






Reference: March 2026 | Issue 3 | Vol 12 | Page 16
Hypertension is common and remains one of the most modifiable risk factors encountered in clinical practice. A World Health Organisation report published in 2023 revealed that the number of individuals with hypertension doubled from 650 million in 1990 to 1.3 billion in 2019.1
Although high blood pressure (BP) can be effectively controlled with medications, undertreated hypertension remains a major cause of premature death, accounting for an estimated 10.8 million avoidable deaths annually.1 Furthermore, hypertension is an important risk factor for cardiovascular disease (CVD), cerebrovascular disease, chronic kidney disease (CKD), and dementia.2 For clinicians, this represents a major opportunity for prevention.
Significantly, a 2023 meta-analysis demonstrated that untreated hypertension was associated with a greater risk of dementia, whereas treated hypertension conferred no greater dementia risk compared to healthy controls.3 This reinforces the importance of timely diagnosis and sustained BP control, particularly in mid-life and older adults, the benefits of which are also replicated in the management of CKD, stroke, and CVD.
Guidelines on the management of hypertension are available, and updates are released regularly. From a European perspective, the European Society of Cardiology (ESC) published updated evidence-based guidelines for the management of elevated BP and hypertension in August 2024, while the European Society of Hypertension (ESH) released guidelines for the management of hypertension in December 2023.
Both guidelines define hypertension as an office systolic BP (SBP) ≥140mmHg and/or diastolic BP (DBP) ≥90mmHg. One point of differential is that the 2024 ESC guidelines define ‘elevated BP’ as an SBP value of 120-139 or a DBP value of 70-89, whereas the ESH do not define this category.
Another significant difference between the two guidelines is that the ESC guidelines advise a target BP of <130/80mmHg for those with hypertension on treatment, while the ESH guidelines focus on the target BP of <140/90mmHg. These differences in target thresholds have important implications for estimating population-level control rates and for day-to-day clinical decision-making.
Our research team at The Irish Longitudinal Study on Ageing (TILDA) in Trinity College Dublin recently investigated the prevalence, awareness, treatment, and control of hypertension, as well as adherence to the ESC hypertension guidelines, over 12 years of follow-up in the Irish context.
TILDA is a population-based prospective cohort study, representative of community-dwelling adults, aged 50 years or older living in Ireland. The initial study sample involved over 8,500 participants and each member of the population in Ireland aged 50 years and older had an equal probability of being invited to participate.
Data collection is conducted in biennial waves, including a computer-assisted personal interview, a self-complete postal questionnaire, and a health assessment every four to six years.4
Our study, ‘Adherence to the ESC hypertension guidelines over 12 years of follow-up in the Irish population’ which was published in Open Heart, defined hypertension as a mean SBP ≥140mmHg and/or mean DBP ≥90mmHg or currently taking any anti-hypertensive medication.5
BP was measured by a healthcare practitioner at the health assessment using a digital automated oscillometric BP monitor. It was recorded twice while seated with a timed interval of one minute between readings. The mean systolic and diastolic readings were obtained from these two measurements. This study focused on data collected at Wave 1 (2009-2011), Wave 3 (2014-2015) and Wave 6 (2021-2023) due to the availability of health assessment data at these waves.
Study findings
Results of the study have clear implications for routine clinical practice in both primary and secondary care settings. Key findings include:
- Hypertension prevalence remained consistently high, increasing from 63 to 71 per cent over 12 years of follow-up.
- Only 56 per cent of those with hypertension were aware they had it, highlighting substantial ongoing under-diagnosis.
- 71 per cent of those with hypertension were taking a medication. Treatment intensity was often suboptimal: Only 14 per cent were prescribed a guideline-recommended dual therapy and only 57 per cent were prescribed a guideline-recommended monotherapy, suggesting potential therapeutic inertia or under-escalation of treatment.
- Among those receiving treatment, just 33 per cent achieved the 2024 guideline-recommended blood pressure target of <130/80mmHg, while 54 per cent were controlled to <140/90mmHg.
- Overall, using the higher BP target of <140/90, 62 per cent of those with hypertension in Ireland (445,000 people) were not appropriately managed, consistent with previous TILDA evidence showing poor long-term control of modifiable cardiovascular risk factors.
- When the lower BP target of <130/80mmHg, as advised by the 2024 ESC guidelines, is applied, this figure rises to 77 per cent, meaning more than three out of every four older adults with hypertension in Ireland were not optimally managed.
