Reference: March 2024 | Issue 3 | Vol 10 | Page 41
An aortic aneurysm is a localised swelling or bulging of the aorta. It can occur in any part of the aorta. By definition, an aneurysm is diagnosed when there is a dilatation of the vessel more than 1.5 times its original size. The normal dimension of a thoracic aorta is roughly 2.5-to-3.5cm, depending on the location and the size of the individual. In general, the aorta is considered aneurysmal when its size reaches beyond 4cm.
Anatomy of thoracic aorta
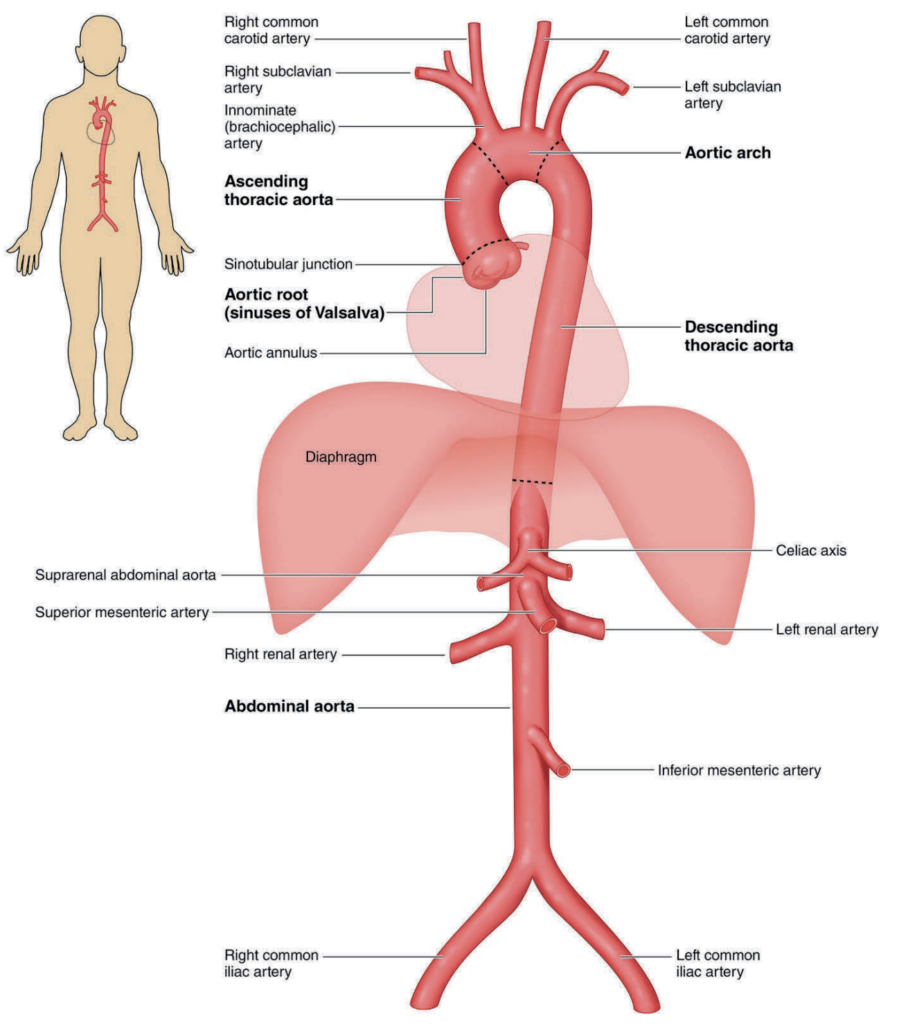
The thoracic aorta commences just above the aortic valve (see Figure 1). This segment is known as the aortic root, whereby the coronary arteries arise out of the coronary sinuses, of which there are three: The left coronary sinus, the right coronary sinus, and the non-coronary sinus. The left and right main coronary arteries arise out of the corresponding coronary sinuses.
Beyond this, the aorta continues in its ascending course and is known as the ascending aorta. The demarcation point between the aortic root and the ascending aorta is known as the sinotubular junction. The ascending aorta then arches around the pulmonary artery. Here, it gives off the three ‘head and neck vessels’ – the innominate artery, the left common carotid artery, and the left subclavian artery. This segment of aorta is known as the arch of aorta.
The aortic arch then continues its descending course as the descending aorta on the left side of the thoracic cavity, giving off intercostal arteries and arteries to the spinal cord known as the artery of Adamkiewicz (arteria radicularis magna) in the lower portion of the thoracic cavity. Beyond this, piercing the diaphragm, it continues as the abdominal aorta.
The location of the aneurysm is important for a number of reasons. Depending on the location, the symptoms defer. In the aortic root, aneurysm in this area is often associated with aortic valvular disease. This is especially associated with patients having bicuspid aortic valvulopathy, and commonly diagnosed as a result of it.
