






This module reviews the epidemiology, pathophysiology, clinical assessment, and medical and surgical management of male LUTS, integrating evidence from major randomised controlled trials and current guideline recommendations
Male lower urinary tract symptoms (LUTS) represent one of the most frequent reasons for consultation in ageing men. Although commonly attributed to benign prostatic hyperplasia (BPH), LUTS are not synonymous with prostatic enlargement and may arise from a variety of pathological processes involving both the bladder and the prostate. Guidelines emphasise that LUTS should be regarded as a functional clinical syndrome rather than a disease entity in itself.1 This distinction is critical, as symptom pattern alone does not reliably identify the underlying pathophysiology or predict response to treatment.
The clinical burden of LUTS extends beyond urinary inconvenience. Symptoms frequently impair sleep, restrict daily activities, and negatively affect quality-of-life. Furthermore, in a proportion of men, LUTS associated with BPH follow a progressive course, culminating in acute urinary retention (AUR) or the need for surgical intervention. Contemporary management therefore requires both symptom control and, where appropriate, modification of disease progression risk.
Epidemiology and pathophysiology
Histological BPH is highly prevalent in ageing men. Approximately half of men aged 50 years have histological evidence of prostatic hyperplasia, rising to around 80 per cent by 80 years of age.7,8 However, the presence of histological hyperplasia does not necessarily correlate with symptom severity, nor does prostate size alone determine obstruction.

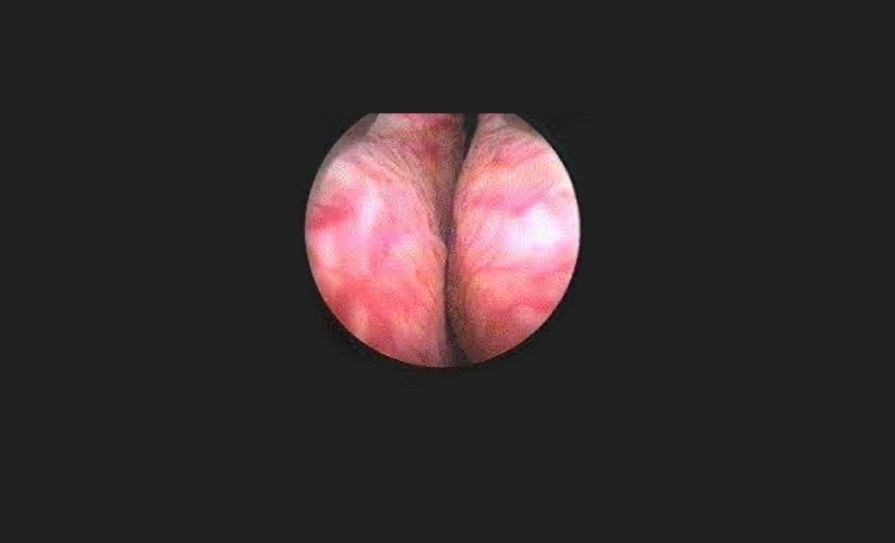
BPH arises predominantly in the transition zone of the prostate. The pathophysiological driver of prostatic enlargement is dihydrotestosterone (DHT), produced from testosterone through the action of 5-alpha reductase. DHT stimulates proliferation of both stromal and epithelial components within the gland, resulting in nodular enlargement. This enlargement contributes to the ‘static’ component of bladder outlet obstruction (see Figure 1).
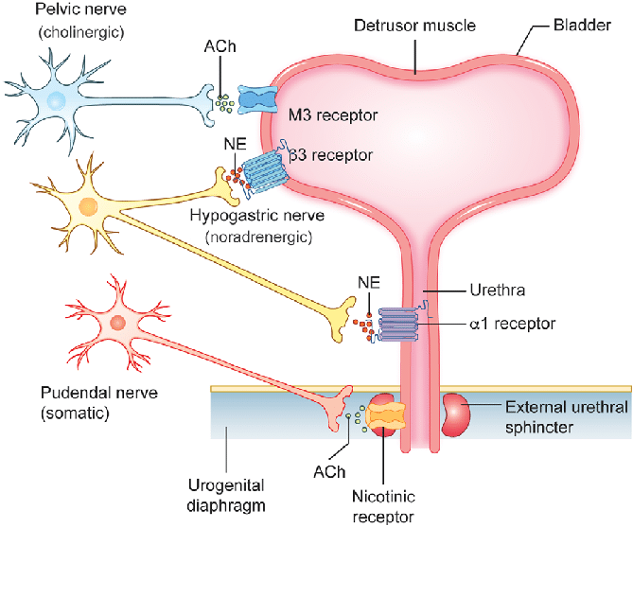
In addition to static enlargement, increased α1-adrenergic smooth muscle tone within the prostate and bladder neck produces a ‘dynamic’ component of obstruction. The relative contribution of static and dynamic factors varies between individuals and underpins the rationale for pharmacological therapy (see Figure 2).
