






Reference: July-August 2025 | Issue 4 | Vol 18 | Page 23
Due to the lack of a clinical care programme, ILD patients are being excluded from community pulmonary rehabilitation and other services
Interstitial lung disease (ILD) describes a group of heterogeneous diseases that are identified by several features such as inflammation and fibrosis of the lung interstitium, of which there are over 200 different types.1 A large subset of patients diagnosed with ILD have pulmonary fibrosis (PF). The most common PF is idiopathic pulmonary fibrosis (IPF), which accounts for around 17-37 per cent of all ILD cases.2
IPF is a chronic progressive disease of unknown aetiology, with potentially enormous impacts on physical and emotional health for patients.3,4 It is characterised by irreversible loss of lung function and typically occurs in older adults.5,6
IPF is a life-limiting lung disease with a median survival rate of three to five years.7 The aetiology of the disease is unknown, but the average age of IPF patients ranges from 65-70 years, with incidence increasing with age, and higher rates seen in males than females.8
In many cases, these patients also require complicated respiratory care, particularly at the end of life.9 Many patients throughout the course of the disease will require supplemental oxygen therapy.10 The incidence of IPF is rising globally in part due to several factors, including an ageing population, increased awareness of IPF, and improved diagnostics.11 The role of the nurse in care provision for this group continues to expand.
Impact of IPF
The main symptoms of IPF are:
- Breathlessness on minimal exertion
- Cough;
- Fatigue;
- Anxiety;
- Depression.10
Until recently, no treatments were available for patients diagnosed with IPF. With the introduction of oral antifibrotic therapy, patients now have options. Despite this, the only treatment known to eradicate the disease entirely is a lung transplant, and this option is not suitable for the majority of IPF patients due to a variety of factors related to the qualifying criteria for lung transplant.12 From my experience with IPF, there is high mortality rates and symptom burdens, which has a significant impact on a patient’s quality of life.
Patient care is developed from evidence and recommendations from organisations including the National Institute for Health and Care Excellence (NICE) guidelines13 and the Irish Thoracic Society (ITS) position statement on IPF.14
These guidelines and statements focus on the importance of the multidisciplinary team (MDT), including doctors, nurses, physiotherapists, and psychologists, in caring for patients with IPF. The ITS position statement also recommends onward referral to the Irish Lung Fibrosis Association (ILFA). This association provides support, education, and advocacy for IPF patients.
The symptom burden for this disease is high. Kalluri et al15 noted the worsening symptoms of IPF (increased breathlessness, cough, and fatigue) are linked to the decline in the health-related quality of life for patients.
Managing IPF
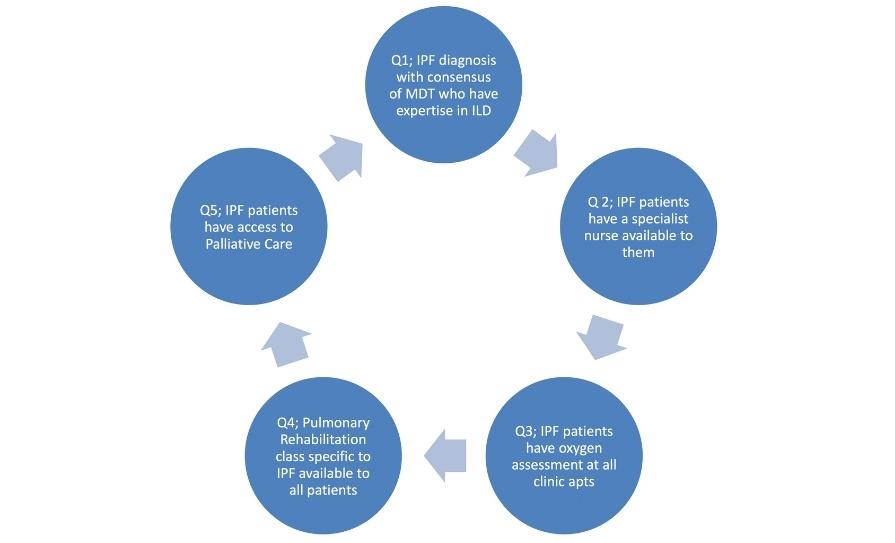
The NICE quality standard for IPF in adults was published in 2015 and has five quality statements, which are illustrated in Figure 1.16 This quality standard highlights the importance of developing a clinical care programme.
The British Thoracic Society (BTS) has a patient registry.17 Their yearly reports are used to assist with establishing a method to review nationwide figures of the disease to create a better understanding of the epidemiology, and in due course, improve patient care.17
The ILD respiratory advanced nurse practitioner (ANP) plays a vital role in the management of ILD, in both in the acute and chronic phase of the disease, providing specialist care to improve patient outcomes. Their expertise extends to patient education, pulmonary rehabilitation, and palliative care, ensuring comprehensive support to both patients and their families/carers.
