






Urolithiasis is a common problem in the emergency department, GP office, and urology and nephrology outpatients, with potentially high recurrence rates
Case study
Referral: A 51-year-old male was referred to the urology clinic with an incidental diagnosis of right-sided kidney stones while undergoing an ultrasound gallbladder.
History: The patient reported no history of flank pain, haematuria, dysuria, or other lower urinary tract symptoms. He had never passed a kidney stone, or had a urinary tract infection. He underwent ultrasound abdomen due to intermittent biliary colic, for which he was awaiting follow-up with general surgeons.
His past medical history is significant for reflux, for which he takes a proton-pump inhibitor, and a previous arthroscopy for knee pain. He is a non-smoker with an estimated alcohol intake of 14 units per week. He is an office worker, who goes to the gym twice a week, and plays tennis once weekly. He lives with his partner and two children. He has no family history of stone disease or nephrological illness.
He drinks two coffees per day, has a carbonated drink with lunch, and ‘tries’ to drink a litre of water per day. He maintains that he follows a relatively healthy diet and his family get take-away once per week.
Examination: Normal body mass index, abdominal examination, and external genitalia with a 30cc smooth prostate on digital rectal exam.
Investigations: Urinalysis is normal. Serum creatinine was 83umol/L.
Management: He underwent an XR-KUB and stone profile bloods in urology clinic and was referred for a CT KUB. His CT showed a 1.5cm intra-renal right-sided non-obstructing stone. Following discussion of his management options, he underwent an elective flexible ureterorenoscopy with laser fragmentation of the stone with stent insertion. He was discharged home the same day.
Follow-up: He underwent stent removal two weeks post-operatively. Stone analysis showed a calcium oxalate stone and he was given stone prevention advice. He is due for follow-up in the urology clinic in six months with an x-ray on arrival.
Urolithiasis is the presence of stones/calculi in the urinary tract. The patient in our case study had an asymptomatic kidney/renal stone. Urolithiasis incidence depends on a variety of factors including genetics, diet, ethnicity, and geography. In Western countries the prevalence rate is 10-20 per cent and is increasing.
Pathophysiology and risk factors
Stones form in the urinary tract due to the aggregation of crystals in the urine. This occurs when the volume of solute overcomes the ability of the urine to dissolve it, causing the crystals to aggregate and stones to form. Risk factors are detailed in Table 1.
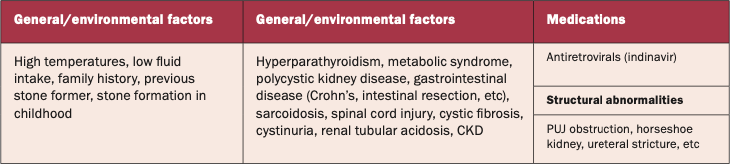
TABLE 1: Risk factors for urolithiasis
Stones are most commonly composed of calcium oxalate (70-80 per cent), a combination of calcium oxalate and phosphate (10 per cent), uric acid, or struvite. Struvite stones (magnesium ammonium phosphate) are associated with recurrent infections due to urease producing bacteria such as proteus, pseudomonas, klebsiella, and staphylococcus. Rarer stone types such as cystine require specialist evaluation as they are associated with cystinuria, a disorder of amino acid transport.
Clinical consequences

FIGURE 1: A representative CT showing intrarenal stones (blue arrows) and a proximal obstructing stone in the left proximal ureter (red arrow)
Stones which form in the kidney (intra-renal stones) can be problematic, or patients can be asymptomatic with stones detected on investigations for other reasons. Our patient had a small asymptomatic stone – the natural history of these is not well defined and the risk of a symptomatic episode or intervention is 10-25 per cent per annum. Intra-renal stones may cause pain, infections or obstruction. A patient may present acutely if a stone passes into the ureter (Figure 1), causing renal colic with or without haematuria, acute kidney injury, or features of urosepsis.
Patient evaluation
History and physical examination
A full history and physical examination should be performed. Pertinent points on history include evaluation of flank pain, symptoms of urinary tract infection, haematuria, as well as a detailed fluid history, medical history, and family history.
Laboratory investigations
In the urology clinic a urine dipstick is performed and a sample sent for microscopy, culture, and sensitivity. Baseline bloods recommended by the European Association of Urology (EAU) guidelines include full blood count, renal profile, bone profile, and C-reactive protein.
Any patient who undergoes intervention should have a stone specimen sent for metabolic evaluation. In recurrent stone formers or patients who are deemed high risk for recurrent stone formation, these patients may undergo detailed metabolic evaluation under the supervision of nephrology. This includes 24-hour urine collection, blood gas analysis, and parathyroid hormone evaluation.
