NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
IKA welcomes development of prototype for Irish Kidney Disease Data System
By
Reporter
- 10th Mar 2026
iStock.com/Natali_Mis
The Irish Kidney Association (IKA) has welcomed the announcement of the initial prototype for the Irish Kidney Disease Data System (IKDDS).
IKA CEO Ms Carol Moore said the IKDDS is “a proactive initiative within the health service to effectively capture key information and improve the identification and management of kidney disease, which should lead to better outcomes for patients”.
In advance of World Kidney Day on 12 March, the IKA is highlighting the high prevalence of chronic kidney disease (CKD) and encouraging the public to learn about the risk factors and seek early testing.
CKD affects approximately one-in-ten adults in Ireland, rising to one-in-seven among those over 50. On its current trajectory, kidney disease is projected to become the fifth leading cause of death globally by 2040. Despite its prevalence, CKD is often described as a ‘silent condition,’ with an estimated 98 per cent of people in the early stages unaware they have it.
The risk of having CKD increases if a person has diabetes, heart disease, or high blood pressure, a family history of kidney disease, are over 50, or use certain over-the-counter medications long term. A blood and urine test undertaken by a GP can help assess kidney health. More information is available at www.ika.ie/kidneyhealth.
The number of people in Ireland requiring dialysis has more than tripled in the past 25 years. At the end of 2025, some 2,647 people – including 30 children – were receiving dialysis treatment, with 351 people receiving home dialysis and 2,296 receiving in-centre haemodialysis. In 2024, there were 559 patients on the kidney transplant waiting list.
Ms Moore said: “Behind every statistic is a person and a family whose lives are permanently changed by kidney failure. There is a profound human cost to patients and their families – including the physical and mental health toll of treatment, emotional strain, and significant disruption to daily life. Dialysis treatment is already costing the HSE more than €300 million per year, showing the urgent importance of prevention and early intervention.
“Dialysis treatment is life-sustaining but demanding, and transplantation, while transformative, requires ongoing life-long specialist care. The burden on patients, families and the health service is significant. Early detection and prevention are the most effective way to reduce avoidable suffering and long-term healthcare costs. New treatments can often help ensure dialysis is not needed. Our awareness campaign highlights the importance of early detection and treatment. We ask people at risk this World Kidney Day to take charge of their kidney health and get tested.”
She added: “We welcome the development of the IKDDS as an essential resource for improving services for patients and we call for the prototype to be guaranteed multi-annual funding to ensure it can be expanded beyond a prototype.”
Prof Austin Stack, Professor of Medicine and Consultant Nephrologist at University of Limerick and University Hospital Limerick and one of the leaders in the development of the IKDDS prototype, said: “Early detection of chronic kidney disease is crucial to preventing progression and improving outcomes through timely intervention and effective management. The development of the Irish Kidney Disease Data System, under the governance of the Health Service Executive, brings Ireland to an important juncture and once fully implemented, will mark a significant step forward in strengthening how we understand and manage kidney disease at a national level, and aligning our services with international standards.
“High-quality, reliable data are fundamental to improving outcomes, enabling earlier intervention, and ensuring that health services are designed around population needs rather than reacting at the point of crisis. By enhancing how kidney health is monitored and measured, Ireland has an opportunity to shift from reactive treatment of kidney failure to proactive protection of kidney health.”
Dr Colm Henry, Chief Clinical Officer of the HSE, added: “I welcome the work of the Irish Kidney Association in raising awareness about kidney health while marking World Kidney Day. Chronic kidney disease is closely linked with other major health priorities, including diabetes, hypertension, and cardiovascular disease, and requires a coordinated, system-wide response in the health system including primary care. The establishment of the prototype Irish Kidney Disease Data System reflects the HSE’s commitment to strengthening chronic disease surveillance and evidence-informed service planning.”
The IKA’s awareness campaign has the endorsement of the HSE’s National Renal Office and the Irish Nephrology Society, along with the support of the Irish Pharmacy Union and various pharmacy chains across Ireland. The HSE is also amplifying the campaign’s messaging.
Management of diabetic nephropathy in patients with type 2 diabetes
By
Dr Mark Emanuel Debono and Dr Francesca Briffa
- 01st Nov 2024
Diabetes mellitus is the leading cause of chronic kidney disease (CKD) and end stage renal disease (ESRD) globally. Around 20-40 per cent of diabetics develop diabetic kidney disease (DKD). This is a clinical syndrome characterised by progressive decline in estimated glomerular filtration rate (eGFR); elevated arterial blood pressure (BP); and persistent albuminuria (>300mg/d) on at least two visits, three to six months apart.
Structural changes include thickening of the glomerular basement membrane (GBM), mesangial expansion, podocyte injury, and glomerulosclerosis. Extraglomerular lesions are also involved in the progression of the disease, including tubular atrophy, interstitial inflammation, and tubulointerstitial fibrosis.
Functional changes encompass a paradoxically high eGFR in the early stages of the disease, termed glomerular hyperfiltration, caused by afferent arteriolar vasodilation and/or by efferent arteriolar vasoconstriction owing to activation of the renin-angiotensin-aldosterone system (RAS), leading to glomerular hypertension. Later, proteinuria, systemic hypertension, and loss of renal function develop.
Risk factors for DN
Non-modifiable risk factors for DN include increasing age, family history, and genetic factors, with genes such as ACE, APOC1, GREM1, UNC13B, ALR2, APOE associated with the disease. DN is also more common in black people, Mexican Americans, Pima Indians, and Hispanics compared to Caucasians, and female gender is associated with a reduced risk of progression from moderate albuminuria to severe albuminuria or ESRD.
Modifiable risk factors include smoking; longer durations of diabetes; obesity; hypertension; poor glycaemic control; and dyslipidaemia (abnormal lipoprotein metabolism is accelerated in DN that causes further renal injury, leading to ESRD).
Clinical features
The most common clinical abnormalities of DKD are persistently elevated urine albumin excretion and/or persistently declining eGFR. These manifestations tend to be asymptomatic, being detected through routine periodic testing. For this reason, type 2 diabetics should undergo testing at the time of diagnosis, and yearly thereafter.
On some occasions, patients can complain of fatigue, foamy urine, and pedal oedema due to hypoalbuminaemia and nephrotic syndrome. They may also have associated peripheral vascular disease, hypertension, cardiovascular disease (CVD), and diabetic retinopathy.
Investigations
1. Routine blood tests: Renal profile, full blood count, electrolytes. 2. Urine albumin excretion: Albuminuria can be established if two to three urine collections obtained over three to six months show elevated levels of albumin. 3. Urine culture to exclude infection and microscopy to examine for red cell casts in glomerulonephritis. 4. Anti-DNA antibodies, antinuclear antibody, extractable nuclear antigen, complement levels, anti-neutrophil cytoplasmic antibodies, antistreptolysin O titre, rheumatoid factor, and anti-glomerular membrane antibody to check for autoimmune disease. 5. Serum protein electrophoresis, immunoglobulins, urine protein electrophoresis for multiple myeloma. 6. Renal ultrasound. 7. Renal biopsy: The gold standard, but rarely used.
