






Platelet-rich plasma holds significant potential for enhancing recovery and rehabilitation of athletes, ultimately contributing to improved outcomes in the field of sports medicine
The positive impact sport has on health is well recognised. However, each spring sees the inevitable rise in presentations of, often preventable, sports injuries in the primary care clinic or on a physiotherapist’s table.
The incidence of injury in sports has increased in recent years due to a rise in participation, poor injury prevention strategies, and faulty or inadequate training. In fact, the prevalence of injury was highlighted in a 12-month, prospective study carried out on 324 Irish athletes involved at a high level of sports participation in one of the following categories: endurance, contact, non-contact, or explosive sports. The findings show that a significant portion of athletes (40 per cent) suffer an injury within a year. The average athlete sustains around 1.17 acute and 0.93 overuse injuries per year, leading to an average of 52 days of lost time due to injury.
The most common injuries include lumbar muscle strains, ankle sprains, and bone fractures. Not surprisingly, contact sports tend to have higher acute injury rates compared to non-contact sports. Key factors associated with higher injury rates include increased training hours, inadequate facilities, and inappropriate training loads. The younger athlete is at greater risk mainly due to limited knowledge to avoid injury. For the professional athlete these factors can inadvertently shorten their career, and have significant implications in their quality-of-life.
For most people, individual musculoskeletal injuries (MSK) in sports are a consequence of chronic misuse or overuse. Many of these problems can be treated conservatively with rest, non-steroidal anti-inflammatory drugs (NSAIDs), physiotherapy and rehabilitation. Unfortunately, some individuals do not respond well to rehabilitation and formal intervention.
Pathology of MSK injuries
In practising athletes, tendons and the entheses (where tendons attach to bone) experience higher biomechanical stress compared to non-athletes, due to the repetitive and intense nature of athletic activities. These activities may also affect the muscle, cartilage, and place bone under chronic stress.
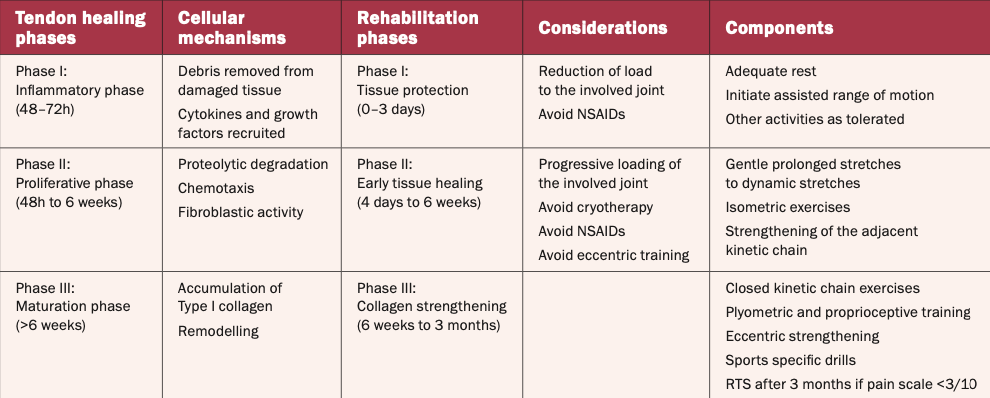
The underlying pathology in persistent cases of MSK injury can be related to irreversible microstructural changes in connective tissue that have failed to recover and adapt to rehabilitation. Typically, recovering from any injury is regarded as a three-phase process, as outlined in Table 1.
These problems do not have an effective treatment modality, and this is the grey area where orthopaedic surgeons and sports physicians are now attempting to employ biological therapy to hasten repair and, thereby, bring about recovery.
In regenerative medicine, which is a growing therapy globally, procedures like platelet-rich plasma (PRP) injections have shown promise. From a clinical perspective, regenerative sports medicine focuses on injuries related to sports activities and ageing, involving various components of the MSK system such as menisci, ligaments, tendons, cartilage, and bones. PRP has shown its utility as an interventional therapy for sports injuries in specific cases.
Emergence of PRP
The concept of using the body’s own inherent healing mechanism to assist in repair, and to potentially replace or restore damaged tissue through the use of autologous or allogenic biologics, has always been considered a possibility. In the clinical setting, the use of PRP began as early as the 1980s when it was found to be effective in treating blood loss during cardiac surgery. Its effect on bone was then examined in the field of dentistry for its regenerative properties on bone maturation and formation. In time, its use in MSK medicine has grown, and a role in tendon and tissue healing has been heavily investigated. Over the last 10 years there has been an increase in the use of PRP among medical clinicians, especially for its potential in treating tendinopathy and degenerative cellular diseases.