Chronic obstruction induces secondary changes within the bladder. Early in the disease process, detrusor overactivity may develop, producing storage symptoms such as urgency and frequency. With prolonged obstruction, detrusor decompensation may occur, leading to incomplete emptying and elevated post-void residual urine.
LUTS are categorised into storage, voiding, and post-micturition symptoms. Symptom distribution does not reliably predict the presence or severity of bladder outlet obstruction (BOO). This reinforces the importance of structured evaluation.
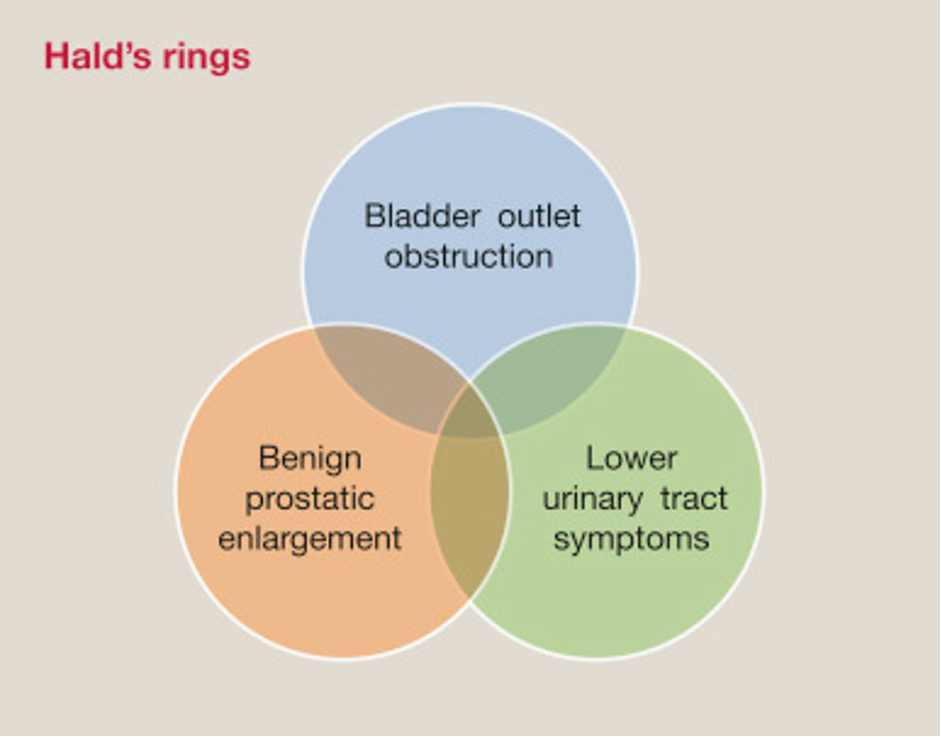
This relationship is often illustrated by Hald’s conceptual ‘rings’, a Venn diagram demonstrating that LUTS, benign prostatic enlargement (BPE), and BOO are overlapping but distinct entities; men may have enlargement without obstruction, obstruction without symptoms, or symptoms in the absence of either (see Figure 3)
Definitions9
Bladder outlet obstruction is the generic term for obstruction during voiding and is characterised by increased detrusor pressure and reduced urine flow rate.
Benign prostatic obstruction is a form of BOO and may be diagnosed when the cause of the outlet obstruction is known to be BPE, due to histologic benign hyperplasia.
Benign prostatic hyperplasia is a term used (and reserved for) the typical histological pattern which defines the disease.
Benign prostatic enlargement is defined as prostatic enlargement due to histologic BPH.