CLASS
DESCRIPTION AND CRITERIA
I
GBM thickening on electron microscopy: GBM >395nm (female), GBM >430nm (male)
IIa
Mild mesangial expansion
IIb
Severe mesangial expansion. A lesion is considered severe if areas of expansion larger than the mean area of a capillary lumen are present in >25 per cent of total mesangium
III
At least one Kimmelstiel-Wilson lesion (nodular intercapillary glomerulosclerosis) and there is <50 per cent global glomerulosclerosis
IV
Advanced diabetic glomerulosclerosis. There is >50 per cent global glomerulosclerosis, attributable to diabetic nephropathy
TABLE 1: Tervaert classification
Classification
Tervaert classification provides a systematic approach with regards to the classification of the pathology of DN and gives a guide with regards to the prognosis of the disease. An important limitation of this classification scheme is that not all pathologic lesions are included, such as presence of mesangiolysis, capillary aneurysms, exudative lesions, and focal/segmental sclerosis.
Treatment
There is no definitive cure for DKD, with management focused on lifestyle interventions and optimal glucose and BP control.
Lifestyle interventions
Input from a dietitian is often indicated for this patient cohort. Patients with diabetes and CKD should generally consume a diet rich in vegetables, fruits, fibre, legumes, plant-based proteins, unsaturated fats, and nuts whilst avoiding processed meats, sweetened beverages, and refined carbohydrates. In advanced CKD, however, potassium in particular, needs to be restricted.
Nutrition therapy can reduce levels of Hba1c to similar or even better ones to those achieved with glucose-lowering medications. However, too much protein can lead to reduced carbohydrate intake with consequent weight loss, and such diets can cause harm to kidney function due to increased urinary excretion of amino acids, which can elevate acid load and precipitate metabolic acidosis, especially in patients with poor kidney function.
On the other hand, in very limited studies, protein restriction has been associated with a slower decline in eGFR in non-diabetics with CKD. Most type 2 diabetic CKD patients would have already been counselled on the appropriate carbohydrate and fat intake, and with protein restriction, malnutrition, reduced quality of life, and hypoglycaemia can develop.
In view of the lack of clinical trials, guidance for such patients is based on the World Health Organisation recommendations for protein intake of 0.8g/kg/day being associated with good outcomes. Patients on dialysis are recommended to consume 1.0-to-1.2g/kg/day as dialysis causes a catabolic response, with loss of amino acids. In addition, the presence of uraemia promotes decreased appetite, increased catabolism, and reduced muscle mass.
Low sodium intake is associated with lower BP and improved cardiovascular (CV) outcomes in the general population. Patients with CKD tend to be salt-sensitive and unable to regulate BP and extracellular fluid volume status when consuming high salt diets. Low salt intake is associated with improvement in volume status and reduced proteinuria, while high sodium intake is associated with increased mortality and morbidity. The guidelines advise that sodium intake should be restricted to <2g/day or <90mmol of sodium/day (<5g of sodium chloride/day).
Engaging in physical activity offers cardiometabolic, kidney, and cognitive benefits. Weight loss may reduce urinary albumin excretion and improve BP. Physical activity lowers inflammatory markers, improves insulin sensitivity and endothelial function, and is associated with slower decline in eGFR.
Therefore, it is recommended that CKD patients with diabetes perform at least 150 minutes of moderately intense physical activity per week. Nonetheless, such patients tend to be elderly with increased risk of falls, obese, and anaemic, with further limitations in their functional capacity, so care needs to be taken.
Use of tobacco is a leading cause of death and also promotes the development of CKD, with a higher incidence of CV events noted among current and former smokers in diabetics with CKD versus never smokers. Second hand exposure is also associated with CKD and kidney disease.
Therefore, diabetics with CKD, along with the general population, are advised to stop using tobacco products, with the help of pharmacotherapy and behavioural support. E-cigarettes are not recommended due to emerging links with lung cancer and CVD, and their impact on kidney disease is not fully known.
Pharmacological therapy
Angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB): It is recommended that patients with diabetes, hypertension, and albuminuria are started on ACEi or ARB, with dose titration as needed. Albuminuria is associated with increased risk of progression of CKD, and ultimately kidney failure, and with increased risk of CVD. Several trials have shown that through RAS (renin-angiotensin-system) blockade, ACEi, and ARBs were effective in reducing albuminuria and even reversal of moderately increased albuminuria, slowing the rate of kidney function loss.
Use of ACEi/ARBs in type 2 diabetes (T2D), albuminuria, and without hypertension are beneficial. However, their use is not beneficial for patients with neither albuminuria nor elevated BP. For CKD patients with T2D and hypertension, but normal urine albumin excretion, BP control with any anti-hypertensive class is important to prevent CVD.
Serum creatinine, eGFR, and potassium should be measured within two to four weeks of starting treatment or making a change in the dose of ACEi/ARBs. These drugs block the action of angiotensin II, leading to selective vasodilatation of the efferent arterioles, resulting in a decrease in the intraglomerular pressure with consequent rise in creatinine and decrease in eGFR, and block the action of aldosterone, potentially leading to hyperkalaemia. ACEi should not be combined with ARBs as this can lead to hyperkalaemia and acute kidney injury (AKI).
It is also important to advise contraception for women of child-bearing age or to discontinue treatment in women who are pregnant or planning to conceive, as ACEi/ARBs are associated with neonatal complications, especially when continued in the second/third trimester including:
Impaired foetal or neonatal kidney function resulting in oligohydramnios during pregnancy and kidney failure after delivery;
Pulmonary hypoplasia;
Limb defects;
Cerebral complications;
Miscarriages or perinatal death.
ACEi can also cause dry cough and angioedema due to inhibition of bradykinin. Switching to ARBs is an option in such cases. Treatment should begin with the lowest possible dose and titrate to the maximum tolerated one, as with increasing dose, side-effect risks increase.
Sodium-glucose cotransporter-2 inhibitors (SGLTi): SGLTi are recommended for the treatment of patients with T2D, CKD, and eGFR ≥20ml/min per 1.73m2. These drugs inhibit kidney tubular reabsorption of glucose leading to lower blood glucose. In view of this glycosuria, a diuretic effect is caused, leading to increased urine output. SGLTi also alter metabolism by shifting away from carbohydrate utilisation to ketogenesis, leading to lower HbA1c, BP, and weight. In addition, they lead to a reduction in intraglomerular pressure and subsequent preservation of kidney function.
SGLTi are associated with CV and heart failure (HF) benefits, with reduction in CV death, all-cause mortality, and HF hospitalisation compared to placebo. Kidney benefits include a slower decline in eGFR, reduction in albuminuria, and reduced risk of dialysis, kidney transplant, and death from renal causes.
With regards to initial therapy for patients not yet started on glucose-lowering drugs, different guidelines recommend different regimens, with some suggesting starting with metformin and others starting with SGLTi. Based on the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, it is recommended that most T2D CKD patients with an eGFR ≥30ml/min per 1.73m2:
Start with a combination of metformin and SGLT2i;
Once eGFR declines to 30-45ml/min/1.73m2, maximum dose of metformin should be halved;
Once eGFR <30ml/min/1.73m2 or the patient is started on dialysis, metformin is stopped;
Metformin can be administered to kidney transplant patients as long as eGFR is ≥30ml/min per 1.73m2 ;
Once eGFR <20ml/min/1.73m2 one can continue treatment with SGLTi;
Very little data is available once patients are started on dialysis or have received a kidney transplant, so discontinuation of SGLTi is recommended at this stage;
SGLTi should not be started if eGFR is ≤20ml/min per 1.73m2.
