Reference: June 2026 | Issue 6 | Vol 12 | Page 62
Trigeminal neuralgia (TN) is a chronic neuropathic disorder which affects the distribution of the trigeminal nerve. Women are more commonly affected than men and the incidence increases with age.
The diagnosis is clinical and is characterised by three main clinical criteria:1
1. The pain is characterised by paroxysms of sudden intense electric shock-like pain which typically last just a few seconds (less than one second to two minutes).
2. The pain is unilateral and is restricted to the territory of one or more divisions of the trigeminal nerve. Bilateral trigeminal neuralgia is rare and should raise concern regarding multiple sclerosis (MS) as the cause of TN or alternatively non-TN facial pain.
3. There are clear triggers such as touching the face, chewing, brushing teeth, shaving, and cold wind.
The clinical examination is normal. There is no trigeminal sensory loss.
History-taking is of utmost importance to establish the diagnosis and to differentiate TN from other types of facial pain such as dental causes, sinusitis, temporomandibular joint disorders, other cranial neuralgias (eg, postherpetic neuralgia), trigeminal autonomic cephalgias (cluster headaches), persistent idiopathic facial pain (previously called atypical facial pain), and giant cell arteritis. Establishing the correct diagnosis is essential, since diagnostic error can expose patients to ineffective and potentially invasive interventions.
Classification
Trigeminal neuralgia can be categorised into one of the following:1
1. Classical TN: The majority of patients with TN fall into this category. These patients have no facial sensory loss. In classical TN, the cause is neurovascular compression (also called neurovascular conflict) of the trigeminal nerve. In other words, a blood vessel (usually an artery) is touching or in some cases even compressing the trigeminal nerve just as it enters the brainstem. The most common vessel responsible is the superior cerebellar artery (SCA). However, other arteries and, in some cases veins, may be responsible. The mechanism by which neurovascular compression is thought to cause TN is related to damage to the myelin sheath of the trigeminal nerve just as it enters the brainstem.
This area, called the nerve root entry zone (REZ), is the most vulnerable part of the nerve because it is where peripheral myelin (Schwann cells) changes to central myelin (oligodendrocytes). Vascular compression of this area leads to focal demyelination. When myelin is lost, neighbouring nerve fibres become ‘leaky’, allowing electrical signals to jump from one nerve fibre to another. This short-circuiting between adjacent demyelinated nerve fibres is called ephaptic transmission. For example, light touch fibres (normally non-painful fibres) may activate neighbouring pain fibres, as a result of which, normally non-painful stimuli – such as touching or washing the face – can trigger sudden severe electric shock-like pain. The injured nerve subsequently becomes hyperexcitable, such that minimal sensory stimuli can produce massive pain discharges.
2. Secondary TN: This accounts for approximately 15 per cent of cases. The most common causes for secondary TN are:
A. Multiple sclerosis (MS): Demyelinating plaques in patients with MS can damage the trigeminal pathways within the brainstem resulting in abnormal electrical conduction, similar to the mechanism describe above for vascular compression. Approximately 3-4 per cent of MS patients have TN, while 2-14 per cent of patients with TN are found to have MS.2,3 Bilateral TN should raise suspicion for MS being the cause.
B. Tumours: Benign tumours, such as meningiomas and schwannomas, and cysts, such as epidermoid cysts, can compress the trigeminal nerve and lead to trigeminal pain.
Although not all patients with secondary TN have facial numbness, the presence of sensory loss is a red flag and should prompt an urgent MRI scan to rule out MS, tumours, and cysts compressing the trigeminal nerve. Other red flag symptoms and signs are corneal numbness, bilateral symptoms, age less than 40 years at the time of symptom onset, and the presence of other cranial nerve deficits.
3. Idiopathic TN: In these patients no neurovascular compression is identified and no secondary pathology (such as MS or tumour) is present. MRI is completely normal in these cases and the cause of TN is unknown.
