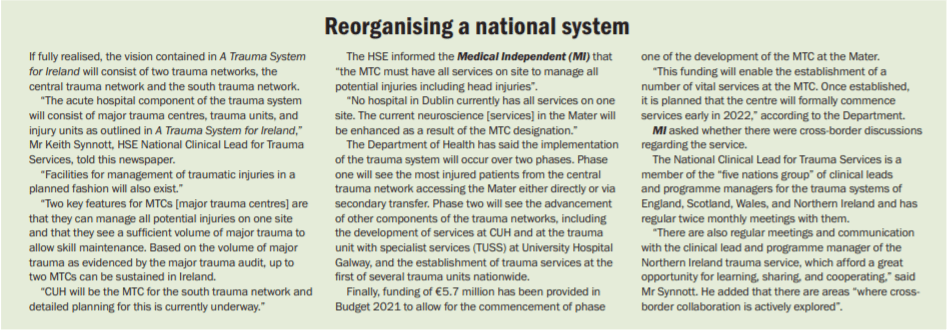
A Trauma System for Ireland was published in 2018. According to the HSE, it took “a whole-system approach addressing all elements of the trauma care pathway including prevention, pre-hospital care, acute hospital care, rehabilitation and supported discharge”.
The report recommended the establishment of an “inclusive trauma system”, where a network of facilities and services co-ordinate in the care of injured patients along standardised pathways.
The report recommended the establishment of an “inclusive trauma system”, where a network of facilities and services co-ordinate in the care of injured patients along standardised pathways.
The full implementation of the strategy will result in a series of changes to the way the trauma system is structured in Ireland (see panel below).
Major trauma involves complex injuries that have the potential to cause prolonged disability or death. The Department of Health estimates that around 1,600 patients a year in Ireland suffer major trauma.
In April, the Government announced the designation of the Mater Misericordiae University Hospital in Dublin as the major trauma centre (MTC) for the central trauma network. Cork University Hospital (CUH) was already identified as the MTC for the south trauma network.
The announcement of the Mater Hospital as the Dublin site sparked some criticism in regard to neurosurgery provision. Neurosurgeons in Beaumont Hospital, where the national neurosurgical centre is located, believe the national neurosurgical centre needs to be co-located with the MTC. (see panel on page 5). The Government also announced St Vincent’s University Hospital and Tallaght University Hospital as the trauma units for the greater Dublin area.
“International studies have consistently shown that concentrating the care of severely injured patients in dedicated MTCs is associated with improved access to care, reduced length of stay and demonstrably better outcomes for patients,” according to the HSE.
A trauma system is both complicated and
simple, in that it touches everything. It has
the capacity to improve other aspects of care
Outcomes
The planned changes to the national trauma system are “very exciting” and “proven to improve outcomes and can have far-reaching effects beyond the headline act of major trauma”, Mr Keith Synnott, HSE National Clinical Lead for Trauma Services and Consultant Orthopaedic and Spine Surgeon at the National Spinal Injuries Unit in the Mater Hospital, told the Medical Independent (MI).

“What we are trying to do is to replicate a system that has been put in place around the world which has been proven to improve survival rates from trauma.”
He said these international systems have been shown to improve survival rates by up to 20-to-30 per cent. Such improvements have been “immediate” and continue “year-on-year”. He added that, with every person that survives, there are more people who “avoid significant long-term disability”.
Mr Synnott said the proposed changes to the trauma system will have positive impacts on the wider health service.
He maintained that this knock-on impact is due to the fundamental “team work” that is a feature of trauma care.
“Trauma can be unpredictable, but [it’s] typically multi-system,” he said.
“Coordinating things is very important. Trauma is a team game so treating trauma, and especially severe trauma, is all about team work, co-operation, coordination with the ambulance service, the emergency department, the x-ray department, the operating department, ICU, orthopaedic, neurosurgeons, general surgeons, and others. It’s all about team work and coordination.”
“I used to think spine surgery and spine trauma is really important, because it’s what I do. And it is really important. But there is no point just fixing someone’s spine, if they have head injuries [as well] or chest injuries. Everything is about team work.”
The HSE national lead believes that when the trauma strategy is fully implemented, patients “regardless of their location or severity of injury” will receive the highest possible standard of care in the most appropriate healthcare facility.