When used as monotherapy, the risk of hypoglycaemia with SGLTi is low as the drug-induced glycosuria decreases as blood glucose normalises. However, when used with other therapies that can cause hypoglycaemia, the dose of these pre-existing medications needs to be adjusted. Withhold SGLTi during times of prolonged fasting or surgery, when patients may be at a greater risk of ketosis.
In patients at risk of hypovolaemia, reduce thiazide or loop diuretic before starting treatment with SGLTi, as SGLTi are associated with an initial natriuresis. SGLTi can cause a reversible decrease in eGFR. An eGFR drop of ≤30 per cent should be tolerated and should not lead to discontinuation of treatment. If eGFR drops further, ensure the patient is not hypovolaemic, adjust diuretic dose, and seek other possible causes of the AKI. CKD or HF patients without T2D can be started on SGLTi, as they offer CV and kidney protection without conferring an increased risk of hypoglycaemia or diabetic ketoacidosis.
Diabetic ketoacidosis is a rare side-effect of SGLTi, as is an increased risk of genital mycotic infections.
Nonsteroidal mineralocorticoid receptor antagonist: Nonsteroidal mineralocorticoid receptor antagonist (MRA) are recommended for T2D patients with ≥eGFR 25ml/min/1.73m2, normal serum potassium concentration, and albuminuria ≥30mg/g despite on maximum tolerated dose of ACEi/ARBs. Through the use of ACEi/ARBs, there is kidney and CV benefit via RAS blockade.
Nonetheless, data has shown that there is incomplete suppression of serum aldosterone levels, thereby suggesting the need for further treatment to reduce residual albuminuria. Steroidal MRA are used to treat primary hyperaldosteronism levels, HF, and to reduce albuminuria, but data is lacking with regards to their effect on kidney disease progression. Moreover, they can cause hyperkalaemia and AKI, and spironolactone is associated with gynaecomastia.
Novel nonsteroidal MRA such as finerenone are more selective for mineralocorticoid receptors, and confer CV and renal benefits with reduced albuminuria and slower decline in eGFR. They are also associated with a lower risk of hyperkalaemia compared to steroidal MRA.
Patients with T2D, CKD, and albuminuria on SGLTi and ACEi/ARBs can also start taking finerenone, provided that they have a normal serum potassium and albumin to creatinine ratio is ≥30mg/g. Use of SGLTi also reduces the risk of hyperkalaemia in patients already on ACEi/ARBs and finerenone. Moreover, finerenone can be added to patients on ACEi/ARBs only, despite not being on SGLTi.
A steroidal MRA is used in the treatment of HF, hyperaldosteronism, and refractory hypertension. Clinical evidence is lacking whether switching from a steroidal to nonsteroidal is associated with an improvement in clinical outcome. When the patient is treated with neither and has T2D, HF, and albuminuria and is already on ACEi/ARBs and SGLTi, treatment should be based on the most concerning clinical indication. At present, a nonsteroidal MRA cannot replace a steroidal MRA for HF and hyperaldosteronism.
Finerenone can cause hyperkalaemia, and monitoring of this electrolyte is important. Treatment with finerenone should not be started if serum potassium is >5mmol/l. Finerenone has a short half-life, therefore stopping the drug for 72 hours will lead to resolution of the elevated potassium.
Steroidal and nonsteroidal MRA should not be combined due to risk of hyperkalaemia. Steroidal MRA are currently contraindicated in pregnancy, and in view of the lack of clinical data of the use of nonsteroidal MRA in pregnancy, this drug should be stopped.
Other anti-hypertensive treatment: KDIGO guidelines recommend that patients with albuminuria, T2D, CKD, and hypertension are started on ACEi/ARBs until maximum tolerated dose. If patients have normal serum potassium and albumin to creatinine ratio is ≥30mg/g, finerenone can be added. If this is not the case and BP is still high, dihydropyridine calcium channel blocker and/or diuretic can be added. Should BP still remain high and eGFR ≥45, steroidal MRA can be added.
Glucagon-like peptide-1 receptor agonists: In T2D CKD patients who have not achieved the desirable glycaemic targets despite lifestyle interventions, treatment with metformin and SGLT2i, or in whom the latter two medications are not tolerated, guidelines recommend prioritising glucagon-like peptide-1 receptor agonists(GLP-1 RA) over other glucose lowering therapies.
GLP-1 RA have been shown to improve glycaemic control, confer weight loss and CV benefit, reduce albuminuria, and slow the rate of eGFR decline. In view of their proven CV benefit, GLP-RA are preferred over other glucose-lowering therapies (Dipeptidyl peptidase-4 inhibitor (DPP-4) inhibitors, thiazolidinediones, sulfonylureas, insulin). The risk of hypoglycaemia is generally low when GLP-1 RA are used alone. When used with other medications, the risk is increased, so the dose of sulfonylurea and/or insulin may need to be reduced.
GLP-1 RA may be preferentially used in patients with obesity, T2D, and CKD to promote intentional weight loss. Further studies are required regarding the use of GLP-1RA in patients with very advanced CKD, patients on dialysis, and in kidney transplant recipients. Side-effects of GLP-1 RA include nausea/vomiting, diarrhoea, and increased heart rate. Also, since most of them are given as a subcutaneous injection, they are associated with pain over the injection site. These medications are contraindicated in patients with a history of medullary thyroid carcinoma, multiple endocrine neoplasia 2, and patients with a history of acute pancreatitis.
Other glycaemic treatment: If the glycaemic target is still not achieved despite lifestyle interventions, metformin, SGLTi, and GLP-1 RA, then other glucose-lowering agents can started, such as DPP-4 inhibitors, thiazolidinediones, sulfonylureas, and insulin.
Monitoring of blood glucose in T2D CKD patients
HbA1c is recommended to monitor glycaemic control in these patients, measured twice a year, or up to four times/year should glycaemic targets not be met. However, inflammation, oxidative stress, and metabolic acidosis associated with CKD, as well as anaemia, transfusions, and use of iron replacement therapies and erythropoiesis-stimulating agents, affect HbA1c level. These effects become more pronounced as the CKD advances or patients are treated with dialysis. Once HbA1c levels are not concordant with blood glucose levels, continuous glucose monitoring and self-monitoring of blood glucose can be used, as these are not influenced by CKD, dialysis, or other treatments. One should aim for target HbA1c of <6.5-to-8.0 per cent, with levels ≤6.0 per cent associated with greater risk of hypoglycaemia and increased mortality.
Dyslipidemia treatment
Managing dyslipidaemia, according to KDIGO recommendations, includes:
CKD patients are at increased risk of adverse events when statins and fibrates are combined. Since statins confer a greater clinical benefit compared to fibrates, statins are preferred.
Statin or statin/ezetimibe combination in adults aged ≥50 with eGFR ≤60ml/min/1.72m2, not on dialysis and without kidney transplant. Ezetimibe monotherapy is not recommended.
Statin in adults aged ≥50 with eGFR ≥60ml/min/1.72m2.
Statin in adults aged 18 to 49 with CKD, but not on dialysis and without kidney transplant if they have coronary disease (myocardial infarction or coronary revascularisation); diabetes mellitus; prior ischaemic stroke; estimated 10-year incidence of coronary death or non-fatal myocardial infarction >10 per cent.