Natural history and disease progression
Although many men experience stable symptoms over time, a clinically significant proportion demonstrate disease progression. Identifying patients at higher risk of progression is central to management decisions.
The Proscar Long-Term Efficacy and Safety Study provided pivotal evidence regarding the natural history of BPH and the impact of medical therapy.3 In this large four-year placebo-controlled study involving over 3,000 men with moderate-to-severe LUTS and enlarged prostates, finasteride significantly reduced the risk of AUR and the need for BPH-related surgery. In addition, finasteride produced sustained improvements in symptom-related bother, activity interference, and worry. Importantly, subgroup analysis demonstrated that the magnitude of benefit was greater in men with baseline PSA ≥1.4ng/mL, a surrogate marker for larger prostate volume.
The Medical Therapy of Prostatic Symptoms trial further clarified progression risk and therapeutic impact.2 In this landmark study, combination therapy with doxazosin and finasteride reduced overall clinical progression by 66 per cent, compared with 39 per cent for doxazosin alone and 34 per cent for finasteride alone. Clinical progression was defined to include symptom deterioration, AUR, incontinence, renal insufficiency, or recurrent urinary tract infections (UTIs). These data established that while alpha-blockers provide symptom relief, 5-alpha reductase inhibitors (5-ARIs) confer disease-modifying benefit, and combination therapy provides superior protection in appropriately selected men.
The CombAT study confirmed the superiority of combination therapy using dutasteride and tamsulosin over tamsulosin monotherapy in reducing the risk of AUR and surgery.10 Together, these trials demonstrate that prostate size and prostate-specific antigen (PSA) are critical determinants of long-term outcome.
Predictors of progression include:2
▶ Age >60 years;
▶ Prostate volume >30mL;
▶ PSA >1.4;
▶ IPSS >7;
▶ Qmax <12mL/sec;
▶ PVR >50mL.
Clinical assessment
A structured approach should be taken to the assessment of male LUTS. Initial evaluation should include a detailed history, quantification of symptoms using the International Prostate Symptom Score (IPSS), digital rectal examination, and urinalysis.1
PSA testing should be offered when results will influence management decisions. Beyond its role in prostate cancer detection, PSA correlates with prostate volume and predicts progression risk.3
Further investigations such as uroflowmetry and measurement of post-void residual volume are useful in selected patients, particularly when considering invasive treatment. Renal imaging is not routinely required, but is indicated in men with suspected upper tract involvement, recurrent infection, haematuria, or renal impairment.
Medical management
Pharmacological treatment of male LUTS targets either the dynamic component of BOO, the static component related to prostatic enlargement, or both. The choice of therapy should be individualised according to symptom severity, prostate size, PSA level, and risk of progression.
Alpha-blockers
Alpha-blockers reduce smooth muscle tone within the prostate and bladder neck, thereby improving urinary flow and reducing voiding symptoms. Their principal benefit lies in symptomatic relief rather than modification of the natural history of prostatic enlargement.
Tamsulosin and alfuzosin are commonly used agents within this class. While both act through α1-adrenergic blockade, their clinical roles differ slightly.
Tamsulosin provides effective improvement in LUTS and is widely used in men with moderate symptoms. However, alpha-blocker monotherapy does not significantly reduce the long-term risk of AUR or the need for surgery when compared with therapies that reduce prostate volume.10 For this reason, in men with enlarged prostates and elevated PSA levels, alpha-blockers alone may not sufficiently address progression risk.
Alfuzosin has demonstrated particular utility in the setting of AUR.6 Initiation of alfuzosin at the time of catheterisation increases the likelihood of successful trial without catheter and reduces the short-term need for surgery following a first episode of spontaneous retention. Continued therapy beyond the acute phase further reduces early surgical intervention. Importantly, alfuzosin has been reported to have good cardiovascular tolerability, including in elderly and hypertensive patients, and was well tolerated in clinical evaluation.
Alpha-blockers, however, do not reduce prostate size and do not modify long-term disease progression in the absence of concomitant volume-reducing therapy.