Radiology
A baseline x-ray kidneys, ureters, and bladder (KUB) is frequently performed in the urology outpatients. It carries a sensitivity and specificity of 44-77 per cent, and is easy to perform with low radiation exposure. If the stone is radiopaque, it is useful for follow-up imaging. However, a low-dose non-contrast CT KUB has become the standard for detailed evaluation of renal and ureteric stones as it will identify radio-opaque stones, and gives information on the anatomy and features of the stone such as its density and area. A contrast-enhanced study gives further anatomical details and is helpful when intervention is being planned. Nuclear imaging such as a renogram is usually only performed if there is a concern about reduced kidney function or chronic obstruction – for example; if a kidney is small/atrophic, or in the setting of a staghorn stone.
Management
Stone management depends on the location and size of the stone, patient co-morbidities and anatomy, and patient preferences. ‘Red flags’ necessitating urgent review in the emergency department for patients with confirmed or suspected stones include signs of sepsis, renal colic in a patient with a single kidney, acute kidney injury, and uncontrollable pain. For asymptomatic intra-renal stones, like the one in our case presentation, the management options are conservative treatment, medical treatment, or active removal (Figure 2). The decision on which management approach to be taken is a collaborative one between patient and clinician following discussion of all management options, the benefits, and the risks.
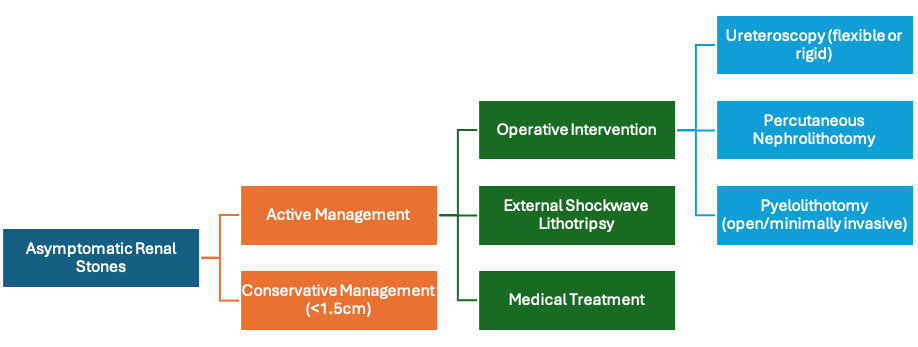
FIGURE 2: Schematic showing treatment options for intra-renal stones
Conservative management
Indication for treatment of intra-renal stones includes stone growth, infection, obstruction, symptoms (pain, haematuria), patient preference, high-risk stone former/recurrent stone former, or for social reasons (eg, pilot). Conservative management is suitable for asymptomatic small intra-renal stones (<1.5cm). Patients are reviewed annually with clinical review, an x-ray KUB, and considered for active management if the stone increases in size, they become symptomatic, or their preferences change. Patients should be informed that studies of patients who have been conservatively managed showed a range of outcomes; symptom development rates of 7-77 per cent and surgical intervention of 7-26 per cent.
Medical management
Medical or pharmacological treatment is useful only in certain stone subtypes such as uric acid stones and in cystine stones. In the setting of acute renal colic due to an ureteric stone, anti-inflammatories (diclofenac, ibuprofen) and alpha blockers (tamsulosin) are helpful for symptom management and to assist stone passage.
Active destruction of stones
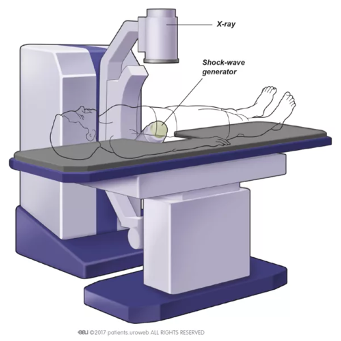
FIGURE 3: Options for active stone management or destruction: A demonstrates ESWL
Finally, there is the active destruction or removal of stones. This can be done using extracorporeal shockwave lithotripsy (ESWL) or surgery (Figure 3A). ESWL is suitable in stones that are <2cm in size. It is usually done with the patient awake and involves using sound waves to fragment the stones, which can then be passed out in the urine. It may require more than one session to fragment the stone.