If at the time of dialysis initiation, patients are already on statin or statin/ezetimibe combination, this can be continued.
Do not start statin or statin/ezetimibe combination in dialysis patients.
In adult kidney transplant recipients, treatment with a statin is recommended.
Statins are contraindicated in pregnant or breastfeeding females, patients with active liver disease or in patients in whom transaminase levels are three times or more the upper limit of normal.
For additional risk-based therapy, aspirin can be used lifelong for secondary prevention among those with established CVD. Ezetimibe or proprotein convertase subtilisin-kexin type 9 inhibitors (PCSK9i) can be added to a statin. PCSK9i can be used in statin-intolerant patients, with these medications showing an improvement in lipid profile and CV risk. Nonetheless, further studies are needed to ascertain their safety in patients with eGFR ≤20ml/min/1.73m2, those on dialysis, and/or renal transplant patients.
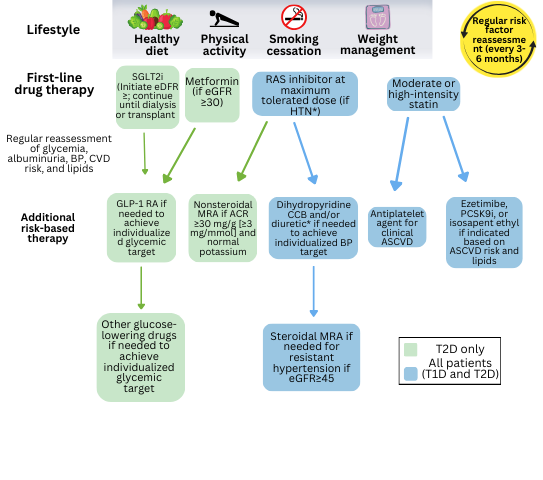
FIGURE 1: KDIGO management of patients with DKD
Conclusion
DKD is a constantly evolving subject with new guidelines issued very frequently. Nonetheless, a patient-centred approach with involvement of relatives and multidisciplinary team is required to achieve the best care possible, including involvement of nutritionist, physiotherapist, personal trainer, smoking cessation support, endocrinologist, cardiologist, GP, and various other medical disciplines.
KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease provides evidence-based recommendations and can be accessed at: www.kdigo.org/wp-content/uploads/2022/10/KDIGO-2022-Clinical-Practice-Guideline-for-Diabetes-Management-in-CKD.pdf.
The HSE is seeking additional funding to include chronic kidney disease (CKD) in the GP chronic disease management (CDM) programme in 2025, it has confirmed. The prevalence of CKD is significantly increasing in Ireland. Some 15.6 per cent of people aged 50 and over have CKD, but most are unaware, according to research published last year by TILDA and the National Renal Office (NRO).
The HSE has stated that recommendations from a review of the NRO are still being considered in the context of health service structural changes. The review was commissioned to examine the current and future work of the NRO, which was established in 2009 before the initiation of the HSE clinical programmes. Its original remit was end-stage kidney disease. The office now requires support for work in other areas, including preventative nephrology.
Commenting on the inclusion of CKD into the CDM programme, the Irish Kidney Association said: “We need to see the Government include provision for this positive development in the forthcoming Budget. We have seen the benefits for cardiac care as well as diabetes and hypertension management. Including CKD will be a significant move towards proactive health management in the general population. Remember, one-in-10 in the population has CKD, including one-in-seven of those over the age of 50.”
General practice completed 99,098 reviews of patients enrolled in the CDM programme in the first two months of 2024, according to figures provided to NiGP. The Department of Health also confirmed that it believes the programme is “the main contributing factor” in a reduction of chronic disease-related hospital admissions in recent years.
“The CDM programme forms part of the wider enhanced community care programme which has improved patient care and provided ongoing improvements to how health services are delivered,” said the Department’s spokesperson.
This reduction in hospital admissions was discussed at the Sláintecare programme board meeting in April. Board members were shown data that indicated a 16 per cent reduction in chronic disease-related hospital admissions as compared to a 3.5 per cent reduction in all other medical admissions per 100,000 population between 2019 and 2023.
The meeting was also told that 91 per cent of patients on the programme “are now fully managed routinely in primary care” and are not attending hospital for ongoing management of their condition. The CDM programme commenced in 2020. It has been rolled out on a phased basis to adult patients with a medical or GP visit card. Approximately 94 per cent of eligible GPs have signed up to providing the CDM programme.
Progress in the treatment of diabetic kidney disease: Feast after famine?
By
Rachel Bonner, Sara Brady, Dr Dean Moore, and Dr Eoin Brennan
- 01st Sep 2024
The origin of the term ‘diabetes’ is an ancient one. Between the 1st and 2nd Century BCE, Demetrius of Apaemia is generally credited with deploying the term, διαβαίνω (diabaino), derived from an Ionic word meaning ‘to pass through’, as fluid through a syphon.1 While definitive sources regarding etymology are elusive, the disease has doggedly troubled humanity for millennia. Diabetes and its complications reach across almost all medical specialities, and the battle to prevent, protect, and restore end-organ damage has produced a variety of treatments with various levels of success over recent decades.
The microvascular complications of diabetes include retinopathy, neuropathy, and diabetic kidney disease (DKD). DKD is one of the most severe complications of diabetes mellitus and is the leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) worldwide. The progressive nature of DKD, coupled with the increasing prevalence of diabetes, underscores the urgent need for effective management strategies. This article delves into these advancements, highlighting novel therapeutic approaches and comprehensive management strategies.
Understanding DKD globally and locally
DKD, also known as diabetic nephropathy, is usually characterised by persistent albuminuria or overt proteinuria, a progressive decline in glomerular filtration rate (GFR), and an increased risk of cardiovascular events. It develops in approximately 40 per cent of patients with diabetes and is a significant contributor to morbidity and mortality. Globally, the prevalence of CKD is approximately 10 per cent with around 30 per cent of all disability adjusted life years in CKD attributable to DKD.2
Last year, 2023, saw the release of Chronic Kidney Disease in Community-Dwelling Adults Aged 50+ Years in Ireland: A Report from TILDA and the National Renal Office.3 This analysis offered the first large population-based data set in the Republic of Ireland and made for interesting, albeit concerning, reading. The prevalence of CKD in adults in the community in Ireland aged 50 years or older was 11.7 per cent in 2009-2011, but rose to 15.6 per cent in 2014-2015. The national prevalence of CKD stage 3 or greater in individuals with diabetes mellitus was 25.21 per cent.
The apparent excess in prevalent CKD in Ireland compared to global figures is difficult to parse given the heterogeneous nature of the data used to compile global figures and estimates. However, the demographic trends unique to Ireland may explain part of this excess, with the percentage of those 65 or older growing faster than all comparative EU neighbours.4
The pathogenesis of DKD involves a complex interplay of metabolic, haemodynamic, and inflammatory factors. Hyperglycaemia, hypertension, and dyslipidaemia are key contributors, leading to glomerular hyperfiltration, increased permeability of the glomerular basement membrane, and tubulointerstitial fibrosis. Chronic inflammation and oxidative stress further exacerbate kidney damage, culminating in progressive renal function decline. The recognition and deeper understanding of this complicated milieu has led to advances in the application of novel agents to treat DKD.