Pulmonary rehabilitation
Exercise is the cornerstone treatment for chronic diseases and has been shown to improve quality of life.18 Dowman et al noted that pulmonary rehabilitation improves symptoms, health-related quality of life, and functional status in other chronic lung diseases.19
However, ILD patients in Ireland are being excluded from some programmes as the new respiratory integrated care programme is restricted to chronic obstructive pulmonary disease (COPD) and asthma patients.20 In some healthcare settings, resource dependent patients have access to dedicated ILD rehab. Patients are also advised of the ILFA virtual rehabilitation classes. These award-winning classes offer an alternative for some patients.
ILD patients need a national clinical care programme to ensure they have the same access to treatments as other respiratory patients. The ILD respiratory ANP advocates for patients to attend pulmonary rehabilitation, ensuring patients benefit to improve their symptoms.
These benefits include managing their breathlessness and anxiety, which assists with a better quality of life. The ILD respiratory ANP advises patients during clinic consultations on the importance of exercise as part of social prescribing. Patients are signposted to classes suitable for ILD patients, in person and online.
Education
Following on from pulmonary rehabilitation, management of ILD requires a combination of education, physiological assessments, appropriate pharmacological and non-pharmacological care, access to lung transplant assessments, and palliative care. In their scoping review, Bramhill et al21 highlighted the need for adequate information and education to be given at the right time.
The appropriate information is the foundation for the management of all ILD patients. This could also be improved with the introduction of a national clinical care programme.
Education on psychological support is also an important requirement to assist with the impact of this diagnosis on patients and their families. Bramhill22 highlighted how psychological support and education in this area remains an under-resourced service for IPF patients in Ireland.
The ILD respiratory ANP provides education to patients and their family on their IPF diagnosis, treatments (including medication which slows disease progression, such as oral antifibrotics, and pulmonary rehab). Also included in the education sessions is the importance of symptom management and the role palliative care plays in this.
Palliative care in IPF
Palliative care in Ireland was traditionally associated with an oncology diagnosis and end-of-life care. In 2014, palliative care services underwent a major review post a key recommendation from the World Health Organisation and the Worldwide Palliative Care Alliance.
They endorsed the integration of palliative care into relevant national health and disease specific policies.23 This endorsement allowed patients with non-malignant diseases to avail of this supportive, holistic, person-centred approach.
Despite recommendations and endorsements, however, international research has shown mixed access to palliative care, with the majority of patients not receiving optimal palliative input over the course of their disease.24 In 2023, of the 29 patients who died that were linked to the ILD services in my hospital, 68 per cent had been linked to palliative care. This increased in 2024, whereby 80 per cent of deceased patients had been linked into palliative care.
These patients were cared for at home, in hospital, or the hospice at the time of their death. The ANP extends care beyond just the patient, and ensures there is follow-up communication with families of the deceased. Also, a quarterly MDT has been established between palliative care and ILD services in my hospital.
These meetings have notably improved access to ILD and palliative services, and patients have verbalised the benefits. Additionally, as the respiratory ANP for ILD, I have up-skilled and enhanced my knowledge by completing a certificate in palliative care.
Participating in the ILD-palliative MDT and completing the Princess Alice Trust Certificate in Palliative Care has enabled palliative care to be freely discussed in the ILD ANP clinic. This ensures the stigma sometimes associated with being referred to palliative services is avoided, and that patients can express concerns or ask questions in a safe environment.
ANP clinic reflection
To highlight the benefit of a referral to palliative services, a patient attending the ILD ANP clinic for a number of years was referred to her local palliative services for symptom management. The patient had been on ambulatory oxygen therapy (10 litres per minute) for the past three years, and recently commenced two litres per minute at rest. She noticed her breathlessness was interfering with her quality of life.
The patient reluctantly accepted the referral to palliative care. On her return to the ANP clinic three months later, she had a beaming smile. The patient was reviewed by all members of the palliative services available in her county. She was able to have a bath for the first time in three years. She also received other aids and advice that have improved her quality of life. It is amazing to see the improvement and hope the ILD patients can have due to the language used and the suggested changes made in clinic.
Conclusion
The ILD respiratory ANP is an important member of the MDT in caring for patients with this burdensome diagnosis. The importance of exercise cannot be over emphasised for ILD patients. However, due to the lack of a clinical care programme, ILD patients are being excluded from community pulmonary rehabilitation programmes.
The ILD respiratory ANP ensures all patients are educated on its importance, along with other treatment options including medications and palliative care. The ANP also ensures patients understand the role palliative care contributes to symptom management and onwards to end-of-life care. The ILD respiratory ANP is the cornerstone in caring for ILD patients and the patient reflection highlights this.
