NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Obesity is described by the HSE as a chronic, complex, and progressive neuroendocrine disease, and is defined as abnormal or excessive adiposity that impairs health. It is reportedly the fastest growing disease globally, placing a massive burden on worldwide healthcare systems. General practice is the ideal setting for identifying and treating obesity, as it encompasses patient-centred care across the lifespan of the patient, and is often described as care “from the cradle to the grave”.
Background
I joined general practice from acute and interventional cardiology in 2019 and work as an advanced nurse practitioner (ANP). I previously completed a masters in preventive cardiology and have a focus on the preventative side of health as there is such a need for this in all aspects of life. I realised that there was fantastic software to keep records and data in general practice, however, after completing an audit, I noted that weight, height, and BMI were generally not recorded for patients. This triggered a subsequent inhouse audit and a change in local policy that all patients would have demographics recorded as part of their vital signs.
Identifying patients for review
All nursing staff aligned, which included an ANP, a general practice nurse (GPN), and a phlebotomy/medical assistant, making every contact count. Every patient that attended for review or annual bloods had their height, weight, and waist circumference recorded. Once a patient was identified as obese or having a BMI that was not within healthy range, they were coded for early intervention and booked in for a visit with the ANP. We recognise that the disease of obesity is not defined by anthropological measurements alone, therefore, we also utilised a Canadian staging tool – the Edmonton staging system – for a holistic assessment which considers physical, psychological, and metabolic parameters – to determine optimal obesity treatment.
Once patients were booked in for review, it became evident that most of them were happy to be identified and to discuss their disease of obesity. These were patients living with obesity that had never before been acknowledged, with many not realising that their obesity was a disease and instead carried the burden of thinking it was somehow self-inflicted. A lot of these patients had no weight recorded on their electronic health record and had never heard from their healthcare professional that they were obese. Some of the patients also perceived a stigma associated with their weight, many of whom reported being told to “eat less, move more”, which was the primary framework and approach to overweight and obesity until recent years.
In 2021, when medications became available for people living with obesity without diabetes, it was a game changer. We now had a tool in our arsenal that could significantly improve outcomes and wellbeing for this patient group. In response to Ireland’s National Obesity Policy Plan, which was launched in 2016 and aligns with the National Framework for the Integrated Prevention and Management of Chronic Disease in Ireland, I attained SCOPE certification – an internationally recognised standard of obesity management expertise – and we launched our obesity management clinic.
Results from a nurse-led obesity management clinic
Once the patient is identified, they are invited in for a consultation, where full anthropological measurements and vital signs are obtained. We discuss the disease of obesity and its impact on their life, as well as dietary and lifestyle modifications, previous weight loss journeys, and medications. I ensure the patients are aware that obesity is a disease and not their fault, ensuring they understand it is the condition of obesity that makes them over eat and not the over-eating that causes obesity.
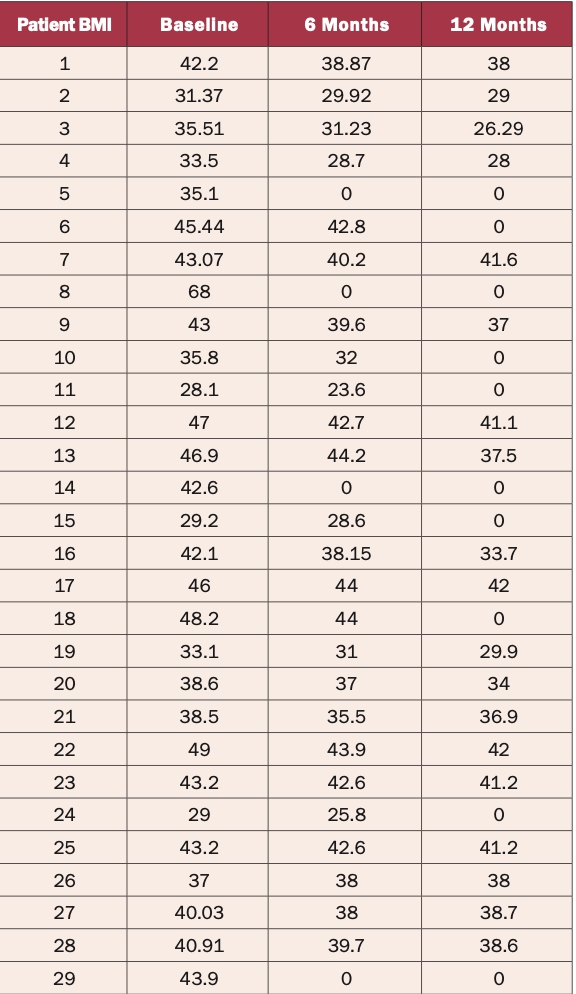
Table 1: BMI values of obese patients at six and 12 months
I also introduce the concept of medications during consultations and educate on the mechanisms of action. It is important to ensure the patient understands that all chronic diseases are treated with medications to keep them under control, and that obesity is no different. The medications are available, and they regulate the hunger and satiety hormones, quietening the hunger voices. The medications, in conjunction with healthy lifestyle choices, treating the disease of obesity and co-morbidities such as pre-diabetes, metabolic syndrome, infertility, and cardiovascular disease (CVD), are showing favourable results.