Advances in therapeutic approaches
While the utility of optimum glycaemic control is established in reducing the likelihood of onset of DKD, in established disease it is of little utility in preventing progression. The treatment of DKD has evolved in the last decade beyond just glycaemic control and blood pressure management with the introduction of new therapeutic agents. These novel agents include sodium-glucose co-transporter (SGLT2) inhibitors, glucagon-like-peptide (GLP)-1 receptor agonists, and non-steroidal mineralocorticoid receptor antagonists (nsMRAs), amongst others. While most of these agents have been used for a variety of indications, recent trials with kidney-specific endpoints in populations with CKD have been published and strengthened the current trends in the clinical management of DKD.
1. SGLT2 inhibitors Although SGLT-2 inhibitors were introduced in clinical practice to regulate hyperglycaemia in diabetes, it is now common knowledge that the beneficial effects of these agents on the kidney and cardiovascular system are independent of glucose-lowering. They exert pleiotropic responses including regulating renal epithelial cell integrity and inflammation. These agents reduce glucose reabsorption in the proximal tubules, leading to increased glycosuria, and reduce glomerular hyperfiltration via tubuloglomerular feedback.
While the nephroprotective effects of SGLT2 inhibitors were first noted as secondary endpoints of cardiovascular outcome trials, specific evidence for renal outcomes came from dedicated kidney-focused trials: CREDENCE, DAPA-CKD, and finally EMPAKIDNEY.5,6,7 This class is also especially appropriate for those with concurrent heart failure, regardless of the level of albuminuria.
SGLT2 inhibitors and renin-angiotensin system (RAS) inhibitors – angiotensin-converting-enzyme (ACE) inhibitor or angiotensin-receptor blocker (ARB) – have both been shown to delay the progression of CKD and remain the mainstay of treatment for the disease at present.
2. GLP-1 receptor agonists GLP-1 receptor agonists, another class of antidiabetic agents, have shown promise in the management of DKD, again independent of the effect on glycaemic control. First extracted from the venom of the Gila monster, these drugs improve glycaemic control, famously promote weight loss, and have well-demonstrated cardiovascular benefits. Mechanistically, GLP-1 receptor agonists counter hyperglycaemia by augmenting insulin secretion, impairing glucagon release, and delaying gastric emptying, as well as centrally promoting satiety via direct neurohormonal signalling.
Studies like LEADER and SUSTAIN-6 have demonstrated that GLP-1 receptor agonists such as liraglutide and semaglutide can reduce the risk of nephropathy as measured by reductions in proteinuria and possible slowing of decline in estimated GFR (eGFR).8,9 Again, the paucity of data in CKD populations with dedicated primary renal outcomes had tempered the nephrology community’s widespread use of GLP-1s.
The FLOW trial demonstrated that once-weekly subcutaneous semaglutide significantly decreased the risk of progression of DKD without significant adverse effects or safety concerns.10 While this data is concordant with previous trials, more than 90 per cent of participants had albuminuria and almost 80 per cent had an eGFR <60ml/min/1.73m2. While certain limitations (no type 1 diabetics, co-administration of SGLT2 inhibitors was not necessary) leave questions to be answered, semaglutide seems to have established its place in the armamentarium of pharmacotherapy for DKD.
3. MRAs The overactivation of the mineralocorticoid receptor in patients with diabetes and CKD leads to kidney and cardiovascular damage through the induction of inflammatory and fibrotic pathways. Steroidal (sMRAs) such as spironolactone and eplerenone have been shown to reduce albuminuria. However, their impact on clinical renal outcomes is uncertain and their side-effect profile, including the risk of hyperkalaemia and acute kidney injury (AKI), limits their use in high-risk populations.
nsMRAs such as finerenone demonstrate superior selectivity for mineralocorticoid receptors with no dramatic increase in side-effects related to androgen and oestrogen activity. Two large phase 3 trials have now shown the cardiovascular and renal benefits of finerenone in patients with type two diabetes (T2DM) and DKD. Pre-clinical models have shown that finerenone had greater anti-inflammatory and anti-fibrotic effects than sMRAs, however, its effect on kidney disease progression had not been reported until these trials.
The FIDELIO-DKD trial demonstrated that the use of finerenone in the treatment of patients with T2DM and CKD already being treated with RAS blockade resulted in a lower risk of CKD progression and cardiovascular events than the placebo group.11 CKD exacerbates the risk of adverse cardiovascular events associated with T2DM. The FIGARO-DKD trial concluded that finerenone reduced the risk of cardiovascular outcomes in participants with T2DM and CKD being treated with RAS inhibitors.12 The rate of mortality due to cardiovascular causes, nonfatal myocardial infarctions and strokes, and heart failure-related hospitalisations were all decreased in the finerenone group.
The FIDELITY analysis is a pooled analysis that was then conducted of the FIDELIO-DKD and FIGARO-DKD trials to demonstrate the efficacy and safety of finerenone in a wide range of patients with CKD and T2DM.13 This analysis, involving 13,026 patients across the two trials, confirmed the reported evidence that finerenone had both renal and cardiovascular protective effects.
International guidelines now suggest the addition of finerenone to first-line therapy for patients with T2DM and a high risk of CKD progression and cardiovascular events based on the results from these trials. However, some potential concerns include the higher rate of hyperkalaemia seen in the finerenone group in comparison to the control. There is also a lack of definitive data describing the effect of combining nsMRAs and SGLT2 inhibitors, but this is currently being investigated in the CONFIDENCE study.14
4. ‘Aldosterone breakthrough’ and aldosterone synthase inhibitors Mindful of the established role of the renin-angiotensin-aldosterone system (RAAS) in kidney disease generally, and DKD specifically, several different approaches to modify the pathway using novel mechanisms have been attempted. Direct renin inhibitors as well as combining ACE inhibitors and ARBs have been examined in previous studies, but have proven unsuccessful commercially and demonstrated unacceptable side-effect profiles respectively.15
Aldosterone breakthrough is a concept that has led to the re-examination of the RAAS. After being first described in the 1980s,16 and confirmed in studies since, it elaborates on the effect of chronic RAAS inhibition and the resultant increase in aldosterone synthesis. Rates of breakthrough are reported variously as between 10 and 50 per cent,17 thus the deleterious effects of elevated aldosterone may perpetuate kidney disease despite achieving the intended clinical goal. This effect is effectively bypassed with the use of aldosterone synthase inhibitors (ASIs).
Other benefits include sparing the (necessary) cortisol-mediated activation of the mineralocorticoid receptor as part of ‘fight or flight’ responses, preventing the non-genomic effects of aldosterone (which are not inhibited by MRAs) and definitively avoiding the off-target oestrogenic effects of MRAs.
Last year saw the first phase 2 trial of ASI.18 Encouragingly, in a patient population of established CKD, the majority of whom were diabetic, a significant decrease in proteinuria was detected both with and without SGLT2 inhibitors. Limited instances of adrenal insufficiency, hyperkalaemia, and AKI were noted and further trials are ongoing examining the role of ASIs in proteinuric CKD and for the treatment of hypertension.
Combination therapy for DKD – searching for synergy
The hunt for a multiple-drug regime in treatment for patients with DKD is an attractive avenue of research. The ability to tailor a treatment regimen for DKD could offer benefit in slowing the progression of disease while avoiding the potential side-effects that any one class alone may cause. The current guideline-recommended drug therapies may not be of benefit to all patients, as DKD is a heterogeneous disease; however, it is difficult to determine which drugs will be of benefit to specific individuals.
