






Reference: May 2026 | Issue 5 | Vol 12 | Page 38
At the recent Primary Care Dermatology Society of Ireland meeting, which took place from 5-7 March, 2026, in Naas, Co Kildare, Dr Cathal O’Connor, Consultant Dermatologist and dual-trained Consultant Paediatrician, delivered two highly practical presentations on neonatal and infantile dermatology, focusing on common pitfalls, time-sensitive diagnoses, and lesions that should trigger early dermatology referral.
His central message was clear: While many neonatal eruptions and birthmarks are benign and self-limiting, a smaller group are clinically important because they signal infection, systemic disease, developmental syndromes, or a narrow therapeutic window in which intervention can prevent permanent morbidity.
For GPs and hospital doctors in Ireland, the talks offered a useful framework for approaching skin disease in early life. Dr O’Connor divided the subject into two broad settings:
- Neonatal and postnatal ward dermatology, where the main task is distinguishing benign transient rashes from infection or serious genodermatoses and reviewing pigmented lesions and sebaceous naevi
- Outpatient infantile dermatology, where problems such as infantile haemangiomas (IHs), atopic dermatitis, and nappy dermatitis are more likely to present. Across both settings, he repeatedly emphasised the importance of timing, morphology, and correct referral pathways, particularly referral to dermatology rather than general paediatrics for skin-led disease.
Benign neonatal eruptions: Common, dramatic, and frequently overcalled
A major theme in the neonatal lecture was that many newborn eruptions look alarming but are entirely benign. Recognising these patterns can prevent unnecessary sepsis workups, emergency department referrals, and parental anxiety.
Erythema toxicum neonatorum was highlighted as the archetypal example. Despite its alarming name, it is a benign eruption affecting around half of term infants and is uncommon in preterm babies. It typically appears at 24-48 hours after birth in a well baby, with blotchy erythematous macules and papules or pustules, usually on the face, trunk, and limbs, while palms and soles are spared. Lesions wax and wane, and individual lesions are short-lived.
The practical message is that a well infant with classic erythema toxicum does not require septic investigation; parents can be reassured that it resolves spontaneously, usually within two weeks, though recurrence around six weeks may occur.
Transient neonatal pustular melanosis was another important benign mimic, especially in darker-skinned infants. Unlike erythema toxicum, it is present at birth. The pustules rupture easily, leaving hyperpigmented macules with a collarette of scale. Recognition of this sequence is useful, particularly where the pustular stage has already passed and the infant presents only with residual pigmented lesions.
Dr O’Connor also reviewed miliaria, caused by sweat duct obstruction, often in the context of overheating or occlusive clothing. Miliaria crystallina produces tiny superficial vesicles, whereas miliaria rubra or pustulosa produces inflamed papules or pustules. Again, the diagnosis is clinical and management is conservative.
Other reassuring newborn findings included milia, often on the nose, palate or gingivae, and sucking blisters, usually solitary blisters or erosions on the lip, hand or wrist due to vigorous sucking in utero
or after birth. These should not be mistaken for herpes or inherited blistering disease in the absence of other features.
The lecture also covered vascular reactivity phenomena, including harlequin colour change and cutis marmorata. These are physiological in many infants, but Dr O’Connor reminded the audience that fixed, persistent marbling from birth should raise the possibility of cutis marmorata telangiectatica congenita, which may be associated with other anomalies.
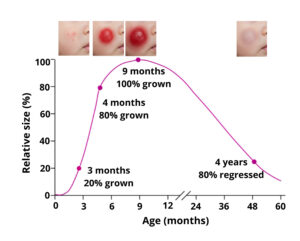
FIGURE 1: IH stabilises between roughly nine and 18 months
IH: Time sensitivity is everything
The vascular birthmarks presentation centred on IH, and the dominant teaching point was that these lesions are time-sensitive. Dr O’Connor strongly advised abandoning outdated terms such as “strawberry”, “capillary”, or “cavernous” haemangioma.
IH is a benign vascular tumour with a characteristic natural history. It is usually not present as a formed haemangioma at birth, though there may be a flat precursor lesion. It develops in the first two to six weeks of life and grows rapidly, with around 80 per cent of growth completed by four months. IH stabilises between roughly nine and 18 months; and involutes gradually over years (Figure 1).
