






A presentation by Dr Cathal O’Connor, a dual-trained consultant dermatologist and consultant paediatrician, at the recent annual Primary Care Dermatology Society of Ireland (PCDSI) meeting in Naas, Co Kildare, provides compelling evidence that challenges long-held assumptions about diet and eczema management
For decades, the relationship between food allergies and atopic dermatitis (AD) (eczema) has been one of the most contentious topics in paediatric dermatology and allergy medicine. Parents desperately seeking answers for their child’s inflamed, itchy skin often turn to baseless dietary modifications, while healthcare providers grapple with nonsensical advice about allergy testing and food elimination diets.
The simple message is: AD is never caused by food allergies. This assertion, supported by research and clinical experience, has profound implications for how we approach the management of childhood eczema.
AD: A multifactorial disease
AD affects up to 30 per cent of Irish children, with approximately 3 per cent experiencing severe disease (O’Connor C. Pediatr Dermatol. 2022). Rather than being a simple allergic reaction to foods, AD represents a complex interplay of three primary pathophysiological mechanisms (Figure 1):
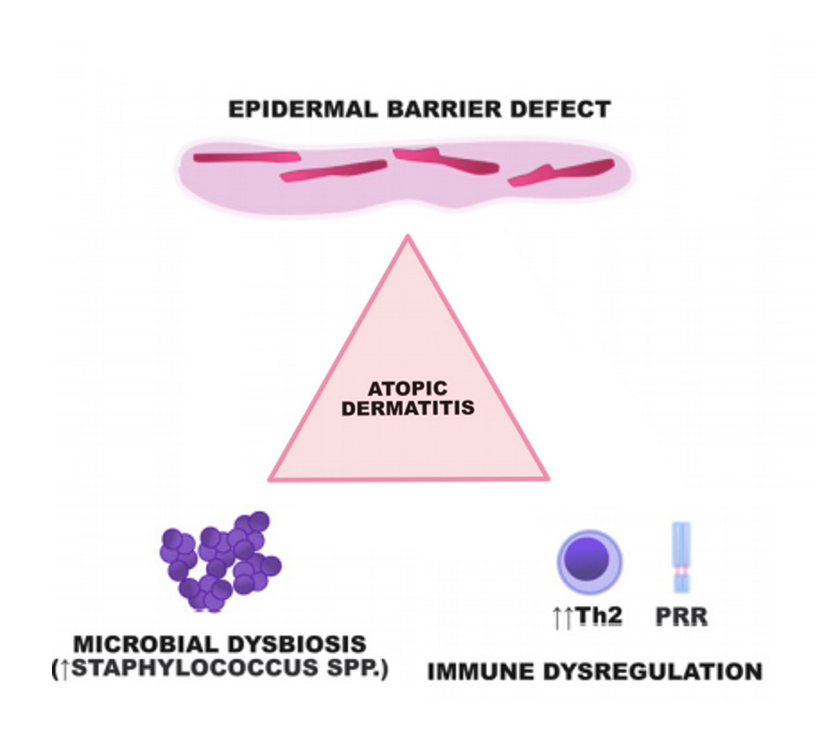
1. Epidermal barrier dysfunction: The skin barrier in AD patients is fundamentally compromised, often due to genetic variants such as filaggrin mutations. These defects result in increased transepidermal water loss and enhanced penetration of allergens, irritants, and pathogens. The barrier dysfunction is primary, not secondary to food exposure.
2. Immune dysregulation AD is characterised by a predominantly Th2-mediated immune response, with elevated levels of cytokines including IL-4, IL-13, IL-31, and increased IgE production. This immune skewing creates a state of chronic inflammation that is self-perpetuating and independent of dietary triggers.
3. Microbial dysbiosis patients with AD demonstrate altered skin microbiomes, with increased colonisation by Staphylococcus aureus (S aureus) and decreased microbial diversity. This dysbiosis contributes to inflammation and barrier dysfunction through the production of bacterial toxins and proteases.
The food allergy development pathway
Contrary to popular belief, food allergies do not cause AD. Instead, the relationship is inverted: AD predisposes to food allergy development through cutaneous sensitisation. The ‘dual allergen exposure hypothesis’ explains that:
- Cutaneous exposure through defective skin barrier leads to Th2-mediated sensitisation and allergy development.