RAS inhibitors and SGLT2 inhibitors both decrease glomerular hypertension and hyperfiltration. The RECOLAR trial showed encouraging results in patients with T2DM.19 The combination of empagliflozin and losartan in people with T2DM had a larger blood pressure-lowering effect versus placebo than either of the drugs alone. This data shows that a combination of a RAS inhibitor and an SGLT2 inhibitor has a positive additive effect on markers of systemic and glomerular haemodynamic function. However, there is a risk of AKI when administering drugs that reduce glomerular pressure as this could lead to hypoperfusion of the kidneys. Further investigation is required to delve deeper into the significance of this risk.
The DURA-TION-8 study of patients with T2DM showed that the combination of an SGLT2 inhibitor and a GLP-1 receptor agonist had a greater positive effect on glycaemic control, body weight, and blood pressure than monotherapy.20 Similarly, in the DECADE study, patients with DKD given a combination of dapagliflozin and exenatide resulted in a greater decrease in albuminuria than monotherapy.21
The ROTATE-3 study demonstrated the additive effect of the sMRA eplerenone and SGLT2 inhibitor-dapagliflozin. The results showed that the combination of the drugs resulted in a greater reduction of albuminuria than monotherapy.22 Additionally, in this study it was seen that dapagliflozin partly attenuated the increased serum potassium levels that eplerenone can induce. The hypothesis of SGLT2 inhibitors increasing the renal protective effects of MRAs is currently being investigated in he phase 2 CONFIDENCE trial, as previously mentioned.14
Conclusion
The management of DKD has witnessed significant advancements in recent years, driven by a deeper understanding of disease mechanisms and the development of novel therapeutic agents. SGLT2 inhibitors, GLP-1 receptor agonists, nsMRAs, and ASIs represent major breakthroughs in the treatment of DKD, offering renal and cardiovascular protection beyond traditional therapies. The concept of ‘4 pillars of DKD’ management has now gained significant currency as the cornerstone of treatment (namely RAAS inhibition, SGLT2 inhibitors, GLP1 agonists, and nsMRAs.
As research continues to unravel the complexities of DKD, it is imperative to translate these advancements into clinical practice to improve the lives of patients with diabetes and prevent the progression to ESKD. The integration of novel therapies, personalised medicine approaches, and innovative technologies will be key to achieving this goal and addressing the rapidly growing burden of DKD in Ireland and worldwide, perhaps lessening even more the burden of a disease recognised since antiquity as a smouldering and pernicious affliction.
“…. because the fluid does not remain in the body, but uses the man’s body as a ladder, whereby to leave it… and many parts of the flesh pass out along with the urine.” The first description of diabetesby Aretaeus of Cappadocia
References
1. Gemmill CL. The Greek concept of diabetes. Bull N Y Acad Med. 1972;48(8):1033-1036. 2. Jadoul M, Aoun M, Masimango Imani M. The major global burden of chronic kidney disease. Lancet Glob Health. 2024;12(3):e342-e343. 3. Nowak N, Mellotte G, O’Halloran A, et al. Chronic kidney disease in community-dwelling adults aged 50+ years in Ireland: A report from TILDA and the National Renal Office. 2023. Available at: www.tilda.ie. 4. Department of Health. Health in Ireland – Key Trends 2023. Dublin: DoH; 2023. Available at: www.gov.ie/en/publication/ccc4b-health-in-ireland-key-trends-2023/. 5. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295-2306. 6. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436-1446. 7. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117-127. 8. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. 9. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016; 375(4):311-322. 10. Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. Published online May 24, 2024. 11. Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219-2229. 12. Pitt B, Filippatos G, Agarwal R, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med. 2021;385(24):2252-2263. 13. Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: The FIDELITY pooled analysis. Eur Heart J. 2022;43(6):474-484. 14. Green JB, Mottl AK, Bakris G, et al. Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE). Nephrol Dial Transplant. 2023;38(4):894-903. 15. Fried LF, Emanuele N, Zhang JH, et al. Combined angiotensin inhibition for the treatment of diabetic nephropathy [published correction appears in N Engl J Med. 2014;158:A7255]. N Engl J Med. 2013;369(20):1892-1903. 16. Staessen J, Lijnen P, Fagard R, et al. Rise in plasma concentration of aldosterone during long-term angiotensin II suppression. J Endocrinol. 1981;91(3):457-465. 17. Bomback AS, Klemmer PJ. The incidence and implications of aldosterone breakthrough. Nat Clin 18. Pract Nephrol. 2007;3(9):486-492. Tuttle KR, Hauske SJ, Canziani ME, et al. Efficacy and safety of aldosterone synthase inhibition with and without empagliflozin for chronic kidney disease: A randomised, controlled, phase 2 trial. Lancet. 2024;403(10424):379-390. 18. Scholtes RA, Mosterd CM, Hesp AC, et al. Mechanisms underlying the blood pressure-lowering effects of empagliflozin, losartan and their combination in people with type 2 diabetes: A secondary analysis of a randomised crossover trial. Diabetes Obes Metab. 2023;25(1):198-207. 19. Frías JP, Guja C, Hardy E, et al. Exenatide once-weekly plus dapagliflozin once-daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy (DURATION-8): A 28-week, multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 2016;4(12):1004-1016. 20. van der Aart-van der Beek AB, Apperloo E, Jongs N, et al. Albuminuria-lowering effect of dapagliflozin, exenatide, and their combination in patients with type 2 diabetes: A randomised cross-over clinical study. Diabetes Obes Metab. 2023;25(6):1758-1768. 21. Provenzano M, Puchades MJ, Garofalo C, et al. Albuminuria-lowering effect of dapagliflozin, eplerenone, and their combination in patients with chronic kidney disease: A randomised crossover clinical trial. J Am Soc Nephrol. 2022;33(8):1569-1580.
Exercise and physical activity in CKD, dialysis, and kidney transplant
By
Orlaith Heslin and Laura McCullagh
- 01st Jul 2024
It is often said that if exercise was a pill, it would be one of the most widely prescribed and cost-effective drugs ever invented. This is also true when looking at the management of chronic kidney disease (CKD), where exercise is a powerful, yet often underutilised tool.
The Irish Longitudinal Study on Ageing (TILDA) revealed in 2023 that the prevalence of CKD in Ireland is rising, with more than one-in-seven people over the age of 50 having the condition. However, 98 per cent of people do not know they have the condition. Patients with hypertension or diabetes are up to three times more likely to have CKD.¹
This study highlighted the importance going forward of action in primary and secondary care to raise awareness and to improve outcomes for people living with CKD in Ireland. It remains crucially important to emphasise the benefits of exercise and physical activity to our patients.
Globally, 28 per cent of adults are insufficiently active, and this sedentary behaviour is predicted to lead to 500 million new cases of non-communicable diseases before 2030.² Research indicates that those living with CKD are at particular risk of a sedentary lifestyle, and should be counselled regularly and encouraged to engage in exercise and physical activity as part of their regular treatment. However, this patient population are not routinely offered support as part of their care, with healthcare providers citing reasons such as lack of skills, time, and resources to access and implement exercise programmes.³
When managing many other chronic conditions, such as chronic obstructive pulmonary disease, or recovery following a cardiovascular event, exercise is a staple part of treatment, and there is access to pulmonary or cardiac rehabilitation services all over Ireland.