This timeline has major implications for general practice. The two to six week window is “prime GP check time”, and delayed referral means missing the period when treatment is most effective at preventing disfigurement, ulceration or functional compromise, attendees heard.
Dr O’Connor repeatedly emphasised early referral to dermatology. He classified IH by morphology in ways that matter clinically: Superficial vs deep, focal vs segmental, and single vs multiple. Premature infants, he noted, are more likely to have superficial lesions with abrupt stepped borders and thicker superficial components, and are more likely to be referred late despite being at increased risk of permanent cutaneous sequelae.

FIGURE 2: IH develops in various sites and patterns
Which haemangiomas need urgent review?
Not every IH needs treatment, and one of the strengths of the talk was its focus on triage. The question Dr O’Connor suggested clinicians ask was: “Would I want my baby to get propranolol for this haemangioma?” If the answer might be yes, referral should be urgent.
Particular sites and patterns matter (Figure 2):
- Periocular haemangiomas risk occlusion, astigmatism, amblyopia,
and even vision loss - Nasal and auricular lesions have major cosmetic implications and can leave permanent contour deformity
- Lip and perioral lesions can interfere with feeding and ulcerate painfully
- Beard-distribution haemangiomas raise concern for airway involvement; stridor should trigger urgent ENT (ears, nose, throat) review and consideration of laryngobronchoscopy
- Breast-area haemangiomas in girls may affect future breast development
- Ulcerated haemangiomas need urgent dermatology review, meticulous wound care, and cautious use of propranolol
- Five or more cutaneous IHs should prompt liver ultrasound because of the association with hepatic haemangiomatosis and, rarely, high-output cardiac failure.
Segmental lesions also raise syndromic concerns. Large segmental facial haemangiomas may indicate PHACE(S) syndrome – posterior fossa malformations, haemangioma, arterial anomalies, cardiac defects, eye anomalies, and sternal defects/supraumbilical raphe.
Dr O’Connor cautioned that not every facial haemangioma is PHACE(S) syndrome, but lesions in a segmental facial distribution need dermatology review and, where appropriate, echocardiography, electrocardiogram, magnetic resonance angiography, and multidisciplinary assessment.
Similarly, segmental lumbosacral or anogenital haemangiomas may be associated with LUMBAR syndrome, encompassing lower body haemangioma with urogenital, spinal, bony, anorectal, arterial, and renal anomalies. These infants may need MRI of the lumbosacral spine, with ultrasound only considered in very young infants.
Propranolol: Practical prescribing messages
Dr O’Connor presented propranolol as the key treatment for problematic IH. Indications include cosmesis, ulceration, visual threat, airway risk, feeding problems, risk to breast development, haemangiomatosis, and syndromic haemangiomas such as PHACE or LUMBAR.
Notably, he described a pragmatic outpatient prescribing approach in which he does not routinely monitor blood pressure, heart rate or glucose in standard cases. His practice is to start propranolol 1mg/kg twice daily using a 50mg/5mL solution, review every three months in younger infants, four to six monthly in older infants, and generally stop after 12 months of age. Parents are advised not to give propranolol if the child is feeding poorly or vomiting, and to administer it in the morning and mid-afternoon to minimise sleep disturbance.
Another useful distinction was between IH and congenital haemangioma. The latter is fully formed at birth, may be rapidly involuting, partially involuting or non-involuting, and does not respond to propranolol. History is therefore critical.
He also warned that a so-called “bleeding haemangioma” may not be a haemangioma at all. True IHs are not simply “bags of blood” and usually do not bleed significantly. Heavy or recurrent bleeding should raise suspicion for pyogenic granuloma, which presents later and bleeds readily.
Vascular malformations and capillary birthmarks
In contrast to IH, vascular malformations are always present at birth and grow proportionately with the child. These include capillary, venous, lymphatic, and combined malformations.
Dr O’Connor distinguished naevus simplex from true capillary malformations. Naevus simplex is extremely common, affecting around half of neonates. Lesions on the eyelids and glabella usually fade by age two, whereas nuchal lesions (or “stork bites”) may persist lifelong. More extensive patterned involvement may represent naevus simplex complex.