TN with continuous pain
As outlined above, paroxysmal pain with pain-free intervals between the attacks is the hallmark of typical trigeminal neuralgia. However, 24-49 per cent of patients report a background continuous pain between the paroxysmal attacks.2,3 This background pain is described by patients as burning, throbbing, or aching, which is in the same distribution as the paroxysmal pain. This was previously called atypical TN but is now termed TN with concomitant continuous pain.4 The pathophysiological mechanism for this pain is poorly understood but it may be associated with trigeminal nerve root atrophy.5 TN with concomitant continuous pain is generally considered more difficult to treat and, in particular, the continuous background component of the pain may be associated with poorer treatment response than the paroxysmal pain.5
Investigations
Although the diagnosis of TN is purely clinical, radiological imaging helps to identify potential causes and guide treatment. It is not possible to differentiate the various subtypes of TN outlined above clinically. Therefore, all patients with TN should undergo MRI. It is important to note that requesting a standard MRI brain alone is insufficient for optimal assessment of TN. The MRI request should include the following:
1. MRI brain with contrast to rule out causes of secondary TN (ie, MS or tumour compressing the trigeminal nerve).
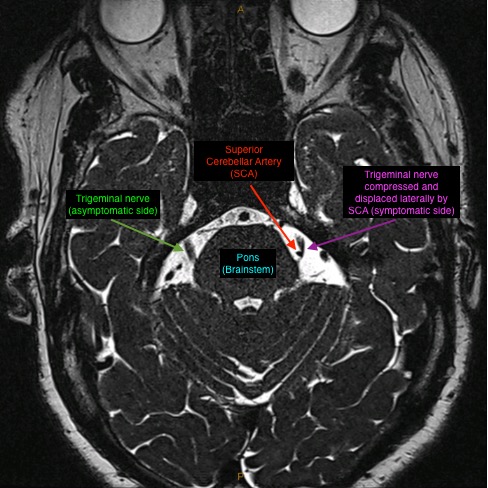
2. Dedicated high-resolution MRI of the trigeminal nerves to identify neurovascular compression. This includes high-resolution, heavily T2-weighted MRI sequences (such as CISS or FIESTA), with fine cuts through the region of the trigeminal nerves. These MRI sequences allow excellent visualisation of the cranial nerves and their relationships to blood vessels (Figure 1). It is worth noting that the blood vessels responsible for neurovascular compression are usually anatomically normal arteries rather than pathological vascular lesions. It is also important to recognise that neurovascular conflict may be observed in asymptomatic individuals and, in isolation, is of no clinical significance. However, in patients with clinically diagnosed TN, the presence of neurovascular conflict on MRI can help guide selection of appropriate surgical interventions. The MRI is best reviewed by neurosurgeons experienced in performing microvascular decompression (MVD) because interpretation of TN imaging can be highly nuanced, and clinically relevant neurovascular compression may be overlooked on routine radiology reporting. As such, referral to an experienced MVD surgeon should be made even when MRI findings are reported as normal.
3. Magnetic resonance angiography (MRA) brain is also useful in assessing the vascular anatomy and may be useful in identifying vascular malformations that can rarely present with TN.
Neurosurgical interventions
Once a clinical diagnosis of TN is made, medical therapy should be started and an MRI should be requested as outlined above. First-line therapy includes carbamazepine or oxcarbazepine. A dramatic response to these medications supports the diagnosis of TN. Although these medications are initially effective in most patients, some individuals may experience reduced efficacy, dose-limiting adverse effects, or treatment intolerance over time. Second-line therapy includes lamotrigine, baclofen, gabapentin, and pregabalin.6
In general, opioids are not effective in acute exacerbations of TN and their use is not supported by evidence.7 Severe acute exacerbations can result in inability to eat or drink and, therefore, can lead to dehydration, weight loss, and, in some cases, suicidal ideation. In such cases, urgent and occasionally emergency in-hospital treatment is necessary for titration of anti-epileptic drugs and rehydration. Acute pain relief is crucial for affording a window of opportunity to adjust oral medication and to control pain in consideration of a possible neurosurgical intervention.7
Patients with medically refractory TN or those unable to tolerate medical therapy should be referred for specialist neurosurgical evaluation.