However, this is not always the case when looking at the management of CKD, despite the already well-established links between CKD and cardiovascular disease (CVD).4 With the role of the renal physiotherapist still in its infancy in Ireland, it is clear to see that there is a significant missed opportunity to improve physical, functional, psychological, and emotional outcomes for patients with high levels of frailty and CVD risk factors throughout all stages of CKD.
Physical activity recommendations
The terms physical activity and exercise are often used interchangeably in healthcare. Physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure, and encompasses everyday activities and hobbies such as gardening, housework, or playing a musical instrument. However, exercise is a subset of physical activity that is planned, structured, and repetitive, with the goal of improving or maintaining physical fitness.5
Some patients with CKD may be active, whether that be in work or day-to-day routines, but do not engage in formal exercise. While regular physical activity is important and helps to reduce the comorbidities associated with a sedentary lifestyle, in order to gain optimal benefits, patients should participate in regular structured exercise. This can range from an exercise class online or in person, to a daily walk.
The guidance has been consistent around exercise where there are no contraindications. As per the World Health Organisation and the UK Renal Association’s Clinical Practice Guidelines: ‘Exercise and Lifestyle in Chronic Kidney Disease’ published in 2022, the recommendations for people with CKD are the same as those for the general population – to aim for 150 minutes per week of moderate-intensity or 75 minutes per week of vigorous-intensity exercise.6 Exercise that aims to improve or maintain strength, balance, and flexibility is recommended to be completed at least twice per week.
Early management – exercise and lifestyle
In individuals with CKD, physical inactivity increases the risk of mortality, accelerates disease progression, and negatively impacts health-related quality-of-life. Management of CKD is a multifaceted approach, however, the general focus can often be on the pharmacological perspective of the disease, with not enough emphasis on lifestyle advice and intervention.
Holistic healthcare incorporates physical, mental, emotional, social, and spiritual components of health, and the management of CKD is no different. This requires a multidisciplinary team (MDT) approach for the best patient outcomes. Exercise will not have the greatest effect alone, and is much more influential when implemented alongside advice from other MDT members on dietary and behavioural modifications.
In pre-dialysis CKD, regular physical activity and exercise can lead to reductions in body weight, improvements in blood pressure, physical function and capacity, functional limitations, and health-related quality-of-life.6
There is a timeline of kidney disease progression, and at each of these stages there is one constant – the benefit of exercise and lifestyle advice. The recommended levels of activity might initially seem overwhelming for someone with a largely sedentary lifestyle, and people with CKD often fear exercise and potential injuries.
Early conversations and advice about lifestyle and exercise will promote best outcomes, and given the complex nature of CKD, guided, structured, and supervised exercise prescriptions from a trained professional are crucial to enhance patients’ knowledge, confidence, and awareness of safe exercise practices, fostering long-term engagement in new lifestyle changes.
Role of exercise in ESKD
For patients with end-stage kidney disease (ESKD), there are two options that may be considered beyond conservative management – dialysis or transplant.7 The National Renal Office (NRO) tracks the prevalence of patients receiving renal replacement therapy (RRT) in Ireland – either dialysis or transplant – and trends over the past 20 years show the demand for adult RRT has more than doubled.8
So, what does dialysis and ESKD mean in terms of exercise? Unfortunately, the majority of those receiving dialysis fall far below the threshold of the recommended levels of physical activity, and these patients experience higher levels of frailty, risk of falls, sarcopaenia, and hospital admissions than the general population.
There are a number of barriers to exercise for this cohort, including the challenges of regular hospital commutes to appointments and dialysis, fatigue, and multiple medical co-morbidities.9 It has also been shown that commencing dialysis is linked to a higher risk of functional impairment, frailty, mood disorders, and CVD.
Exercising while receiving dialysis, known as intradialytic exercise, may not be what many would consider a typical form of exercise, but there is an abundance of data supporting a multitude of benefits. Intradialytic exercise also has the potential to overcome many of the traditional barriers to exercise, such as time and commutes to appointments/sessions.
It is a safe, feasible, and effective way to reduce hospitalisations, improve quality-of-life, cardiovascular health, physical function, and muscular strength.6,10
The Renal Association’s Clinical Practice Guidelines on Haemodialysis¹¹ clearly outline the recommendation for intradialytic exercise to be available in all dialysis units; however, these programmes are not yet routinely established throughout Ireland. Intradialytic exercise should include aerobic and resistance training for at least 30 minutes per haemodialysis session, and the best results are seen with programmes lasting longer than six months.
Aerobic exercise can be carried out on a specialised lower limb bike which can be used while a patient is resting in bed or a chair, and resistance training can be completed using resistance bands and/or handheld dumbbells or ankle weights.
It is recommended that all exercise is supervised by an appropriately trained member of staff, for example, a physiotherapist. If we consider the data from the NRO showing the significant number of patients on dialysis, it is important these patients have access to the resources, education, and research available about the benefit of exercises.
Similarly, for those completing peritoneal or haemodialysis at home, exercise is also shown to be extremely effective. Adequate levels of physical function are required to maintain strength and independence for people choosing to complete home-based therapy, and again, the addition of core exercises into a structured exercise programme for these patients is recommended and best led by an exercise professional.¹²
Exercise post-kidney transplant
For patients affected by ESKD, renal transplant can often represent a dramatic improvement in quality-of-life. However, the requirement for physical activity and exercise does not stop at kidney transplantation, as we now move to the maintenance stage of the exercise journey.
Kidney transplant recipients continue to face a heightened risk of cardiovascular, metabolic, and infectious diseases. Post-kidney transplant patients frequently report low physical activity, low energy, fatigue, poor exercise capacity, and a sedentary lifestyle.
To limit disease progression, enhance quality-of-life, and optimise physical function, a multidisciplinary renal rehabilitation approach – incorporating medical nutrition therapy and regular exercise – is recommended to support this population.6
Digital health interventions
Remote digital health interventions have been shown to be beneficial in improving physical activity and physical function across various chronic conditions.¹³ Although there are many health apps on the market, most are designed for the general population.
While they remain beneficial for those living with CKD, they are not specifically tailored to this population, and patients may not feel safe and assured that the exercises are suitable for them given the complexities of their condition.
Kidney Beam, developed by Dr Sharleen Greenwood, Consultant Physiotherapist, King’s College Hospital, London, UK, is a kidney-specific exercise and lifestyle management website/app designed to support, empower, and improve the lives of people living with CKD. Kidney Beam offers both live and on-demand exercise classes, education sessions, and programmes that people can complete from the comfort of their own homes.
Evidence from a randomised controlled trial in 2024 showed significant and clinically important improvements in health-related quality-of-life, and in the secondary outcome of physical function, in the Kidney Beam group, who completed a 12-week programme of twice weekly virtual exercise classes and education compared with usual care.¹4
There was also positive trends of improvement for secondary outcomes of symptom burden – social interaction, anxiety/depression, and patient activation – in the Kidney Beam intervention group. Given that access to a specialised renal physiotherapist is not widely available in Ireland and only available in the acute setting, digital health interventions may offer a way to help bridge this gap for patients in the interim.