5-alpha reductase inhibitors
5-ARIs act by inhibiting the conversion of testosterone to DHT, thereby reducing prostate volume over time. Reduction in prostate size typically occurs gradually over months and is associated with decreased risk of AUR and surgical intervention.3
In men with enlarged prostates, long-term treatment reduces progression events and improves symptom-related bother and activity interference. Benefits are most pronounced in men with higher baseline PSA levels (≥1.4ng/mL), which correlate with larger prostate volume and increased risk of progression.2
Unlike alpha-blockers, 5-ARIs provide disease-modifying benefit. However, they are associated with sexual side-effects. Over prolonged treatment, reductions in sexual interest and sexual satisfaction have been observed compared with placebo. Notably, differences in sexual satisfaction were less pronounced in men with higher baseline PSA levels, suggesting that the overall benefit-risk balance may favour treatment in higher-risk individuals.10
Thus, 5-ARIs are particularly appropriate in men with demonstrable prostatic enlargement and elevated PSA who are at risk of progression.
Combination therapy
In men with moderate-to-severe symptoms and enlarged prostates, combination therapy with an alpha-blocker and a 5-ARI addresses both the dynamic and static components of obstruction. This approach provides rapid symptomatic relief through smooth muscle relaxation while simultaneously reducing long-term risk of progression.
Combination therapy has been shown to reduce the likelihood of clinical progression more effectively than either agent alone, particularly in men with larger prostates and elevated PSA levels.2,10
Phosphodiesterase type 5 inhibitors – tadalafil
Tadalafil 5mg once daily is approved for the treatment of LUTS associated with BPH. Symptom improvement occurs without significant change in maximum urinary flow rate, indicating that mechanisms beyond simple mechanical relief of obstruction contribute to its effect.5
A substantial proportion of men experience clinically meaningful improvement in symptoms, with many achieving perceptible benefit within one week of therapy and the majority within four weeks. The relatively rapid onset of effect may enhance treatment adherence and patient satisfaction.4
Acute urinary retention
AUR represents a significant clinical milestone in the natural history of BPE and is associated with increased morbidity and healthcare utilisation. Its incidence increases with age, and in older men the cumulative risk becomes substantial. Immediate management requires bladder decompression by catheterisation. Historically, early surgery was often performed following an episode of retention; however, concerns regarding increased perioperative morbidity and mortality associated with urgent intervention have led to the widespread adoption of trial without catheter (TWOC).11
Pharmacological therapy plays an important role in this setting. Initiation of an alpha-adrenergic antagonist at the time of catheterisation improves the likelihood of successful TWOC and reduces the need for early surgical intervention. In men experiencing a first episode of spontaneous AUR related to BPH, treatment with alfuzosin has been shown to significantly increase TWOC success rates compared with placebo and to reduce short-term progression to surgery when continued after catheter removal.6
Not all patients have equal risk of recurrence. Older age and larger drained volumes at the time of catheterisation are associated with increased risk of TWOC failure, while elevated post-TWOC residual urine volumes are associated with subsequent relapse and need for surgery. These observations underscore the importance of risk stratification following an episode of retention.
While alpha-blockers improve short-term outcomes, they do not eliminate the long-term risk of progression in men with significant prostatic enlargement. Patients with persistent obstruction, recurrent retention, or high-risk features should be considered for definitive surgical management.
Surgical management
Surgical intervention remains an essential component of management for men with refractory symptoms, recurrent AUR, renal impairment attributable to obstruction, recurrent UTIs, or patient preference following failure of medical therapy.