As for ascending aortic aneurysm, this can be associated with aortic valvular disease, or more commonly, is found incidentally on imaging usually indicated for other reasons. Both aortic root and ascending aneurysm seldom cause any symptoms.
Aneurysm of the aortic arch can be associated with either ascending or descending aortic aneurysm or can occur on its own. Aneurysm in this area can lead to compression of a number of neighbouring structures, leading to symptoms such as hoarseness (recurrent laryngeal nerve), dysphagia (oesophagus), or shortness of breath (bronchus).
Aneurysm of the descending aorta is usually not associated with any symptoms and often found incidentally on imaging. Patients can sometimes present with very mild chest pain.
However, all aneurysms can dissect. This happens when there is an intimal tear in the intimal layer; blood traverses into this defect and splits the middle muscular layer (also known as tunica media). This leads to two separate lumens of the aorta, a ‘true’ (original) lumen and a ‘false’ (lumen between the media layers and sometimes between the media layer and the adventitial layer) lumen.
Patients tend to present with sudden severe central chest pain radiating to the back. This is often associated with severe hypertension. The condition has a high mortality rate, and 90 per cent of patients will succumb to it in the immediate aftermath. Those who survive the initial dissection still have a poor prognosis and need to be treated immediately, as it can lead to aortic rupture, cardiac tamponade, acute severe aortic regurgitation, and distal organ malperfusion.
Pathology and associated conditions
Causes of thoracic aortic aneurysm include heritable disorders (Marfan syndrome, Loeys-Dietz syndrome, Ehlers-Danlos syndrome, familial thoracic aortic aneurysm); congenital conditions (bicuspid aortic valve, Turner’s syndrome, coarctation of aorta); multifactorial degenerative conditions; previous aortic dissection; inflammatory diseases (giant cell arteritis, Behcet disease, Takayasu arteritis); and infectious diseases (bacterial, fungal, syphilitic).
Aneurysms of the aortic root and ascending thoracic aorta tend to have a heritable influence and present at younger ages, whereas aneurysms of the descending thoracic aorta tend to be degenerative and present at older ages. Moreover, aneurysms of the aortic root and ascending thoracic aorta are also commonly associated with bicuspid aortic valve.
Guidelines for treatment
Surgical repair remains the mainstay of treatment for most thoracic aortic aneurysm except for the descending aorta, whereby it is mainly treated via an endovascular approach. The treatment indications for thoracic aortic aneurysm are mainly for prophylaxis of dissection.
As the surgical treatment is still associated with sometimes significant morbidity and even mortality, indication should be carefully evaluated on an individual basis. Guidelines exist to guide the timing of surgery.
In general, surgical treatment is recommended based on:
1. Absolute dimension
- >5.5cm;
- >5.0cm if associated with bicuspid valve;
- >4.5cm if associated with connective tissue disorder, if patient was undergoing concomitant cardiac surgery such as coronary artery bypass graft or valvular repair/replacement.
2. Rate of growth >0.3cm/year
Decision to intervene should be made at the aortic multidisciplinary meeting and guided by the patient’s body surface area and comorbidities.
Surgical treatment
Detailed surgical treatment is beyond the scope of this article. Some details are elucidated in the featured case studies. Briefly, surgical treatment entails resecting the diseased aneurysmal segment and replacing it with a synthetic tube graft.
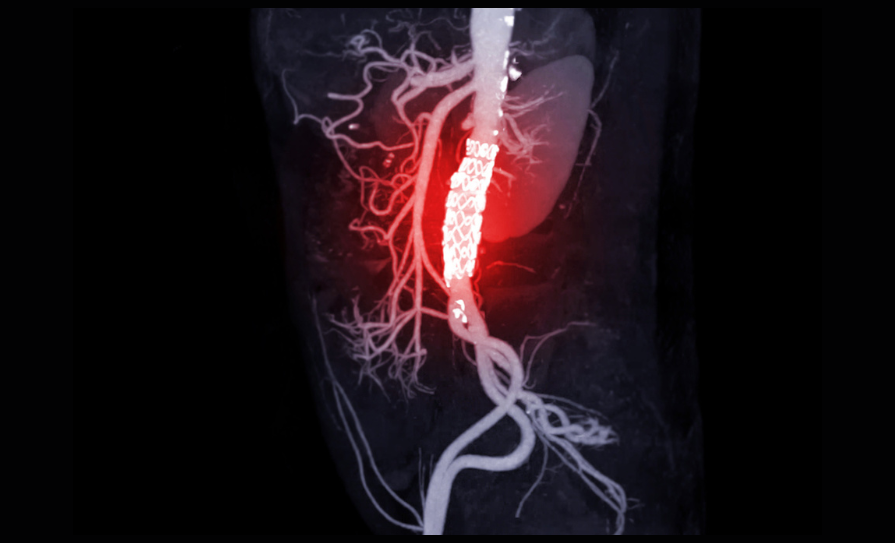
The current available prostheses are made out of a material known as polytetrafluoroethylene. The material is inert, non-porous, and non-degradable. Currently, surgical repair remains the only treatment option for suitable patients requiring replacement of the aortic root, ascending aorta, and the aortic arch. Aneurysm of the descending aorta is increasingly treated with the endovascular approach using a covered stent graft.