Neurosurgical interventions for TN include the following:
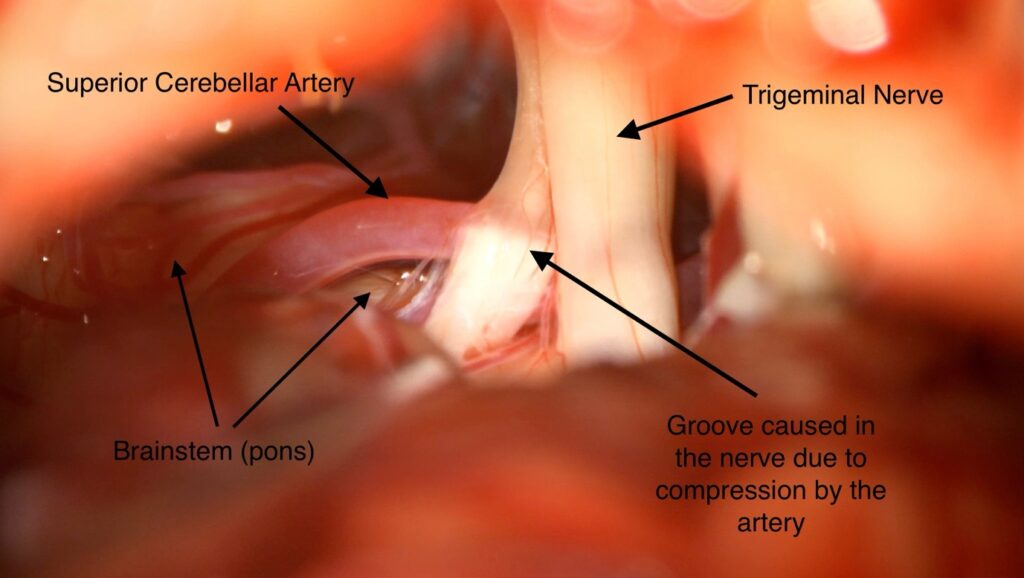
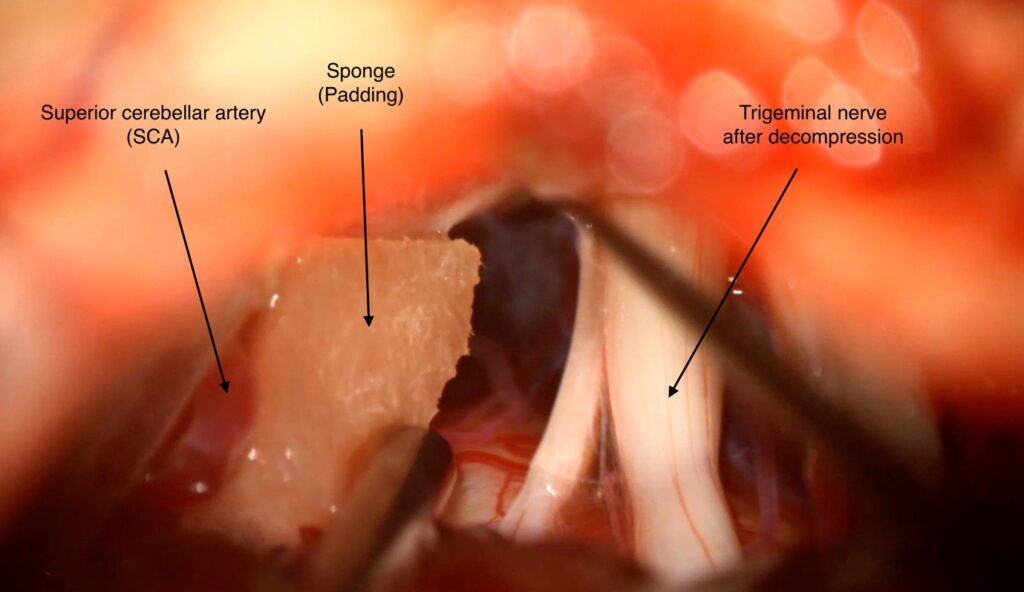
1. Microvascular decompression: This is a neurosurgical procedure performed under general anaesthesia by neurosurgeons with specific interest in TN. It is performed through a mini-craniotomy just behind the ear/mastoid process. Using the neurosurgical operating microscope, the trigeminal nerve REZ is exposed and the blood vessel compressing it is mobilised away from the nerve. A small piece of padding material is placed between the artery and the nerve to keep them separated (Figure 2 and Figure 3).
This procedure is appropriate in patients with classical type TN where an MRI has confirmed neurovascular compression. Among non-pharmacologic interventions for TN, MVD has the highest success rate in terms of long-term pain control. At one to two years postoperatively, 68-88 per cent of patients are pain-free with no need for medication, with this percentage being 61-88 per cent at four to five years.7
Although MVD carries potentially serious risks, including stroke and mortality, these complications are rare in experienced centres. Mortality and stroke have been reported to occur in 0.3 per cent and 0.6 per cent, respectively.7 The risk of ipsilateral hearing loss due to stretching of the vestibulocochlear nerve is minimised by the use of intraoperative neurophysiological brainstem auditory evoked potential monitoring.
