






Reference: March 2024 | Issue 3 | Vol 10 | Page 22
Valvular heart disease is a leading cause of cardiovascular morbidity and mortality.1 The prevalence of mitral valve disease (MVD) is increasing with the ageing population and poses a substantial burden to healthcare systems worldwide. MVD includes a spectrum of conditions.
The three most common diseases of the mitral valve include mitral stenosis, mitral regurgitation, and mitral valve prolapse.1,2 Mitral regurgitation is the most frequently diagnosed of the three, accounting for approximately 9.3 per cent of MVDs in those over 75 years. Mitral stenosis accounts for around 0.2 per cent.1
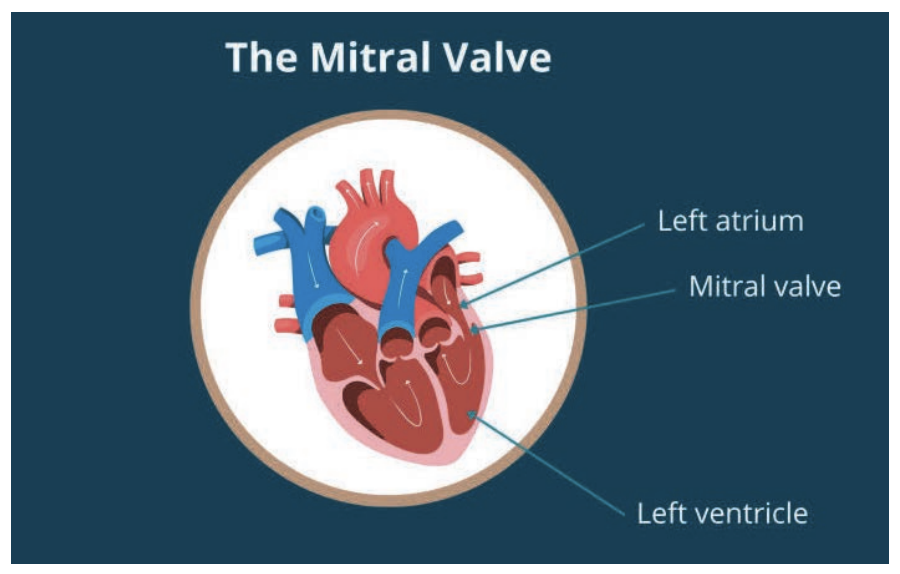
Figure 1: The mitral valve source: www.rbhh-specialistcare.co.uk/news/mitral-valve-problems
Pathophysiology
The mitral valve is a bileaflet valve positioned between the left atrium and left ventricle. The mitral orifice area ranges from 4-to-6cm2. Under normal physiological conditions, the mitral valve opens during left ventricular diastole, facilitating the passage of blood from the left atrium to the left ventricle. During diastole, the pressure in both the left atrium and left ventricle is equal.
The left ventricle undergoes blood filling in early ventricular diastole, leaving only a small quantity of blood in the left atrium. This residual blood contributes to the left ventricular filling through the contraction of the left atrium, often referred to as the ‘atrial kick’, occurring in late ventricular diastole.2
If not closed tightly enough, or if the mitral valve’s size and shape are altered, blood may leak in the wrong direction. Mitral valve stenosis occurs when the mitral valve narrows, restricting blood flow into the main pumping chamber of the heart. The mitral valve may also leak, causing blood to flow back through the valve each time the left ventricle contracts, leading to mitral valve regurgitation.2
Mitral stenosis
Mitral stenosis is characterised by the narrowing of the mitral valve orifice. The most common cause is rheumatic fever, although the stenosis usually does not become clinically noticeable for 20-to-40 years after an episode of rheumatic fever. Uncommon causes of mitral stenosis are calcification of the mitral valve leaflets and congenital heart disease. Other causes include infective endocarditis, mitral annular calcification, endocardial fibroelastosis, malignant carcinoid syndrome, systemic lupus erythematosus, Whipple disease, Fabry disease, and rheumatoid arthritis.3,4
Despite a global decline in its prevalence, rheumatic heart disease remains the most common cause of mitral stenosis.3 The clinical manifestation of rheumatic mitral stenosis varies. In global regions where the disease is prevalent, individuals typically present at a young age (teenager-to-30 years) with commissural fusion and pliable non-calcified valve leaflets, often associated with regurgitation. In Western countries, with a lower disease prevalence, mitral stenosis is usually detected in older people (50-to-70 years) who present with calcified fibrotic leaflets in addition to commissural fusion and sub-valvular involvement.1
Mitral regurgitation
Mitral regurgitation, sometimes called mitral insufficiency or mitral incompetence, is caused by the retrograde flow of blood from the left ventricle into the left atrium through the mitral valve, causing a systolic murmur best heard at the apex of the heart with radiation to the left axilla. It is the most common valvular abnormality worldwide, affecting over 2 per cent of the global population, and has a prevalence that increases with age.5 Mitral regurgitation is the second most frequent valvular heart disease in Europe.3
Mitral regurgitation is divided into primary (or organic) and secondary (or functional) mitral regurgitation. Primary mitral regurgitation is a pathology of the mitral valve itself, whereas secondary mitral regurgitation is a pathology of the left atrium, or left ventricle, that affects the function of the mitral valve.