- Forty per cent of the population were in the ‘elevated BP’ category identified by the ESC (SBP 120-139mmHg or DBP 70-89mmHg). Notably, 71 per cent of this group had evidence of high cardiovascular risk. This represents a large cohort in whom earlier intervention may alter long-term outcomes.
- People aged 85 + years and those with moderate to severe frailty were less likely to have undiagnosed hypertension and were more likely to be taking guideline-recommended medications – similar rates of blood pressure control when compared to the wider population.
- People with CKD were more likely to receive guideline-recommended treatment and achieve blood pressure control to a target of <140/90mmHg, suggesting targeted care can be effective in high-risk groups.
Unmet need
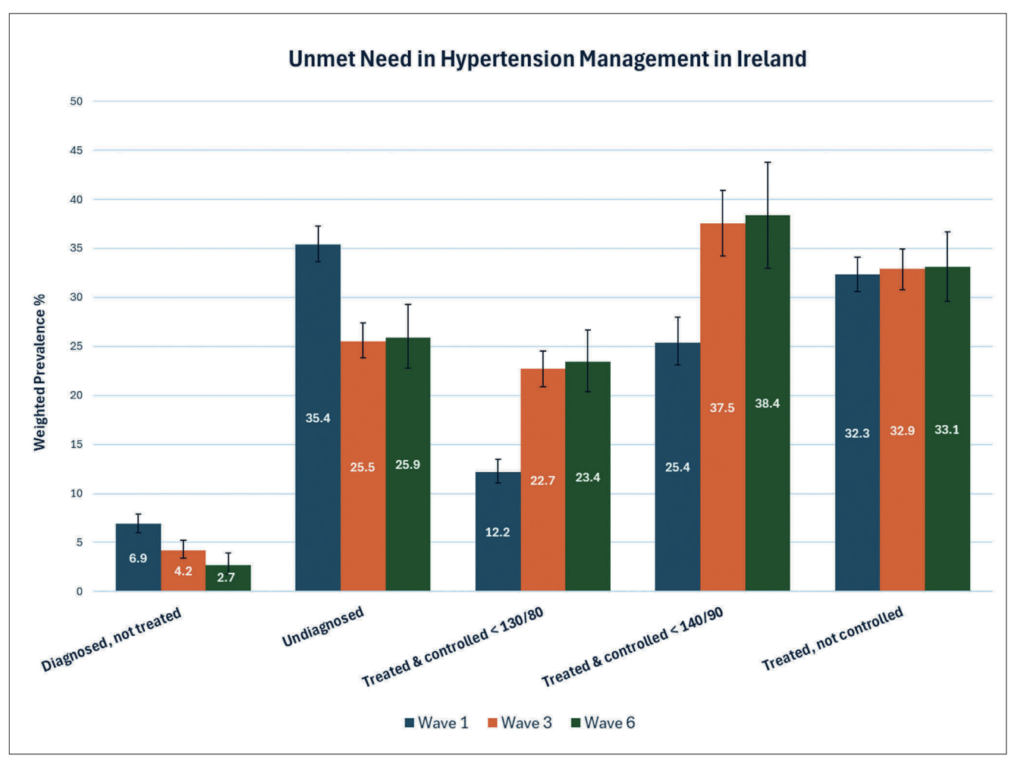
Based on data collected between 2021 and 2023 at Wave 6, 61.7 per cent of people with hypertension in Ireland were not appropriately managed, according to the 2018 guidelines which recommend a BP target of <140/90. This group either had undiagnosed hypertension, were diagnosed but not on treatment, or were on treatment but not controlled to a target BP of <140/90. This figure was 74.6 per cent in Wave 1 and 62.3 per cent at Wave 3, as demonstrated in Figure 1.
Using the lower BP target of <130/80, as advised by the 2024 ESC guidelines, 87.8 per cent, 77.1 per cent, and 76.7 per cent of those with hypertension at Waves 1, 3, and 6, respectively, were not appropriately managed.