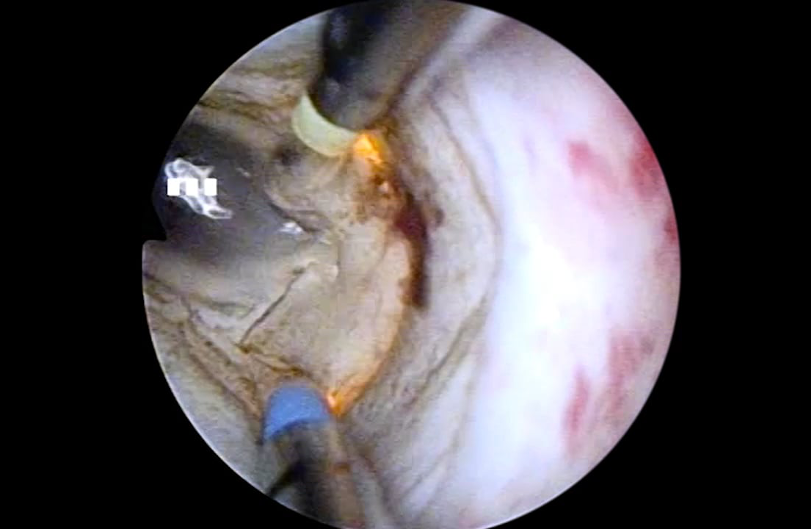
Procedure selection is guided primarily by prostate size, clinical context, and available expertise. Transurethral resection of the prostate (TURP) remains the reference standard for prostates between 30 and 80mL (see Figure 4). It provides durable symptom relief and remains widely performed.12
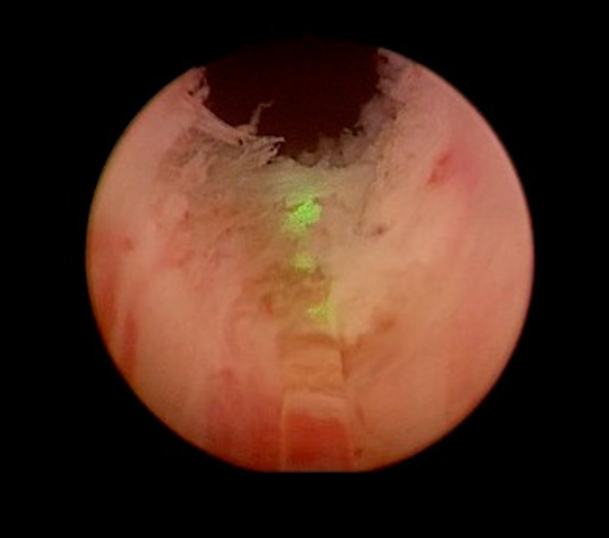
For larger glands, holmium laser enucleation of the prostate (HoLEP) offers effective size-independent treatment and is suitable across a broad range of prostate volumes (see Figure 5). In very large prostates, typically exceeding 80–100mL, simple prostatectomy, whether open or minimally invasive, remains appropriate.13
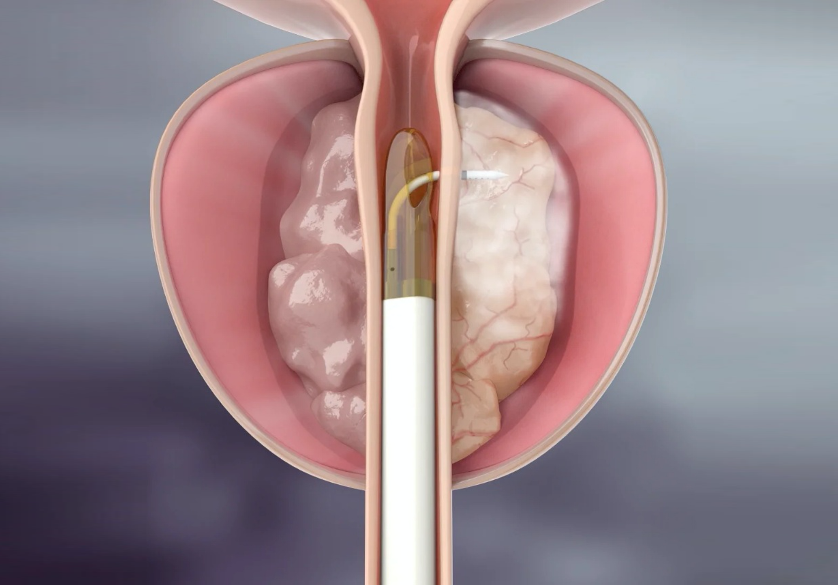
Minimally-invasive surgical therapies have emerged as alternatives for selected patients. These procedures may offer reduced perioperative morbidity and shorter recovery times, but are generally associated with higher retreatment rates when compared with established resection or enucleation techniques (see Figure 6).14,15
Surgical decision-making must therefore balance durability, perioperative risk, prostate size, comorbidity profile, and patient expectations. Importantly, intervention should be viewed not solely as symptom relief, but as prevention of long-term complications in appropriately selected patients.