An in-house audit of patients in our clinic without diabetes on glucagon-like peptide (GLP)-1 medications for obesity management from 2021-to-present was undertaken. The demographics audited included patients that continued on the medication and included:
Effects on hypertension;
Effects on wellbeing;
Reduced BMI;
Cardiovascular benefits.
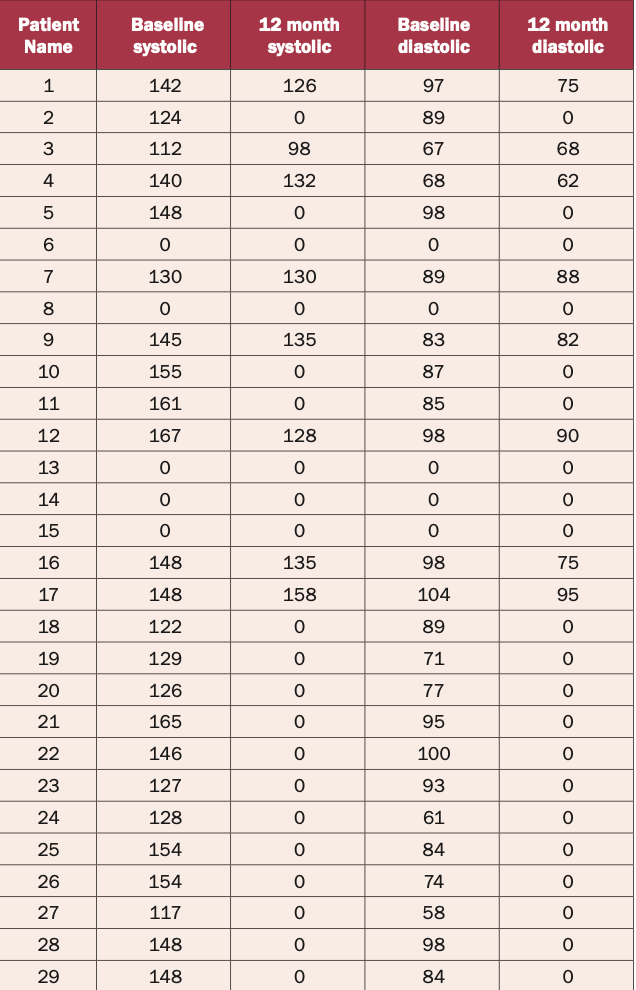
The results are positive and reflect a reduction in BMI, an improvement in wellbeing, and a reduction in CVD risk, including hypertension and lipid profile. Results are outlined in Tables 1-2. A numerical value of zero has been allocated where data was unavailable.
Table 2: Blood pressure values of obese patients at six and 12 months
Conclusion
While these are positive and promising results, like all chronic diseases, obesity requires life-long therapy and currently these medications are very expensive. There is a reimbursement pathway for liraglutide, but it has a very rigid criteria that not all patients fit into. The patient must have a BMI above 35 with CVD risk factors such as hypertension or hypercholesteraemia, be on medications, plus present with both impaired fasting glucose and elevated glycated haemoglobin.
There are a range of new therapies on the market, however, not all are available, reimbursable, or licensed for this patient cohort in Ireland at this time, which is frustrating. For now, we work with what we have, and there is a lot more hope for the future. For patients not responding to existing treatment or requiring bariatric services, we work closely with our colleagues in speciality care. We are also lucky to have a collaborative ANP contact in Loughlinstown, Co Dublin, and Galway to discuss cases with, and refer on, when outside our capacity to treat appropriately. However, for the majority of patients, nurse-led clinics in general practice are the ideal setting for managing their chronic disease.












Leave a Reply
You must be logged in to post a comment.