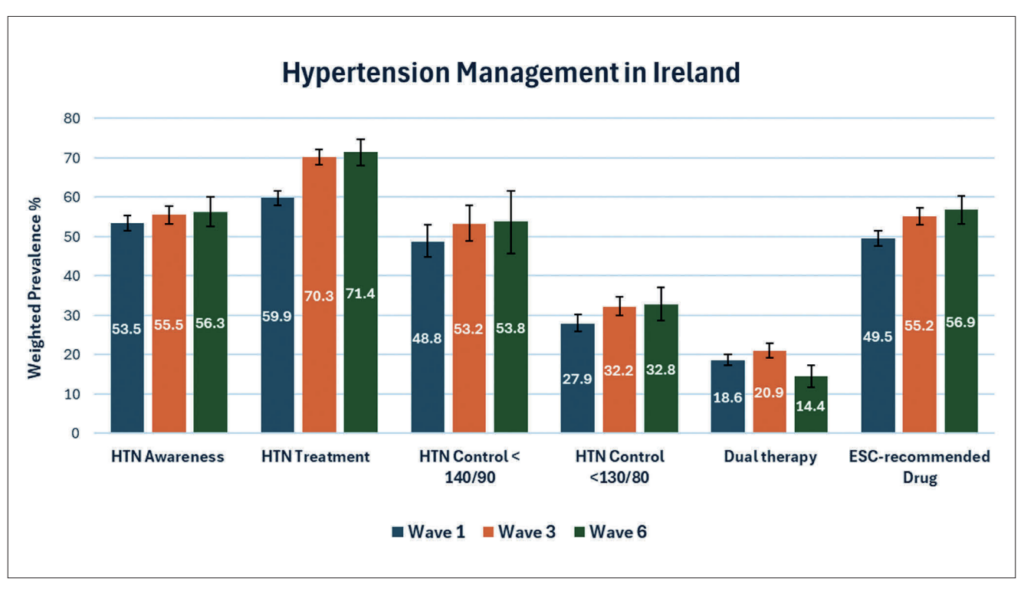
Figure 1 demonstrates a detailed breakdown of the unmet need in hypertension management in Ireland at three time points over 12 years of follow-up. Figure 2 demonstrates changes in hypertension awareness, treatment, and control at three time points over 12 years of follow-up. Findings demonstrate modest increases in each category across the follow-up period except in the case of dual therapy prescription.
Discussion
This study demonstrates a high prevalence of hypertension (71%) in community-dwelling adults aged 50 years and older in Ireland. This corresponds to an estimated hypertension burden of over 700,000 people at each wave in this population group. For context, at the time of Wave 6, Ireland’s population of community-dwelling adults over 50 years old was estimated to be 1.1 million people based on 2022 Census data.
For clinicians practicing in Ireland, this equates to hundreds of thousands of patients at elevated cardiovascular risk, many of whom are potentially modifiable through improved detection and optimisation of therapy.
According to the most recent data, 76.7 per cent of those with hypertension were not appropriately managed. This means that they were either diagnosed with hypertension but not on treatment, on treatment for hypertension but not controlled to a BP target of 130/80, or that they had undiagnosed hypertension.
Applying a BP target of 140/90, 61.7 per cent of those with hypertension were not appropriately managed. As seen in Figure 2 there is significant room for improvement in terms of the prescription of dual therapy and guideline-recommended anti-hypertensive agents.
The 2024 ESC guidelines place increased emphasis on the category of elevated BP, not meeting the criteria for hypertension. In this study, those with elevated BP ranged from 37.3-40.7 per cent of the population, amounting to approximately 450,000 people aged 50 years and older at each. Most of this group at Wave 3, 71.0 per cent or 346,209 people, had evidence of high cardiovascular risk.
As advised by the guidelines, individuals with elevated BP and high cardiovascular risk may warrant treatment to similar targets as for those with documented hypertension. This raises important questions for clinicians working in Ireland regarding earlier pharmacological intervention.
The subgroup analyses of this study focused on those aged 85 years or older, those with moderate to severe frailty, and those with CKD. All groups demonstrated a high prevalence of hypertension. Individuals aged ≥85 years and those with moderate to severe frailty were less likely to have undiagnosed hypertension.
Those with higher frailty scores were more likely to be taking anti-hypertensive medications, including those recommended by the ESC guidelines, and had similar rates of BP control <130/80mmHg to the overall population. This contrasted with those aged ≥85 years who had lower rates of anti-hypertensive use compared to those with frailty, perhaps reflecting a tendency to deprescribe in older age rather than in frailty.
Interestingly, those with greater frailty or CKD were more likely to receive guideline-recommended therapy, suggesting that increased healthcare contact may improve adherence to best practice.