The HSE predicts the implementation of A Trauma System for Ireland will take five-to-seven years.
Key step
In April, the Irish Association for Emergency Medicine (IAEM) “warmly” welcomed what it described as the “long-awaited” announcement of the location of the MTCs.
“It’s an important step, it’s a key step, but it doesn’t end at that point,” Dr Fergal Hickey, IAEM President, told MI.

“There is a series of recommendations in the report [A Trauma System for Ireland], which we would like to see implemented, sooner rather than later. This is going to require funding and staffing and a degree of service reorientation and
and reconfiguration to facilitate it and the sooner those things happen the better.”
Dr Hickey said that the IAEM is “as supportive as ever” of the creation of a national trauma system.
“We’ve been pushing this from the very beginning. We produced a position paper in 2014, where we basically called for a national trauma system. The expert
group report, which came out subsequently, is very similar to our particular position paper.”
However, Dr Hickey said there was
significant frustration with the pace of
implementation.
“Like lots of people we share frustrations that the speed [of] the central decision-making process is not as quick and efficient as it should be,” he said.
“Our biggest frustration is the amount of time it has taken to get to this point. Clearly, we ran into a lot of problems: Having no Government for an extended period of time [in early 2020], then Covid arrived and it has essentially taken over pretty much everything
“So yes, we have designations, we have agreements to implement. But we need to get on and implement it.”
In April, the IHCA President Prof Alan Irvine described the announcement of the proposed development of trauma services as “welcome and long overdue”
“International experience has shown that the development of such trauma services improves survival rates for patients sustaining major trauma by up to 25 per cent and also leads to dramatically improved outcomes for those who suffer such trauma or injury,” he added.
However, he warned that the “hospital consultant recruitment and retention crisis” poses a significant challenge to the implementation of the trauma strategy.
“The recruitment of consultants to lead and manage trauma care will be challenging given the nature of the work (24/7) and the complexity involved,” an IHCA spokesperson told MI.
“In addition, a significant number of consultants are required to staff the MTCs and trauma units and it will take time for them to be recruited and become established….
In that regard, the current consultant contract terms on offer in Ireland will need to be more competitive in several respects if we are going to recruit the required number of consultants for our services.”
The IHCA and the IMO are currently engaged with the Department of Health and HSE regarding the new Sláintecare consultant contract.
The HSE told this newspaper that resources are available for the appointment of consultants in the MTC in Dublin and the “recruitment process is underway”. Preparation for an application for similar resources for the units in CUH and University Hospital Galway (where a trauma unit with specialist services will be opened under the trauma strategy) in the upcoming estimates process has also commenced.
process has also commenced.
“There is anecdotal evidence that working in a trauma system as envisioned for Ireland is attractive to many Irish doctors overseas,” Mr Synnott told MI. “There is a sense of enthusiasm for the system that is very encouraging and it is not felt that recruitment will be an issue.”
While there seems to be a significant level of cross-party support for the aims of the national trauma strategy, in April, the Independent TD for Roscommon-Galway Deputy Denis Naughten raised concerns that improvements to “air ambulance services” and “additional ground ambulance resources” may be
needed to help patients from across the country access the MTCs in Cork and Dublin.
Mr Synnott said the HSE does not see significant issues in relation to the ambulance service. “Resources have been provided for the implementation of trauma by-pass, which has already been successfully piloted and implemented between Naas and Tallaght,”
“Resources have also been made available to progress trauma by-pass in other areas when the system matures to the point where it is feasible. NAS [National Ambulance Service] are involved in the implementation plan so resource requirements can be fully considered.”
Debating a decision
In April, the Government accepted the recommendation of the HSE board that the Mater Hospital be the location of the major trauma centre (MTC) for the central trauma network “following the report of an independent assessment panel comprised of local and international experts”.
Following that announcement, neurosurgeons in Beaumont Hospital raised public concerns over the decision.
In a letter to The Irish Times, published on 5 May, Beaumont neurosurgeons wrote that “as Ireland’s specialists in treating patients with severe head injury, we welcome the news of reform of trauma services in Ireland”.
“International experience clearly demonstrates the benefits of a trauma system of care. We are, however, dismayed at the announcement by the Minister for Health that the central network major trauma centre is to be located at the Mater hospital….” The surgeons wrote that the “international standard is to co-locate the MTC with a major neurosurgical centre”.