Within the specialty of pain management, the use of regenerative medicine is a relatively new treatment option. PRP contains numerous growth factors and cytokines that potentially offer an alternative treatment modality to assist in the healing of multiple MSK issues. The use of PRP is expanding exponentially, creating new frontiers for the treatment of MSK and spinal pain.
One reason for the growth in interest in PRP is because, according to World Anti-doping Agency regulations, PRP is not prohibited. Although individual growth factors are still prohibited when given separately as purified substances. PRP therapy is only prohibited if it offers performance-enhancing effects, or if the PRP was altered in a way that can produce performance-enhancing benefits.
Why does PRP work?
In the early phase of any injury the inflammatory phase predominates. Ice, rest, activity modification, and anti-inflammatory medications are generally included in the current mode of management. Many injuries settle but, in some cases, local steroid injections are required. While steroids are the gold standard to reduce inflammation, they do little to directly promote the healing phase. Occasionally, even steroids fail to resolve the symptoms, leaving the individual with a long uphill battle to recovery.
This is fundamentally where PRP therapy has an important role. PRP seeks to recruit and enhance the body’s own inherent healing mechanism to assist in repair, and to potentially replace or restore damaged tissue. PRP therapy can increase the rate of MSK healing by stimulating angiogenesis, cell proliferation, and chemotaxis. It has been demonstrated that PRP promotes healing in cases of tendinous, ligamentous injury and muscular strain. Thus, PRP has been utilised for the purpose of shortening the recovery period, and it has helped improve the recovery time of athletes.
How is PRP prepared?
Generally, the preparation of PRP involves obtaining autologous whole blood from the patient followed by a centrifugation process to separate plasma from red blood cells and leukocytes (Figure 1). The method of isolation plays a role in the final concentration of platelets and leukocytes in the PRP preparation. What was once a complex ‘event’ has been simplified into a three-step process.
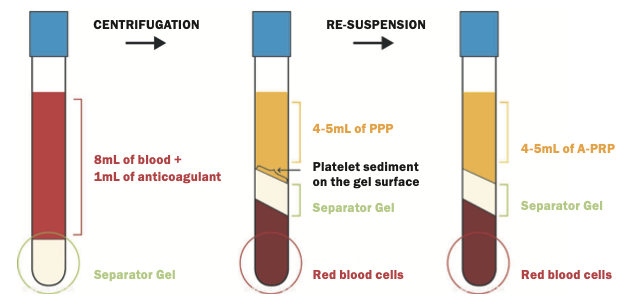
1. Withdraw a blood sample in a specific collecting tube.
2. Centrifuge the sample to separate the plasma which is rich in several growth factors.
3. Reinjection of the product at the injury site. This is best undertaken using image guidance such as ultrasound or fluoroscopy to improve accuracy.
This preparation process, and the injection of the PRP, can be completed in a matter of minutes, using simple clinical equipment, and delivered safely to the affected site. Ultrasound guidance is preferable to increase the accuracy and improve treatment outcome.
What does PRP contain?
Platelets, which are one of the main components in PRP, help mediate the release of several growth factors that are essential in the healing process. These include platelet-derived growth factor, transforming growth factor, fibroblast growth factor, vascular endothelial growth factor, epidermal growth factor and insulin-like growth factor. These growth factors are essential for the three phases of healing: Inflammation, proliferation, and remodelling.
The proposed benefit of PRP is that it allows for the patient’s own blood to provide a high concentration of growth factors to promote healing at injury sites that have limited healing capacity due to blood supply. This matrix serves as a scaffold for sustained release of growth factors that drive chemotaxis and angiogenesis.
There are several basic science studies to support the use of PRP for tendon and ligament healing in the in vivo setting. PRP has been shown to:
a) Induce tendon cell proliferation along with induction of angiogenic factors.
b) Have anabolic effects on tendon cells by increasing the total collagen synthesis in tenocytes. Collagen type I seems to be promoted by PRP and may help limit the development of fibrotic tissue. There is an important ratio between different types of collagen and a balance seems necessary to avoid increased fibrosis and reduced strength of a tendon.
What is the clinical evidence to support PRP?
The evidence in the literature reflects the greater use of the technique globally.
a) Lateral epicondylitis
Also known as tennis elbow, lateral epicondylitis has shown very favourable results when treated with PRP compared to traditional steroid injections. In a meta-analysis of randomised controlled trials (RCTs) examining the use of PRP, it was reported that PRP was significantly more effective at reducing pain intensity compared to various controls in both short-term (<6.5 months) and long-term (>one year) follow-up periods.