Prevalence and rates of hypertension awareness, treatment, and control found in this study are very much in keeping with previous studies undertaken in the Irish context. These studies have been based on data from SLÁN, STEPwise approach to NCD risk factor surveillance (STEPS), and TILDA.6,7,8
However, this is not a uniquely Irish problem. An international study published in The Lancet in 2019 examined trends in hypertension among individuals aged 40 and older up to 2017; it noted significant improvements in awareness, treatment, and control during the 1990s and 2000s, with a concerning plateau thereafter.9
In a study published recently in NEJM, Kishore et al offered the explanation that hypertension control remains poor in the United States due to systemic failures, including misaligned incentives, fragmented data systems, and persistent therapeutic inertia, rather than any scientific limitations.10
The authors argue that meaningful improvement will require aligning payment and quality measurement structures – integrating realtime BP data, expanding protocolised teambased care, and creating policies that make long-term prevention financially sustainable.10
In the Irish context, at present, primary care employs the Opportunity Case Finding Programme to identify those with elevated BP and other cardiovascular risk factors. Individuals diagnosed with hypertension are then registered on the Chronic Disease Management Programme for annual review.
However, this system is exclusive to medical card or GP visit card holders and hypertension is not included in the structured programme. In addition, CKD is not yet included in this scheme, despite being a major risk factor for both hypertension and CVD.
However, the Health Minister recently announced the inclusion of CKD in the programme “over the coming months” during a recent Dáil Éireann debate. From a systems perspective, the current structure may unintentionally contribute to gaps in detection and continuity of care.
Conclusion
In summary, hypertension remains highly prevalent and often suboptimally managed in Ireland. Despite clear guidelines and effective treatments, substantial proportions of patients remain undiagnosed, undertreated, or uncontrolled. Improving hypertension care will require greater public awareness, clearer national guidance on guideline adoption, systematic medication optimisation, and strengthened primary care supports. The potential gains in reduced CVD, stroke, CKD, and dementia are considerable.
References
- World Health Organisation. Global report on hypertension: The race against a silent killer. Geneva: WHO; 2023. Available at: www.who.int/publications/i/item/9789240081062
- Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension. 2020;75(2):285-292. doi:10.1161/HYPERTENSIONAHA.119.14240.
- Lennon MJ, Lam BCP, Lipnicki DM, et al. Use of antihypertensives, blood pressure, and estimated risk of dementia in late life: An individual participant data meta-analysis. JAMA Netw Open. 2023;6(9):e2333353. doi:10.1001/jamanetworkopen.2023.33353.
- Whelan BJ, Savva GM. Design and methodology of the Irish Longitudinal Study on Ageing. J Am Geriatr Soc. 2013;61 Suppl 2:S265-S268. doi:10.1111/jgs.12199.
- McGarvey C, Scarlett S, Briggs R, et al. Adherence to the European Society of Cardiology hypertension guidelines over 12 years of follow-up in the Irish population. Open Heart. 2025;12(2):e003744. doi:10.1136/openhrt-2025-003744.
- Barron S, Balanda K, Hughes J, Fahy L. National and subnational hypertension prevalence estimates for the Republic of Ireland: Better outcome and risk factor data are needed to produce better prevalence estimates. BMC Public Health. 2014;14:24. doi:10.1186/1471-2458-14-24.
- World Health Organisation. Hypertension Ireland 2023 country profile. Geneva: WHO; 2023. Available at: www.who.int/publications/m/item/hypertension-irl-2023-country-profile
- Murphy CM, Kearney PM, Shelley EB, et al. Hypertension prevalence, awareness, treatment, and control in the over 50s in Ireland: Evidence from The Irish Longitudinal Study on Ageing. J Public Health (Oxf). 2016;38(3):450-458. doi:10.1093/pubmed/fdv057.
- NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: An analysis of 123 nationally representative surveys. Lancet. 2019;394(10199):639-651. doi:10.1016/S0140-6736(19)31145-6.
- Kishore SP, Kocher R. The hypertension control paradox – why is America stuck? N Engl J Med. 2026;394(5):417-420. doi:10.1056/NEJMp2515023.
- Dail Eireann (2025) Disease Management, Dáil Éireann Debate. Available at: www.oireachtas.ie/en/debates/question/2025-03-06/142/ [accessed 11 February 2026].