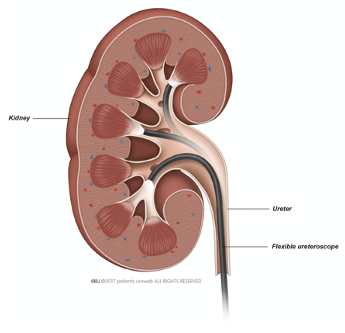
FIGURE 3: Options for active stone management or destruction:
B flexible ureterorenoscopy
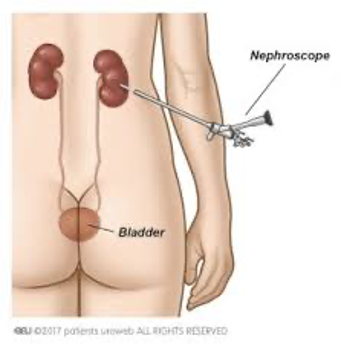
FIGURE 3: Options for active stone management or destruction:
C PCNL All images courtesy of EAU Uroweb
More invasive surgical approaches are usually done by the minimally-invasive endoscopic approach known as ureteroscopy. This involves passing a semi-rigid or flexible scope via the urethra to the ureter and renal pelvis. Through this scope a laser and other instruments can be passed, which allows destruction and extraction of stones (Figure 3B & 4). This can usually be done as a day case procedure under general anaesthesia and is suitable for most stone types. For larger stones, or those in difficult to access calyces, percutaneous nephrolithotomy (PCNL) may be advised (Figure 3C). During PCNL a tract is created via the patient’s flank to allow passage of a scope directly into the kidney. Both PCNL and ureteroscopy are considered safe and effective procedures for the management of stones with excellent outcomes. In the era of minimally-invasive endourology the need for open surgery for the management of intra-renal stones has become rare.
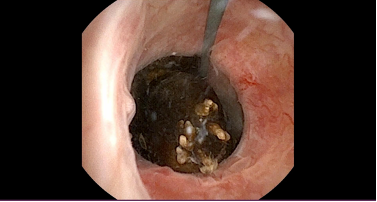
FIGURE 4: Image of a stone in the ureter on ureteroscopy
Stent symptoms
Following ureteroscopy or PCNL, patients may have a ureteric stent inserted as a temporary measure. Stents usually consist of PTFE or silicone and sit completely internally, from renal pelvis to bladder. Stent-related symptoms are well recognised, with 78 per cent of patients complaining of bothersome urinary symptoms including frequency, haematuria and urgency. Up to 80 per cent of patients may also complain of flank pain or suprapubic discomfort. Alpha blockers (tamsulosin 400mcg OD) may improve stent-related symptoms.
Stone prevention
All patients should be given advice about stone prevention. The British Association of Urological Surgeons information leaflets provide a useful adjunct to oral advice given in the outpatient department. It is recommended to drink 2.5-3 litres of fluid per day, preferably water, with an aim of urine output of 2-2.5 litres per day. Advice should be given to increase fluid intake with warm weather or exercise so as to balance fluid losses. Caffeine, alcohol, and carbonated drinks should be reduced. Other dietary advice includes limiting NaCl content to 4-5g/day, and animal protein to 0.8-1.0g/day.
It is important not to reduce calcium intake, as reduced dietary calcium causes an increase in urinary oxalate which can precipitate stone formation.
Long-term follow-up
Approximately 26 per cent of first-time stone formers will have further stones within five years. This rate is higher in those patients who are recurrent stone formers, and in those with underlying metabolic abnormalities. The EAU guidelines recommend that patients who are stone free after treatment should be followed up for a minimum of two years following treatment. X-ray is suitable if stones are radio-opaque, but ultrasound may be required in radiolucent stones. This gives a safety margin of approximately 80 per cent. In metabolic stone formers or those with residual fragments, a more prolonged follow-up is required.
Conclusion
Urolithiasis is a common problem in the emergency department, GP office, and the urology and nephrology outpatients. Patients with renal stones may be unaware of their presence, or suffer with significant problems including urosepsis and kidney injury.
Management options depend on a variety of patient and stone factors, but all decisions regarding management should be made in a collaborative fashion. Treatment options include observation, analgesia, stone dissolution, ESWL and minimally-invasive endoscopic interventions.
Stones recur in up to 26 per cent of first-time stone formers within five years. Key in the prevention of stone recurrence is lifestyle modification, particularly fluid intake and dietary adjustments. Where necessary, more detailed metabolic evaluation and referral to specialist services can be required.
References available on request
Author: Ms Sorcha O’Meara, Urology Specialist Registrar in Blackrock Clinic Dublin; and Prof Niall F Davis, Consultant Urologist, Beaumont Hospital, Dublin; and Senior Lecturer, RCSI











Leave a Reply
You must be logged in to post a comment.