Secondary mitral regurgitation can be classified into ischaemic or non-ischaemic, depending on the cause. Common causes of mitral regurgitation are mitral valve prolapse, rheumatic disease, ischaemic disease, endocarditis, congenital heart defects, and dilated cardiomyopathy.3 Mitral valve prolapse related to myxomatous degeneration of the mitral valve is the most common cause of primary mitral regurgitation.5
In mitral valve prolapse, also called floppy mitral valve, the valve is slightly deformed and bulges back into the left atrium when the ventricle contracts. This can allow a small amount of blood to leak back into the left atrium. As many as one-in-10 people have some degree of mitral valve prolapse, which usually causes little or no symptoms as the amount of blood that leaks back is minimal. In primary mitral valve prolapse, advancing age is the driving factor responsible for disease progression.5,6
Clinical presentation of mitral valve disease
Mitral stenosis: The most common symptoms of mitral stenosis are orthopnoea and paroxysmal nocturnal dyspnoea. Patients may have symptoms of palpitations, chest pain, haemoptysis, thromboembolism (when the left atrial volume is increased), and ascites, oedema, and hepatomegaly if right-sided heart failure develops. There is also an increase in symptoms of fatigue and weakness with exercise and pregnancy.5
Advanced mitral stenosis presents with signs of right-sided heart failure (jugular venous distention, parasternal heave, hepatomegaly, ascites) and/or pulmonary hypertension. Other signs include atrial fibrillation, left parasternal heave (right ventricular hypertrophy due to pulmonary hypertension), and a tapping apex beat.5
Mitral regurgitation: Mild mitral regurgitation may not cause any symptoms. The symptoms associated with more severe mitral regurgitation include shortness of breath, fatigue, palpitations, and ankle oedema.6
Acute mitral regurgitation: Acute mitral regurgitation is usually caused by myocardial infarction involving the left coronary artery, resulting in development of necrotic tissue that is unable to support the chordae. It can also occur with endocarditis when the infection results in an abscess at the area of the chordae causing rupture.
In acutemitral regurgitation, the patient will usually complain of significant dyspnoea at rest, exacerbated in the supine position, as well as cough with clear or pink, frothy sputum. They may also experience symptoms associated with myocardial ischaemia, such as chest pain radiating to the neck, jaw, shoulders, or upper extremities, nausea, and diaphoresis.5
Chronic mitral regurgitation: Patients often exhibit no symptoms until the later stages of disease progression. Common clinical findings across all aetiologies include fatigue, exertional dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea, weight gain, widened pulse pressure, apical holosystolic murmur with radiation to the axilla, dependent oedema, displaced apical impulse, and jugular venous distension.
In advanced cases, syncope or near syncope, cyanosis, clubbing of digits, anasarca, hepatomegaly, signs of ascites with a fluid wave or shifting dullness, and evidence of pleural or pericardial effusions may also be present.