The HSE informed the Medical Independent (MI) that, since April, meetings have taken place between the HSE Chief Clinical Officer Dr Colm Henry, National Clinical Lead for Trauma Services Mr Synnott, and the Beaumont neurosurgeons “regarding the best options for further developing this service”.
The option to relocate the national neurosurgical centre in Beaumont
Hospital to the Mater “is one of a
number of options which have been proposed”, Mr Synnott told MI.
“There are various models around the world for the delivery of neurosurgical services in an MTC. These include co-locating all neurosurgery on one site or having a two-site model. There are pros and cons for each approach with multiple things to be considered and the optimal solution is not as binary as is sometimes presented.”
Mr David O’Brien, Consultant Neurosurgeon and Chair of the national neurosurgery centre in Beaumont Hospital, told MI that the neurosurgeons at Beaumont still had significant concerns regarding the selection of the Mater as a site for the MTC. He restated the importance of co-location of the services.
“We would like the national neurosurgery centre to be on the same site as the major trauma centre,” Mr O’Brien explained. The need for the co-location of the national neurosurgery centre and the MTC was a “basic principle”, he outlined. In terms of the general trauma strategy and reform, Mr O’Brien said the trauma system “will improve”. “The focus is on it [trauma services] now, it used to be on cancer, then stroke, etc. Now it’s trauma’s turn. So we have got to do this right. Because, after this, the focus will be on paediatrics or something else. So now is the time to highlight it, to make it [trauma services] better.”
The neurosurgeons at Beaumont had raised concerns prior to the public decision on the MTC. In a letter dated 27 March, Mr Stephen McNally, Clinical Director and Consultant Neurosurgeon at the national centre for neurosurgery, wrote to the Minister for Health Stephen Donnelly “on behalf of all neurosurgeons at the national neurosurgical centre, Beaumont Hospital”
In the correspondence seen by MI following a Freedom of Information request, Mr McNally wrote that his letter was “to highlight our concerns regarding the potential location of the Dublin major trauma centre and to arrange an urgent meeting with you”. He wrote that “we need to bring to your attention additional up to date information”.
“In our previous letter we highlighted the fact that in the UK, only two of 27 MTCs are not co-located with their main neurosurgical centre. We have now been made aware that mortality rates for patients with traumatic brain injury are significantly higher in one of the non-co-located centres compared to co-located MTCs. This mistake must be avoided in Ireland to avoid unnecessary deaths.”
Mr McNally wrote that a second issue was that due to recent advances in technology, “one of our allied specialties (interventional neuroradiology) is becoming critically involved in the treatment of patients with traumatic brain injury.”
“Therefore, if the MTC is not co-located with the current national neurosurgical centre, provisions would be needed to relocate not only neurosurgery, but also interventional neuroradiology (which includes the national thrombectomy service for stroke) to the new MTC site.
“Such a major relocation of services is likely to take several years and any interim solution could put patients’ lives at risk as evidenced by similar models in the UK.”
Mr McNally concluded the letter by stating “this evidence further endorses our opinion that any MTC needs to be co-located with a major neurosurgical centre as in line with international standards”.
On 26 April, Minister Donnelly wrote a reply to Mr McNally.
Minister Donnelly wrote that he was “very happy to confirm that the HSE undertook a clear and objective process to inform the recommendation for the designation [of the MTC], which included a public consultation on the designation framework”
In terms of “patient safety concerns”, the Minister wrote that “data from the NOCA [National Office of Clinical Audit] major trauma audit 2018 shows that of the 1,221 patients who had a head injury of AIS 3 or greater, only 18 per cent went directly to a neurosurgical unit and 19.2 per cent went to a neurosurgical unit following transfer from the original receiving hospital”.
“The clear objective of the national trauma strategy is for all trauma patients to access the treatments they need in a timely manner. “This will be possible through the establishment of two major trauma centres that have all trauma specialties, including neurosurgery. I believe that the availability of all trauma specialties in one hospital will create very significant benefits for patients, including a reduced need for a secondary transfer, as well as reduced waiting times between sequential surgeries.”
The Minister ended his letter by stating that he looked forward to “further engagement with my Department, the
HSE, and you and your colleagues to realise the benefits for patients”.












Leave a Reply
You must be logged in to post a comment.