In 2017, a study was undertaken to compare outcomes between a single PRP injection and surgery for patients suffering from lateral elbow tendinopathy. It appears that both can provide at least similar pain relief in the first 12 months, but after two years arthroscopy was superior to PRP in terms of long-term pain and functional outcomes. Nevertheless, for some individuals, a 15-minute bedside procedure annually may be the preferred option.
b) Rotator cuff tendinopathy
The use of PRP in rotator cuff pathology has come with mixed results in the literature. Early studies on augmenting rotator cuff repair with PRP have been inconsistent with regard to clinical outcomes. A more recent meta-analysis by Hurley et al examined over 18 randomised controlled studies comparing PRP to arthroscopic repair alone. Their study included over 1,147 patients and found that those treated with PRP had significantly decreased rates of incomplete tendon healing for small-medium and medium-complete tears. They also found a significant decrease in visual analogue scores (VAS pain score) at 30 days and final follow-up compared to the control group.
c) Patellar tendinopathy
Patellar tendinopathy, otherwise known as jumper’s knee, is characterised by chronic pain as a result of overuse. The clinical evidence suggests that PRP can improve pain and function, with up to 22-81 per cent of patients able to return to their pre-symptom level of activity.
The number of PRP injections has also been shown to have an effect on the outcome of the treatment, with two injections found to improve outcomes significantly more than a singular injection.
d) Achilles tendinopathy
The Achilles tendon is a conjoined structure composed of the tendinous regions of the superficial posterior compartment musculature. The tendon resists forces up to 12 times body weight during exercise and is among the strongest in the body. Despite its robust structure, it is also among the most frequently ruptured tendons in the lower extremity, and accounts for 20 per cent of major tendon injuries.
Due to increased sports competitiveness, an ageing population and rising obesity rates, the incidence of Achilles tendon rupture is on the rise. The majority of severe Achilles tendon injuries occur as a result of sports activities, and professional athletes are thus more prone to Achilles tendon injury. Approximately 30-50 of 100 sports-related injuries involve tendon issues. Sports such as jogging, badminton, squash, or training in sub-zero weather put individuals at higher risk of an Achilles tendon injury.
Due to its relative non-invasiveness and minimal risk, PRP injections are being investigated with hopes of improving tendinopathy outcomes. Unfortunately, the initial results are not very encouraging.
e) Ulnar collateral ligament injury
Injury to the medial ulnar collateral ligament (MUCL) occurs as a result of extraneous valgus loads and is common in overhead-throwing athletes. A fully torn ligament or one that has not responded favourably to conservative treatment will be treated surgically; however, success rates have varied from 83-to-90 per cent for a return to the sports field within nine–12 months post-surgery. A case study by Hoffman et al detailed the outcome of an MUCL reconstruction in a 25-year-old professional baseball pitcher that was augmented with a dermal allograft reconstituted in PRP and mesenchymal stem cells. The authors found that their patient was able to return to pitching by four months post-op.
Despite various case reports, there are no available RCTs examining the effectiveness of PRP in MUCL injuries and it is still unclear whether PRP expedites return to play in conservative management.
f) Anterior cruciate ligament
The anterior cruciate ligament (ACL) is vital to the stability of the knee and its rupture requires surgical intervention to restore this functionality. A systematic review by Figueroa et al regarding ACL repair with the aid of PRP showed variable results in terms of clinical outcomes, bone tunnel healing/widening, and graft maturation.
The use of PRP may show more promise in partial tears. A systematic review by Di Matteo et al included two studies of PRP used for partial ACL tears, which showed that between 70-to-84 per cent of patients return to previous level of activity without surgery. Initial research regarding the use of PRP to treat ACL injuries shows promise in terms of its ability to help induce cell growth for various grafts; however, there is not sufficient research to conclude the best composition of PRP injections to induce the maximal amount of healing.
g) Other options
With the ease of preparation, improved ultrasound accessibility, and a growing awareness in the medical community, the probability is that different tendons and ligaments are going to be injected. For refractory cases such as gluteal tendonitis, ankle ligament, and hand injury, PRP therapy will continue to open up simple treatment options for more individuals. The initial feedback is very encouraging both in terms of pain reduction and improved functional capacity. Capturing this data in a form that can be shared to advance the treatment is a challenge.