Conclusion
Maintaining a healthy lifestyle remains a cornerstone in CKD management. However, despite the abundance of research highlighting the benefits of physical activity and exercise in those with CKD, exercise programmes are not always prioritised as part of standard care. Healthcare providers must advocate for and facilitate exercise programmes, while ensuring they are accessible and tailored to the needs of those with CKD in Ireland.
With the persistent increase in numbers of people with CKD, the role of the renal physiotherapist in Ireland is likely to develop further in the near future. It could prove significant in improving health outcomes and empowering patients to take an active role in managing their condition.
The promotion of regular exercise should be a vital component of CKD treatment strategies, aiming to reduce disease progression, enhance life quality, and ultimately provide a path to better health and wellbeing.
References
Nowak N, Mellotte G, O’Halloran A, et al. Chronic kidney disease in community-dwelling adults aged 50+ years in Ireland: A report from TILDA and the National Renal Office. 2023. Available at: www.tilda.ie.
World Health Organisation. Global status report on physical activity 2022. Geneva: WHO; 2022. Available at: www.who.int/teams/health-promotion/physical-activity/global-status-report-on-physical-activity-2022.
Wilund K, Thompson S, Bennett PN. A global approach to increasing physical activity and exercise in kidney care: The International Society of Renal Nutrition and Metabolism Global Renal Exercise Group. J Ren Nutr. 2019;29(6):467-470.
Schrauben SJ, Apple BJ, Chang AR. Modifiable lifestyle behaviours and CKD progression: A narrative review. Kidney360. 2022;3(4):752-778.
Dasso, NA. How is exercise different from physical activity? A concept analysis. Nursing Forum. 2019;54(1):45.
Baker LA, March DS, Wilkinson TJ, et al. Clinical practice guideline exercise and lifestyle in chronic kidney disease. BMC Nephrology. 2022;23(1):75.
Conlon, P, Donnelly P, Dunne, H. Haemodialysis and peritoneal dialysis: A guide for patients, Book 2, 5th edition. 2021. Available at: www.ika.ie/wp-content/uploads/2022/07/BEAUMONT_BOOK_2_2021.pdf.
Health Service Executive. Programme documents and resources: Renal. Dublin: HSE; 2023. Available at: www.hse.ie/eng/about/who/cspd/ncps/renal/resources/.
Li T, Lv A, Xu N, et al. Barriers and facilitators to exercise in haemodialysis patients: A systematic review of qualitative studies. J Adv Nur. 2021;77(12):4679-92.
De Moura Reboredo M, Henrique DMN, De Souza Faria R, et al. Exercise training during haemodialysis reduces blood pressure and increases physical functioning and quality-of-life. Artificial Organs. 2010;34(7):586-93.
Ashby D, Borman N, Burton J, et al. Renal association clinical practice guideline on haemodialysis. BMC Nephrology. 2019;20(1):379.
Bennett PN, Bohm C, Harasemiw O, et al. Physical activity and exercise in peritoneal dialysis: International Society for Peritoneal Dialysis and the Global Renal Exercise Network practice recommendations. Peritoneal Dialysis International. 2022;42(1):8-24.
Zangger G, Bricca A, Liaghat B, et al. Benefits and harms of digital health interventions promoting physical activity in people with chronic conditions: Systematic review and meta-analysis. J Med Internet Res. 2023;25:e46439.
Greenwood SA, Young HML, Briggs J, et al. Evaluating the effect of a digital health intervention to enhance physical activity in people with chronic kidney disease (Kidney BEAM): A multicentre, randomised controlled trial in the UK. Lancet Digit Health. 2024;6(1):e23-e32.
Rising prevalence of chronic kidney disease in Ireland
By
NiGP
- 01st Jan 2024
Jan-Feb 2024 | Issue 2 | Vol 17
New research has revealed that one-in-seven people over 50 have chronic kidney disease (CKD) in Ireland, and 98 per cent do not know they have the condition. The data was released from the largest study to date in Ireland that aims to characterise the population affected by CKD over the age of 50 years.
Trinity researchers analysed data from The Irish Longitudinal Study on Ageing in Ireland (TILDA), a nationally representative cohort study, and conducted the research in collaboration with the HSE. The findings have renewed calls for CKD to be included in the Chronic Disease Management Programme.
Commenting on the findings, Principal Investigator of TILDA Prof Rose-Anne Kenny noted that Ireland is “the fastest ageing country in Europe”, and that early diagnosis of CKD improves management of the disease and patient outcomes. “The data will assist new screening, referral, and management pathways for CKD, and increase independent living and quality-of-life for Irish adults,” she said.
Major findings from the study show:
CKD prevalence in adults aged 50 years and over in Ireland is rising;
– CKD was present in 15.6 per cent of people aged over 50 in Ireland, which equates to approximately 226,000 people;
– 98 per cent of people who had CKD were unaware they suffered from it;
– Whereas blood pressure management should be tightly controlled in CKD to prevent or slow down progression, blood pressure was poorly controlled in CKD sufferers in Ireland;
– New cases of CKD in Ireland in people over 50 are occurring at a rate of 16 people per 1,000 person-years of follow up, which will likely also contribute to substantial future demand on nephrology services and hospital inpatient stay;
– Hypertension was the most common CKD-related condition in the Irish adult population. The estimated prevalence of CKD in Irish adults aged 50+ years without diabetes and hypertension was 6.22 per cent based on Wave 1 data, and 10.01 per cent based on Wave 3 of TILDA. Age, HbA1c, body mass index, and hypertension were significantly correlated with the presence and severity of CKD.
The increasing prevalence of CKD has implications for future treatment policies in nephrology, including healthcare resource allocation planning as part of Sláintecare, as well as the implications of new treatment options for CKD on the Chronic Disease Management Programmes in Ireland.
Prof Donal Sexton Lead author of TILDA and Consultant Nephrologist at St James’ Hospital described the report as “extremely important”, as it highlights “not only how common it [CKD] is but also emphasises the public health requirement to improve awareness and treatment in the light of new approved medications”.
He is among several experts calling for CKD to be incorporated into the Chronic Disease Management Programme in Ireland, to “facilitate improved treatment of the condition in primary care”.
Recommendations from the study include: – Increased awareness of CKD and the adverse health outcomes associated with it are needed, including, cardiovascular disease, kidney failure, and premature death; – The incorporation of CKD into the HSE Chronic Disease Management Programme for primary care may facilitate improved care of patients with CKD in Ireland; – The introduction of medications known to reduce rates of deterioration in kidney function and reduce cardiovascular risk, such as SGLT2 inhibitors, GLP-1 analogues, and non-steroidal mineralocorticoid antagonists where appropriate; – Improve blood pressure control in people with CKD in Ireland based on international guideline targets and aim to manage their additional cardiovascular risk factors.
Prof Colm Henry, Chief Clinical Officer in the HSE, said: “CKD is one of the most common comorbidities amongst the conditions already covered by the Chronic Disease Management Programme. In the advent of new disease-modifying medications, screening for CKD in high-risk groups is of paramount importance, in particular in primary care and opportunistic screening in secondary care. This work will help inform not just our renal service, but also chronic disease and renal transplant programmes.”
Prof George Mellotte, National Clinical Director for Renal Services and Carol Moore, CEO of the Irish Kidney Association, both said the results of the survey should reinforce calls for CKD to be integrated into the HSE National Chronic Disease Management Programme as a crucial step forward in managing the disease, improving patient outcomes, and decreasing healthcare costs.