References
- Salciccioli JD, Marshall DC, Goodall R, et al. Interstitial lung disease incidence and mortality in the UK and the European Union: An observational study, 2001-2017. ERJ Open Res. 2022;8(3):00058-2022.
- Aiello M, Bertorelli G, Bocchino M, et al. The earlier, the better: Impact of early diagnosis on clinical outcome in idiopathic pulmonary fibrosis. Pulm Pharmacol Ther. 2017;44:7-15.
- Lancaster L, Bonella F, Inoue Y, et al. Idiopathic pulmonary fibrosis: Physician and patient perspectives on the pathway to care from symptom recognition to diagnosis and disease burden. Respirology. 2022;27(1):66-75.
- Lee JH, Park HJ, Kim S, et al. Epidemiology and comorbidities in idiopathic pulmonary fibrosis: A nationwide cohort study. BMC Pulm Med. 2023;23:54.
- Maher TM, Molina-Molina M, Russell AM, et al. Unmet needs in the treatment of idiopathic pulmonary fibrosis-insights from patient chart review in five European countries. BMC Pulm Med. 2017;17(1):124.
- Van Manen MJ, Geelhoed JJ, Tak NC, et al. Optimising quality of life in patients with idiopathic pulmonary fibrosis. Ther Adv Respir Dis. 2017;11(3):157-169.
- Kaunisto J, Salomaa ER, Hodgson U, et al. Demographics and survival of patients with idiopathic pulmonary fibrosis in the Finnish IPF registry. ERJ Open Res. 2019;5(3):00170-2018.
- Bajwah S, Yorke J. Palliative care and interstitial lung disease. Curr Opin Support Palliat Care. 2017;11(3):141-146.
- Janssen DJ, McCormick JR. Palliative care and pulmonary rehabilitation. Clin Chest Med. 2014;35(2):411-421.
- Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68.
- Delameillieure A, Dobbels F, Vandekerkhof S, et al. Patients’ and healthcare professionals’ perspectives on the idiopathic pulmonary fibrosis care journey: A qualitative study. BMC Pulm Med. 2021;21(1):93.
- Shaw J, Marshall T, Morris H, et al. Idiopathic pulmonary fibrosis: A holistic approach to disease management in the antifibrotic age. J Thorac Dis. 2017;9(11):4700-4707.
- National Institute for Health and Care Excellence. Idiopathic pulmonary fibrosis in adults: Diagnosis and management. 2017. Available at: www.ncbi.nlm.nih.gov/books/NBK553262/.
- Irish Thoracic Society. Position Statement on the Management of Idiopathic Pulmonary Fibrosis. 2018. Available at: http://irishthoracicsociety.com/wp-content/uploads/2018/08/ITS-Pulmonary-Fibrosis-Position-Statement.pdf.
- Kalluri M, Luppi F, Ferrara G. What patients with idiopathic pulmonary fibrosis and caregivers want: Filling the gaps with patient-reported outcomes and experience measures. Am J Med. 2020;133(3):281-289.
- National Institute for Health and Care Excellence. Idiopathic pulmonary fibrosis in adults.2015. Available at: www.nice.org.uk/guidance/qs79 (Accessed 4th October 2024).
- British Thoracic Society. BTS ILD Registry. 2024. Available at: www.brit-thoracic.org.uk/quality-improvement/bts-ild-registry/.
- Anderson E, Durstine JL. Physical activity, exercise, and chronic diseases: A brief review. Sports Med Health Sci. 2019;1(1):3-10.
- Dowman L, Hill CJ, May A, et al. Pulmonary rehabilitation for interstitial lung disease. Cochrane Database Syst Rev. 2021;2(2):CD006322.
- House of the Oireachtas. Committee on the Future of Healthcare Slaintcare Report. 2017. Available at: https://data.oireachtas.ie/ie/oireachtas/committee/dail/32/committee_on_the_future_of_healthcare/reports/2017/2017-05-30_slaintecare-report_en.pdf.
- Bramhill C, Langan D, Mulryan H, et al. Exploration of the unmet needs of patients diagnosed with idiopathic pulmonary fibrosis: A scoping review protocol. BMJ Open. 2023;13(5):e070513.
- Bramhill C. Pulmonary fibrosis: Unmet healthcare needs. Medical Independent. 2024;4(10) 28-39.
- Mc Veigh C, Reid J, Larkin P, et al. The experience of palliative care service provision for people with non-malignant respiratory disease and their family carers: An all-Ireland qualitative study. J Adv Nurs. 2018;74(2):383-394.
- Chaaban S, McCormick J, Gleason D, et al. Palliative Care for the interstitial lung disease patient a must and not just a need. Am J Hosp Palliat Care. 2022;39(6):710-715.











Leave a Reply
You must be logged in to post a comment.