While regenerative PRP management can be provided independently, it should be provided in conjunction with other modalities of treatment including a structured exercise programme, physical therapy, behavioural therapy, and appropriate conventional medical therapy as necessary. Appropriate precautions should be taken into consideration and followed prior to performing biologic therapy.
Conclusion
In conclusion, PRP has shown great promise as a treatment modality for sports injuries. Its regenerative properties and ability to promote tissue healing have made it a very valuable option for conditions such as tendon and ligament injuries commonly encountered in sports. PRP has demonstrated effectiveness in treating specific sports-related conditions like tennis elbow, jumper’s knee, and runner’s knee. Further research is needed to optimise PRP protocols and understand the mechanism of action in sports injury, but it is already clear that it holds significant potential for enhancing recovery and rehabilitation of athletes, ultimately contributing to improved outcomes in the field of sports medicine.
Disclosure
Prof Hegarty does not receive reimbursement from any specific company to use or promote the technique or products mentioned in this article.
References
1. American Society of Interventional Pain Physicians: Responsible, safe, and effective use of biologics in the management of low back pain: American Society of Interventional Pain Physicians (ASIPP) Guidelines. Pain Physician. 2019 Jan;22(1S):S1-S74
2. Kia C, Baldino J, Bell R, Ramji A, Uyeki C, Mazzocca A. Platelet-rich plasma: Review of current literature on its use for tendon and ligament pathology. Curr Rev Musculoskelet Med. 2018 Dec;11(4):566-572
3. DelRossi AJ, Cernaianu AC, Vertrees RA, et al. Platelet-rich plasma reduces postoperative blood loss after cardiopulmonary bypass. J Thorac Cardiovasc Surg. 1990;100(2):281–6
4. Ferrari M, Zia S, Valbonesi M, Henriquet F, Venere G, Spagnolo S, et al. A new technique for haemodilution, preparation of autologous platelet-rich plasma, and intraoperative blood salvage in cardiac surgery. Int J Artif Organs. 1987;10(1):47–50
5. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(6):638–46
6. Anitua E. Plasma rich in growth factors: Preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants. 1999;14(4):529–35
7. Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: An evidence-based approach. PM R. 2011;3(3):226–50
8. Mazzocca AD, McCarthy MB, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94:308–16.
9. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: From basic science to clinical applications. Am J Sports Med. 2009;37:2259–72
10. Malanga GA, Goldin M. PRP: Review of the current evidence of musculoskeletal conditions. Curr Phys Med Rehab. 2014;2(1):1–15
11. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16:585–601
12. Scherer SS, Tobalem M, Vigato E, et al. Nonactivated versus thrombin-activated platelets on wound healing and fibroblast- myofibroblast differentiation in vivo and in vitro. Plas Reconstr Surg. 2012;129(1):46e–54e
13. Geaney LE, Arciero RA, DeBarradino TM, Mazzocca AD. The effects of platelet-rich plasma on tendon and ligament: Basic science and clinical application. Oper Tech Sports Med. 2011;19(3):160–4
14. Anitua E, Andia I, Sanchez M, et al. Autologous preparations rich in growth factors promote proliferation and induce VEGF and HGF production by human tendon cells in culture. J Orthop Res. 2005;23:281–6
15. Chen L, Dong SW, Tao X, Liu JP, Tang KL, Xu JZ. Autologous platelet-rich clot releasate stimulates proliferation and inhibits differentiation of adult rat tendon stem cells towards nontenocyte lineages. J Int Med Res. 2012;40(4):1399–409
16. Zhang J, Wang JH. Platelet-rich plasma releasate promotes differentiation of tendon stem cells into active tenocytes. AJSM. 2010;38(12):2477–86
17. McCarrel T, Fortier L. Temporal growth factor release from platelet-rich plasma, trehalose lyophilised platelets, and bone marrow aspirate and their effect on tendon and ligament gene expression. J Orthop Res. 2009;27(8):1033–42
18. Zhou Y, Wang J. PRP treatment efficacy for tendinopathy: A review of basic science studies. Biomed Res Int. 2016;2016:1–8