Conclusion
Male LUTS represent a common and clinically-significant problem in ageing men. Importantly, LUTS should not be regarded as synonymous with BPH. The conceptual framework illustrated by Hald’s rings emphasises that LUTS, BPE, and BOO are overlapping but distinct entities and that accurate evaluation is essential before treatment decisions are made.
Management should be guided by symptom burden, prostate size, PSA level, and risk of progression. Alpha-blockers provide effective symptomatic relief through reduction of smooth muscle tone, while 5-ARIs reduce prostate volume and lower the long-term risk of AUR and surgery, particularly in men with larger glands and elevated PSA.16 Combination therapy offers the most comprehensive medical approach for men at higher risk of progression. Tadalafil provides an additional therapeutic option, with clinically meaningful symptom improvement often occurring early in the course of treatment.
An episode of AUR marks a pivotal point in disease progression and requires both immediate management and careful reassessment of long-term strategy. Surgical intervention remains appropriate for men with refractory symptoms, recurrent retention, or complications of obstruction, with procedure selection determined by prostate size, patient comorbidity, and anticipated durability.
Ultimately, effective care of men with LUTS requires structured assessment, risk stratification, and individualised therapy. A clear understanding of the relationship between symptoms, enlargement, and obstruction allows clinicians to move beyond symptom suppression alone and towards prevention of progression and preservation of quality-of-life.
References
Gratzke C, Bachmann A, Descazeaud A, et al. EAU Guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67(6):1099-109
McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349(25):2387-98
Bruskewitz R, Girman CJ, Fowler J, et al. Effect of finasteride on bother and other health-related quality-of-life aspects associated with benign prostatic hyperplasia. PLESS Study Group. Proscar long-term efficacy and safety study. Urology. 1999;54(4):670-8
Oelke M, Shinghal R, Sontag A, Baygani SK, Donatucci CF. Time to onset of clinically meaningful improvement with tadalafil 5mg once-daily for lower urinary tract symptoms secondary to benign prostatic hyperplasia: Analysis of data pooled from four pivotal, double-blind, placebo controlled studies. J Urol. 2015;193(5):1581-9
Porst H, Kim ED, Casabé AR, et al. Efficacy and safety of tadalafil once daily in the treatment of men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia: Results of an international randomised, double-blind, placebo-controlled trial. Eur Urol. 2011;60(5):1105-13
McNeill SA, Hargreave TB, Roehrborn CG. Alfuzosin 10mg once-daily in the management of acute urinary retention: Results of a double-blind placebo-controlled study. Urology. 2005;65(1):83-9; discussion 9-90
Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132(3):474-9
Garraway WM, Collins GN, Lee RJ. High prevalence of benign prostatic hypertrophy in the community. Lancet. 1991;338(8765):469-71
Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61(1):37-49
Roehrborn CG, Barkin J, Siami P, et al. Clinical outcomes after combined therapy with dutasteride plus tamsulosin or either monotherapy in men with benign prostatic hyperplasia (BPH) by baseline characteristics: 4-year results from the randomised, double-blind combination of avodart and tamsulosin (CombAT) trial. BJU Int. 2011;107(6):946-54
Taube M, Gajraj H. Trial without catheter following acute retention of urine. Br J Urol. 1989;63(2):180-2
Porto JG, Bhatia AM, Bhat A, et al. Transurethral resection of the prostate across continents: A meta-analysis evaluating quality of gold standard in the 21st Century. World J Urol. 2025;43(1):85
Hurle R, Vavassori I, Piccinelli A, Manzetti A, Valenti S, Vismara A. Holmium laser enucleation of the prostate combined with mechanical morcellation in 155 patients with benign prostatic hyperplasia. Urology. 2002;60(3):449-53
McNicholas TA, Woo HH, Chin PT, et al. Minimally invasive prostatic urethral lift: Surgical technique and multinational experience. Eur Urol. 2013;64(2):292-9
McVary KT, Gange SN, Gittelman MC, et al. Minimally invasive prostate convective water vapor energy ablation: A multicenter, randomised, controlled study for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Urol. 2016;195(5):1529-38
Jacobsen SJ, Jacobson DJ, Girman CJ, et al. Treatment for benign prostatic hyperplasia among community dwelling men: The Olmsted County study of urinary symptoms and health status. J Urol. 1999;162(4):1301-6








Leave a Reply
You must be logged in to post a comment.