- Oral exposure during the critical window of immune development (first months of life) promotes tolerance through regulatory T-cell responses.
This explains why filaggrin mutations, which cause severe barrier dysfunction, increase the odds ratio for peanut allergy by 5.3-fold while only increasing AD risk by 3.1-fold.
Clinical differentiation: Eczema vs food allergic reactions
One of the most critical skills for parents and healthcare providers is distinguishing between AD flares and genuine food allergic reactions. True food allergic reactions are never subtle.
AD characteristics:
- No temporal relationship to food ingestion.
- Chronic or subacute course (not hyperacute).
- Gradual onset and resolution.
- Eczematous morphology (not urticarial).
- Absence of systemic symptoms.
Food allergic reaction features:
- Hyperacute onset within minutes of allergen exposure.
- Clear temporal relationship to allergen exposure.
- Urticarial/erythematous appearance (not eczematous).
- Potential angioedema (lips, eyes, face).
- Systemic symptoms may include respiratory distress, cardiovascular changes, or gastrointestinal symptoms.
- Parents typically recognise these as allergic reactions without prompting.
As I noted at the PCDSI conference, if parents ask whether their children need food allergy testing, then they probably do not. Genuine food allergic reactions are dramatic events that families readily identify as such.
The allergy testing controversy
The problem with specific IgE testing
Current allergy testing practices present significant challenges in the context of AD:
- 70 per cent of AD patients are sensitised to one or more foods on SpIgE testing.
- Less than 10 per cent are genuinely allergic to those foods.
- This creates a massive potential for misdiagnosis and inappropriate dietary restrictions.
The term ‘RAST testing’ has been considered obsolete since the year 2005, having been replaced by specific IgE (SpIgE) testing using newer generation methods. However, even modern SpIgE testing has limitations:
- Results are not binary (positive/negative), but exist on a continuum.
- Predictive values vary significantly by allergen and patient age.
- Component-resolved diagnostics and skin prick testing may offer better specificity.
Total IgE: Generally a worthless test for eczema
During my presentation at the PCDSI conference I was particularly critical of total IgE measurements – I only order them when suspecting the ultra-rare hyper-IgE syndrome or considering dupilumab therapy for alopecia areata. Total IgE levels do not aid in the diagnosis or management of AD and should be abandoned in routine practice.
The dangers of food elimination
Iatrogenic food allergy development
Perhaps the most concerning finding is that food elimination can actually cause food allergies. Research demonstrates that:
- 20 per cent of children with AD develop food allergies when previously tolerated foods are removed from their diet.
- 30 per cent of these newly-developed allergies present as anaphylaxis.
- Fatal allergic reactions have been reported as consequences of unnecessary food elimination.
This phenomenon occurs because continuous oral exposure is necessary to maintain immune tolerance in early childhood. When foods are withdrawn in infancy, the oral tolerance pathway is disrupted, potentially leading to sensitisation upon re-exposure.
The breastfeeding misconception
A particular area of concern is the advice given to breastfeeding mothers to eliminate dairy from their diets to ‘treat’ their baby’s eczema. Compelling evidence against this practice includes that:
- Human breast milk contains one-millionth the β-lactoglobulin concentration of cow’s milk.
- This level is too low to trigger reactions even in most infants with confirmed cow’s milk protein allergy.
- Maternal dairy elimination can lead to maternal nutritional deficiency and psychological distress.
- It provides no benefit for infant eczema and any observed response is a placebo response.
Early food introduction: The prevention paradigm
The LEAP trial revolution
The Learning Early About Peanut Allergy (LEAP) trial fundamentally changed our understanding of food allergy prevention. In children with severe eczema and/or egg allergy:
- Early peanut introduction (four to 11 months) reduced peanut allergy by 81 per cent.
- Peanut allergy prevalence was 17.3 per cent in the avoidance group versus 0.3 per cent in the consumption group.
- Earlier introduction was more effective than later introduction.
Current recommendations
Based on this evidence, I recommend:
- Introduce smooth peanut butter at 12 weeks of age;
- Continue regular consumption to maintain tolerance;
- Do not delay introduction of other allergenic foods;
- Use structured introduction protocols (milk ladders, egg ladders) when reintroducing previously inappropriately avoided foods.