19. Madry H, Kohn D, Cucchiarini M. Direct FGF-2 gene transfer via recombinant adeno-associated virus vectors stimulates cell proliferation, collagen production, and the repair of experimental lesions in the human ACL. Am J Sports Med. 2013;41:194–202
20. Marui T, Niyibizi C, Georgescu HI, Cao M, Kavalkovich KW, Levine RE, et al. Effect of growth factors on matrix synthesis by ligament fibroblasts. J Orthop Res. 1997;15:18–23
21. Unlu M, Kivrak A, Kayaalp ME, Birsel O, Akgun I. Peritendinous injection of platelet-rich plasma to treat tendinopathy: A retrospective review. Acta Orthop Traumatol Turc. 2017 Dec;51(6):482–487
22. Chen X, Jones IA, Park C, Vangsness CT. The efficacy of platelet-rich plasma on tendon and ligament healing: A systematic review and meta-analysis with bias assessment. Am J Sports Med. 2018 Jul;46(8):2020–32
23. Merolla G, Dellabiancia F, Ricci A, Mussoni MP, Nucci S, Zanoli G, et al. Arthroscopic debridement versus platelet-rich plasma injection: A prospective, randomised, comparative study of chronic lateral epicondylitis with a nearly two-year follow-up. Arthroscopy. 2017 Jul;33(7):1320–1329
24. Hak A, Rajaratnam K, Ayeni OR, Moro J, Peterson D, Sprague S, et al. A double-blinded placebo randomised controlled trial evaluating short-term efficacy of platelet-rich plasma in reducing postop- erative pain after arthroscopic rotator cuff repair: A pilot study. Sports Health. 2015;7(1):58–66
25. Zhao JG, Zhao L, Jiang YX, Wang ZL, Wang J, Zhang P. Platelet- rich plasma in arthroscopic rotator cuff repair: A meta- analysis of randomised controlled trials. Arthroscopy. 2015 Jan;31(1):125–35
26. Hurley ET, Lim Fat D, Moran CJ, Mullett H. The efficacy of platelet-rich plasma and platelet-rich fibrin in arthroscopic rotator cuff repair: A meta-analysis of randomised controlled trials. Am J Sports Med. 2019 Mar;47(3):753–761
27. Liddle AD, Rodríguez-Merchán C. Platelet-rich plasma in the treatment of patellar tendinopathy: A systematic review. Am J Sports Med. 2015;Oct: 43(10):2583–90
28. Gosens T, Den Oudsten BL, et al. Pain and activity levels before and after platelet-rich plasma injection treatment of patellar tendinopathy: A prospective cohort study and the influence of pre- vious treatments. Int Orthop. 2012;36(9):1941–6
29. Andriolo L, Sante Altamura SA, et al. Nonsurgical treatments of patellar tendinopathy: Multiple injections of platelet-rich plasma are a suitable option: A systematic review and meta-analysis. Am J Sports Med. 2019 Mar;47(4):1001-1018
30. Dayton P. Anatomic, vascular, and mechanical overview of the Achilles tendon. Clin Podiatr Med Surg. 2017;34(2):107–13
31. Benjamin M, Toumi H, Ralphs JR, Bydder G, Best TM, Milz S. Where tendons and ligaments meet bone: Attachment sites (‘entheses’) in relation to exercise and/or mechanical load. J Anat. 2006;208(4):471–90
32. Di Matteo B, Kon GFE. Platelet-rich plasma: Evidence for the treatment of patellar and Achilles tendinopathy — a systematic review. Musculoskelet Surg. 2015;99(1):1–9
33. Clark NJ, Desai VS, Dines JD, Morrey ME, Camp CL. Nonreconstruction options for treating medial ulnar collateral ligament injuries of the elbow in overhead athletes. Curr Rev Musculoskelet Med. 2018 Mar;11(1):48–54
34. Podesta L, Crow SA, Volkmer D, Bert T, Yocum LA. Treatment of partial ulnar collateral ligament tears in the elbow with platelet-rich plasma. Am J Sports Med. 2013;41(7):1689–94
35. Figueroa D, Figueroa F, Calvo R, Vaisman A, Ahumada X, Arellano S. Platelet-rich plasma use in anterior cruciate ligament surgery: Systematic review of the literature. J of Arth and Rel Surg. 2015;31(5):981–8
36. Di Matteo B, Loibl M, Andriolo L, et al. Biologic agents for anterior cruciate ligament healing: A systematic review. World J of Orthop. 2016;7(9):592–603
37. WADA regulations. Available at: www.usada.org/spirit-of-sport/orthobiologics-athletes-need-know-prp/
38. Anjanavanna MM, Perumal S, Alwar T, et al. Platelet‑rich plasma (PRP) injection in sports injuries. Indian Journal of Orthopaedics. 2021;55:484–491
39. Patil P, Jadhav M, Suvvari TK, Thomas V. Therapeutic uses of platelet-rich plasma (PRP) in sport injuries – A narrative review. J Orthop Rep. 2024 June;3(2):100287











Leave a Reply
You must be logged in to post a comment.