For capillary malformations involving the forehead, he emphasised the need to consider Sturge–Weber syndrome. The practical rule given was that MRI brain with contrast and ophthalmology review are indicated only when there is forehead involvement. This distinction helps avoid over-investigation of V2-only lesions.
Pigmentary lesions: Low melanoma risk, but know the exceptions
Dr O’Connor’s discussion of congenital melanocytic naevi (CMN) was intentionally reassuring. CMN may be present at birth or become apparent in the first year and are classified by predicted adult size. He stressed that the risk of melanoma is generally low, and for a single CMN it is vanishingly rare in childhood. Most melanomas arise de novo rather than from a pre-existing naevus.
Management therefore centres on photoprotection, reassurance, and self-monitoring later in life. Hair can be shaved, trimmed or removed with depilatory cream if desired, but plucking should be avoided. Elective excision is not routinely required unless there are cosmetic concerns. He was also firm that laser should not be used for pigmented lesions, because it is ineffective and may obscure the diagnosis of melanoma.
The more nuanced point concerned CMN syndrome, reflecting possible neurological involvement due to shared neural crest origins of melanocytes and elements of the nervous system. Risk increases with multiple CMN and a larger main lesion (Figure 3). MRI screening remains controversial, but Dr O’Connor’s own rule was pragmatic: Consider MRI brain and whole spine with contrast in the first six months when there are two or more CMN and at least one is >5cm. He stated explicitly that single CMN, even if midline, do not warrant MRI.
He also reviewed congenital dermal melanocytosis, advising clinicians not to use the term “Mongolian blue spot”. These lumbosacral bluish-grey lesions are common in infants with more deeply pigmented skin, usually fade by age four, and are important to document clearly because they can be mistaken for bruising or non-accidental injury.

FIGURE 3: Multiple CMN and a large main lesion
Other pearls: Mastocytosis, sebaceous naevi, and neurofibromatosis type 1 clues
Among other useful outpatient messages, Dr O’Connor highlighted cutaneous mastocytosis as a cause of lesions that may be mistaken for bruising, safeguarding concerns, or meningococcal disease. Children are usually otherwise well. Recognition of Darier sign and typical morphology can avoid inappropriate escalation. Clinical forms include mastocytoma, urticaria pigmentosa, and diffuse cutaneous mastocytosis.
Naevus sebaceous was described as a yellow-orange smooth plaque, typically on the scalp, forehead or temple, often more obvious at birth due to maternal hormones. It tends to become more verrucous at puberty. The key practical points were that the risk is mainly of trichoblastoma, which is benign, and that if removal is desired it is best referred to plastic surgery in late childhood, not infancy.
Dr O’Connor used multiple scalp yellow-orange papules as a clue to juvenile xanthogranulomas and possible nuurofibromatosis type 1 (NF1) association. More broadly, he reminded clinicians that NF1 is rarely clinically diagnosable in infancy, because many features emerge over time. This is important when counselling parents about café-au-lait macules or related findings in the first year of life.
Infectious neonatal dermatoses: Think clinically, but think early
In contrast to the benign transient eruptions, infectious neonatal skin disease requires careful attention to context. Dr O’Connor stressed that gestation, maternal history, timing, morphology, and systemic status are critical. Risk factors such as prematurity, prolonged rupture of membranes, maternal pyrexia, chorioamnionitis, maternal HSV (herpes simplex virus) and GBS (group B streptococcus) infection, and poor neonatal condition increase concern.
Staphylococcal skin infection featured prominently. Localised folliculitis and furuncles may occur, especially in preterm or immunocompromised babies, and should prompt bacterial swab and anti-staphylococcal treatment. Bullous impetigo is caused by Staphylococcus aureus toxin-mediated blistering and presents with superficial bullae and erosions; bacterial culture can be obtained from blister fluid.
More severe still is staphylococcal scalded skin syndrome (SSSS), especially in neonates who lack protective antibodies and have immature renal clearance of toxin. The characteristic sequence is diffuse erythema, wrinkling, blistering, peeling, and a positive Nikolsky sign, with mucous membranes relatively spared because the toxin targets desmoglein 1.