Evidence-based treatment of AD
I advocate for a targeted approach addressing the three pathophysiological mechanisms:
1. Topical anti-inflammatory therapy
- Topical corticosteroids are the foundation of treatment of eczema/dermatitis.
- Ointment formulations are preferred over creams.
- Liberal application (not ‘sparingly’) with sufficient potency, volume, frequency, and duration.
- Induction therapy (once daily) for at least two weeks.
- Weaning periods (Tuesday/Thursday/Saturday/Sunday) for two weeks.
- Maintenance therapy (Saturday/Sunday weekend therapy ) to prevent flares for four to six months of clear skin to ensure immune reconstitution.
- Topical steroid concerns are unfounded – topical steroids are safe and effective for mild-to-moderate eczema.
2. Barrier repair
- Emollients treat xerosis (dry skin) rather than active inflammation – they are not the mainstay of therapy for eczema/dermatitis;
- Applied downwards to prevent folliculitis;
- Pump dispensers preferred to prevent contamination;
- Wet wraps are discouraged due to burden, infection risk, and limited efficacy.
3. Antimicrobial therapy
- Antiseptic baths (sodium hypochlorite/Milton solution) twice weekly;
- Reduces S aureus colonisation without promoting antibiotic resistance;
- Adjunctive therapy, not monotherapy.
Debunking common myths
Three persistent ‘nonsenses’ in eczema management:
1. Detergents cause eczema
Modern washing machines leave negligible detergent residues. Unless patients wash laundry by hand or apply detergent directly to skin, clothing detergents do not cause eczema. Advising non-biological detergents is unnecessary and potentially anxiety-provoking.
2. Topical steroids are unsafe
Topical corticosteroids represent elegant, targeted therapy that avoids systemic exposure. Twice-weekly maintenance therapy does not cause skin thinning. The major issue is nocebo effect and steroid concerns perpetuated by social media misinformation.
3. Food allergies cause eczema
As extensively discussed, this fundamental misconception leads to inappropriate testing, unnecessary dietary restrictions, and potential harm through induced food allergies.
The social media misinformation crisis
Social media misinformation is causing a significant negative impact on eczema management. Some posters on platforms like TikTok and Instagram promote dangerous advice including:
- Topical steroid concerns;
- Extreme dietary restrictions;
- Unproven ‘natural’ treatments;
- Fear-mongering about established therapies.
Healthcare providers must actively counter this misinformation with evidence-based education and clear communication.
Clinical implications and future directions
For primary care providers:
- Avoid routine allergy testing in AD patients;
- Focus on proper topical therapy education;
- Encourage early food introduction in all infants;
- Refer appropriately for moderate-to-severe AD requiring systemic therapy.
For specialists:
- Patient education remains crucial for treatment adherence.
- Biologics and newer systemic therapies offer hope for severe cases.
Research priorities
- Improved biomarkers for distinguishing sensitisation from clinically-relevant allergy.
- Better understanding of the skin microbiome’s role in disease pathogenesis.
- Development of barrier repair therapies targeting specific genetic defects.
Conclusion
The directionality of the relationship between food allergies and AD is very different to what many healthcare professionals were taught in training. Rather than foods causing eczema, AD creates the conditions for food allergy development through barrier dysfunction and cutaneous sensitisation. This paradigm shift has profound implications:
1. Routine allergy testing in AD is unnecessary and potentially harmful.
2. Early food introduction prevents rather than causes allergies.
3. Dietary restrictions may cause more harm than benefit.
4. Topical anti-inflammatory therapy should be the treatment focus.
This approach provides a roadmap for evidence-based management that prioritises effective treatments while avoiding interventions that may inadvertently worsen outcomes.
The chicken (genetic predisposition and barrier dysfunction) comes before the egg (food sensitisation), and understanding this sequence is crucial for optimal patient care.
The takeaway for healthcare providers is clear: Focus on treating the underlying disease mechanisms of AD rather than chasing dietary ghosts.
We must resist the pressure to order ‘just in case’ allergy tests and instead provide families with the evidence-based education they need to make informed decisions about their child’s care.
Utilising this evidence-based knowledge, we can break the cycle of misinformation and provide truly effective management for children suffering from AD.
*The Irish Skin Foundation provides information and support resources for both healthcare professionals and patients. See https://irishskin.ie/eczema/
References on request









Leave a Reply
You must be logged in to post a comment.