MVD is unique among surgical treatments for TN in that it is a non-ablative procedure that treats the underlying neurovascular compression without intentionally damaging the trigeminal nerve. Therefore it is associated with a very low rate of postoperative facial numbness. The procedure can be performed safely in carefully selected elderly patients with excellent results and therefore age alone is not a contraindication to surgery.8 Unfortunately, the outcomes following MVD in MS-related TN are generally less favourable than those observed in classical TN.9
2. Stereotactic radiosurgery (SRS): This is highly focused radiation treatment that is delivered using stereotactic techniques. The radiation is delivered very accurately to a small segment of the cisternal segment of the trigeminal nerve (just anterior to the brainstem). SRS is an ablative procedure and results in selective injury to the nerve fibres involved in pain transmission, leading to reduced ectopic firing. It is a minimally invasive treatment which is performed as a day case procedure without the requirement for any form of anaesthesia. Pain relief is usually delayed (days to weeks, sometimes months).
The treatment can be delivered using a variety of equipment such as the Gamma knife, Cyberknife, Zap-X, and linear accelerator (LINAC)-based systems. The success rate is lower than that of MVD and recurrence rates are higher, with 24-71 per cent of patients pain-free, with no need for medication at one to two years, and 33-56 per cent at four to five years.7 Facial numbness occurs in approximately 15 per cent of patients following SRS, although severe or bothersome numbness is uncommon.7,10 SRS can be used in patients with classical TN as well as those with idiopathic TN. Given its minimally invasive nature, SRS is frequently considered in patients with MS-related TN, particularly as these patients do not respond as well to MVD as those with classical TN.
3. Percutaneous ablative procedures: These procedures are performed by inserting a cannula through the cheek and advancing it through the foramen ovale to access the trigeminal ganglion under image guidance, usually fluoroscopy. The procedure is performed as a day case procedure under sedation with local anaesthesia or under light general anaesthesia. The aim is to selectively injure pain-transmitting fibres within the trigeminal nerve.
The three main percutaneous ablative techniques are radiofrequency thermocoagulation (RFTC), balloon compression (BC), and glycerol rhizolysis (GR). The success rate is lower than with MVD, with long-term pain-free rates of 26-82 per cent for RFTC, 55-80 per cent for BC and 19-58 per cent for GR.7 There is also a higher rate of facial numbness compared to other techniques (19 per cent for RFTC and15 per cent for BC).7 However, percutaneous procedures are particularly useful in acute pain crises, as they are minimally invasive and can frequently be delivered with minimal delay.
Conclusion
In summary, all patients with TN should undergo appropriate MRI imaging of the brain and trigeminal nerves. Patients whose pain is refractory to, or who are unable to tolerate, medical therapy should be referred to a neurosurgeon with expertise in TN, even when MRI findings are reported as normal. Microvascular decompression, stereotactic radiosurgery, and percutaneous ablative procedures can provide significant improvement in pain control for appropriately selected patients with TN.
References
- Cruccu G, Di Stefano G, Truini A. Trigeminal neuralgia. N Engl J Med. 2020 Aug 20;383(8):754-762. doi: 10.1056/NEJMra1914484.
- Di Stefano G, Maarbjerg S, Nurmikko T, . Triggering trigeminal neuralgia. Cephalalgia. 2018 May;38(6):1049-1056. doi: 10.1177/0333102417721677.
- Maarbjerg S, Gozalov A, Olesen J, Bendtsen L. Concomitant persistent pain in classical trigeminal neuralgia – evidence for different subtypes. Headache. 2014 Jul-Aug;54(7):1173-83. doi: 10.1111/head.12384.
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1-211. doi: 10.1177/0333102417738202.
- Di Stefano G, De Stefano G, Leone C, et al. Concomitant continuous pain in patients with trigeminal neuralgia is associated with trigeminal nerve root atrophy. Cephalalgia. 2020 Nov;40(13):1502-1510. doi: 10.1177/0333102420949206.
- Royal College of Surgeons of England. Guidelines for the management of trigeminal neuralgia 2021.
- Bendtsen L, Zakrzewska JM, Abbott J, et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019 Jun;26(6):831-849. doi: 10.1111/ene.13950.
- Javadpour M, Eldridge PR, Varma TR, et al. Microvascular decompression for trigeminal neuralgia in patients over 70 years of age. Neurology. 2003 Feb 11;60(3):520. doi: 10.1212/wnl.60.3.520.
- Eldridge PR, Sinha AK, Javadpour M, et al. Microvascular decompression for trigeminal neuralgia in patients with multiple sclerosis. Stereotact Funct Neurosurg. 2003;81(1-4):57-64. doi: 10.1159/000075105.
- Tuleasca C, Régis J, Sahgal A, et al. Stereotactic radiosurgery for trigeminal neuralgia: A systematic review. J Neurosurg. 2019 Mar 1;130(3):733-757. doi: 10.3171/2017.9.JNS17545.