The practical point is that in suspected SSSS, clinicians should swab likely colonisation sites such as the nose, eyes, throat or umbilicus rather than intact blisters, and treat promptly with intravenous (IV) anti-staphylococcal antibiotics and supportive skin care.
Congenital infections remain important. Dr O’Connor used the classic example of congenital syphilis, particularly in the setting of absent antenatal serology. The dermatological clue is a palmoplantar vesiculobullous or maculopapular eruption with erythema and desquamation.
As syphilis incidence is rising, clinicians should keep it on the differential, especially when rash involves palms and soles. He also reminded attendees that false-positive VDRL (venereal disease research laboratory) results can occur in pregnancy, so treponemal antibodies are important in interpretation.
A rarer, but memorable, diagnosis was granulomatosis infantiseptica, the disseminated cutaneous form of congenital listeriosis, presenting with widespread papulonodular skin lesions in an unwell newborn, often against a background of maternal febrile illness or chorioamnionitis.
Neonatal herpes simplex was presented as a must-not-miss diagnosis. Vesicles, erosions or crusted lesions on skin, scalp, eyes, mouth or perineum in a neonate should prompt urgent investigation. Dr O’Connor outlined the extensive workup required: HSV PCR (polymerase chain reaction) from mucocutaneous lesions, blood and cerebrospinal fluid, and treatment with IV aciclovir pending results. He noted the importance of maternal timing: Third trimester maternal infection carries particular risk, and booking serology may not detect later infection.
Similarly, neonatal varicella remains relevant. Maternal immunity status matters greatly, and exposed non-immune mother or baby may require varicella-zoster virus immunoglobulin, while symptomatic neonates need IV aciclovir. Congenital varicella syndrome and scarring are separate but related concerns.
Rare and serious neonatal dermatoses: Early dermatology input is essential
One of the strongest messages in the neonatal talk was that some babies with severe skin disease need urgent dermatology involvement, often alongside tertiary paediatrics.
Neonatal erythroderma, defined as redness involving more than 90 per cent of the skin, is a rare clinical term rather than a final diagnosis. Differential diagnoses include infection, immunodeficiency, drug reactions, ichthyoses, metabolic disorders, and, more rarely, neonatal presentations of common inflammatory dermatoses. Dr O’Connor was explicit that atopic dermatitis is not a neonatal erythroderma diagnosis. That point is clinically useful, because ‘eczema’ is often used too loosely in unwell red infants.
He discussed epidermolysis bullosa (EB) as a key neonatal blistering disorder. Extensive blistering or erosions at birth, particularly with mucosal involvement or trauma-induced lesions, should raise suspicion. The major practical pearl was referral – get these babies to an expert centre, handle gently, and do not attempt to give families a prognosis before expert assessment and subtype clarification.
Collodion membrane was another important presentation. These babies are born encased in a shiny, taut membrane that later sheds to reveal the underlying disorder, most often an autosomal recessive congenital ichthyosis, though a self-healing phenotype exists. Management is largely supportive: Liberal paraffin-based emollients, eye lubrication, and careful monitoring. Again, prognosis should be left to specialist teams.
Finally, incontinentia pigmenti was presented as a classic pattern-recognition diagnosis – usually in female infants, following the lines of Blaschko, progressing through vesicular, verrucous, hyperpigmented, and sometimes, hypopigmented phases. The broader significance is that it is not just a skin disorder; teeth, cenral nervous system, eyes, and breast tissue may also be involved.
Conclusion
Dr Cathal O’Connor’s presentations distilled neonatal and infantile dermatology into a series of memorable clinical rules. Many neonatal eruptions are benign and transient, but they are frequently misread as infection. Conversely, a small but important group of rashes and birthmarks require urgent recognition because they indicate serious infection, syndromic disease, genodermatosis, nutritional deficiency, or a narrow treatment window.
For Irish GPs and hospital doctors, perhaps the most important practical take-home messages are these: Know the timing of IH, because early referral to dermatology changes outcomes; do not undertreat infantile eczema, especially on the body; recognise that atopic dermatitis spares the napkin area; and refer children with skin disease to dermatology rather than to general paediatrics, as this is the appropriate route to correct diagnosis and management.