References on request
CASE STUDY 1
A 78-year-old man who is generally fit and well, with only a past history of very mild dementia and hypertension, presented to his general practitioner with mild shortness of breath. He was initially treated with antibiotics for respiratory tract infection.
However, during the consultation, a murmur was detected in the aortic area. He was promptly referred to the cardiology service for further evaluation. Initial assessment via echocardiography revealed moderate mixed aortic valve disease with preserved left ventricular function. There were no other valvular problems. Incidentally, a severely dilated aortic root was detected.
A CT aorta was subsequently performed following consultation with the cardiac surgical service. This revealed a severely dilated aortic root, measuring around 7cm and extending to the mid ascending aorta. The rest of the aorta was normal in size. To complete the investigations, coronary angiography was performed, revealing mild non-obstructive coronary artery disease, and a right dominant circulation.
The patient’s case was discussed in the multidisciplinary meeting and was deemed to have met the criteria for surgery. Following informed consent, the patient was planned for an elective aortic root replacement.
Intra-operatively, following sternotomy, establishment of mild hypothermic cardiopulmonary bypass and myocardial arrest, the aorta was transected at the mid ascending aorta. The aortic root tissue was then resected with preservation and mobilisation of the coronary ostia as buttons. The aortic valve was also resected in this case as there was moderate aortic valve disease.
Following that, a bovine bioprosthetic valve was sutured into a tube graft made of PTFE. This was used to replace the aortic root and aortic valve. Two 1cm2 incisions were made in the graft, and the coronary buttons anastomosed onto it. The distal end of the graft was then measured to length and anastomosed to the native ascending aorta.
Once surgery was completed, the heart was reanimated and separated from cardiopulmonary bypass. The patient’s incision was then closed and they were transferred to the intensive care unit. The patient made an unremarkable recovery and was discharged about a week later. As it was a bioprosthetic valve, he did not require long-term anticoagulation.
CASE STUDY 2
A 44-year-old man was brought in by ambulance to the emergency department following complaints of sudden, severe, central crushing chest pain. Following a negative troponin, a CT pulmonary angiogram was performed to rule out pulmonary embolism. This demonstrated a type A aortic dissection arising from just above the right coronary artery and extending to the proximal arch of aorta. This is associated with a dilated ascending aorta.
The patient was stable and had no symptoms or signs of malperfusion. He had no previous history other than newly diagnosed hypertension. However, he had a strong family history of aortic dissection (sister) and aortic aneurysm (uncle).
He was brought urgently to the operating theatre as aortic dissection is a life-threatening emergency when it progresses to severe acute aortic incompetence, cardiac tamponade, aortic rupture, and malperfusion of vital organs.
Intra-operatively, following slow induction of general anaesthesia and establishment of cardiopulmonary bypass via peripheral cannulation of the femoral vessels, moderate hypothermia and myocardial arrest was induced. The aorta was then transected to assess for the entry point of the intimal tear in the aorta. This usually arises just above the coronary ostia, but sometimes can extend down into the aortic root and complicate repair.
In this case, the intimal tear was in the typical position just above the right coronary ostia and limited to the ascending aorta. The ascending aortic tissue was then resected including the intimal tear. Following that, the layers of dissected aorta in the aortic root were reapproximated with a combination of bioglue and sutures to reconstruct an aortic root. A standard PTFE tube graft was then anastomosed to it. As opposed to normal anastomosis, anastomosis in aortic dissection cases are further reinforced with Teflon strips to strengthen the tissue.
Once completed, we turned our attention to the aortic arch. At this stage, hypothermic circulatory arrest (whereby patient’s circulation is essentially suspended for a short period of time) was started and the aortic arch inspected for further entry tears that needed to be addressed.
In this patient’s case, there was none. Hence, the layers of aorta, similar to the root, was reapproximated in similar fashion with a combination of glue and sutures. This was then anastomosed to the tube graft. Once completed, the patient was rewarmed completely back to normal body temperature.
The patient was then separated from cardiopulmonary bypass. Following careful haemostasis and chest closure, the patient was transferred to the intensive care unit.
Due to the period of circulatory arrest, the patient was kept on sedation for a period of time to allow for brain recovery. The patient was extubated on day two successfully. The remainder of his recovery was uneventful.