The latter manifestations indicate the development of pulmonary hypertension and subsequent right ventricular systolic dysfunction resulting from chronic pressure overload. The differential diagnosis is extensive, with specific clinical findings dependant on the underlying aetiology. Chronic mitral regurgitation due to primary MVD is best treated by mitral valve replacement because the valve is diseased.5
Investigations and diagnosis
The clinical assessment of mitral valve disease involves a comprehensive evaluation of symptoms, medical history, and physical examination. In mitral stenosis, classic symptoms, such as exertional dyspnoea, orthopnoea, and haemoptysis may be present. In mitral regurgitation, patients may complain of fatigue, palpitations, and signs of heart failure. The presence of a holosystolic murmur and additional auscultatory findings aid in the initial identification of the specific mitral valve pathology.3,4,5
Diagnostic investigations include chest x-ray and electrocardiogram, however, echocardiography remains the cornerstone for diagnosing MVD. Transthoracic echocardiography (TTE) provides a non-invasive and readily available method for assessing valve morphology, measuring orifice areas, and evaluating the severity of regurgitation. Transoesophageal echocardiography offers higher-resolution imaging, particularly valuable in cases where TTE results are inconclusive.2,3,8
Doppler imaging techniques, including colour flow Doppler and continuous-wave Doppler, enhance the accuracy of diagnosing MVDs. These techniques allow for the quantification of regurgitant volumes, assessment of gradients, and determination of valve area in mitral stenosis.3,7,8
Cardiac MRI and CT play a complementary role, especially in cases where echocardiography yields ambiguous results. These modalities offer detailed anatomical information, aiding in the assessment of valve structure, regurgitation severity, and associated complications.3,7,8
Exercise stress testing may be used to detect latent symptoms, assess functional capacity, and determine the impact of physical activity on valve function in MVD.3,7,8
Cardiac catheterisation and left heart catheterisation with angiography may be performed in selected cases to assess haemodynamics, measure gradients, and determine the severity of MVD. These invasive procedures are often reserved for preoperative evaluation in candidates for surgical intervention.3,7,8
Biomarkers and genetic testing may also play a role in risk stratification and early detection. European guidelines for the diagnosis and management of valvular heart disease refer to the use of serum B-type natriuretic peptide (BNP) as a marker of prognosis in aortic stenosis and mitral regurgitation, but thresholds are poorly defined and there are no definitive recommendations on its use.9
Treatment of MVD
Medical management: In both mitral stenosis and mitral regurgitation, medical management plays an important role in symptom relief and prevention of disease progression. Diuretics, beta-blockers, and angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers are commonly employed. Anticoagulation therapy is important in specific cases, particularly for those with atrial fibrillation or a history of embolic events.5,6,10
Invasive management: The most common mitral valve procedures are mitral valve repair, mitral valve replacement, and balloon valvuloplasty.10
Mitral stenosis
Transcatheter interventions, such as percutaneous balloon valvuloplasty, are the treatment of choice for selected cases of mitral stenosis. This procedure provides symptomatic relief by dilating the stenotic valve and restoring normal blood flow.4,10
Valve repair and replacement are now routine cardiac surgical procedures with increasing safety and durability, and are responsible for the increased survival of patients with valvular heart disease.1 Severe cases of mitral stenosis may require surgical intervention, either through mitral valve repair or replacement. Advances in minimally invasive and robot-assisted techniques have improved outcomes and reduced morbidity.4
Mitral regurgitation
Medical versus surgical management of mitral regurgitation depends on the severity, chronicity, comorbidities, and aetiology. Mitral valve repair is considered the gold standard for treating mitral regurgitation. Techniques include annuloplasty, chordal repair, and leaflet resection. Early intervention, particularly in asymptomatic patients with severe regurgitation, is associated with better outcomes.3,5
Mitral valve replacement is used to replace the mitral valve with a mechanical or bioprosthetic valve. It is usually performed when mitral valve repair is not possible.5,10
Transcatheter mitral valve repair and replacement has emerged as a less invasive option for high-risk or inoperable patients with mitral regurgitation. Various devices, such as the Mitraclip, are utilised to repair the valve percutaneously. Ongoing research is exploring the feasibility of transcatheter mitral valve replacement.3,5
Complications of mitral valve surgery/replacement include infections, such as infective endocarditis; bleeding; clotting and stenosis of the new valve; valve dysfunction; arrhythmias; stroke; and death.5
Outlook
Heart valve disease has been described as ‘the next cardiac epidemic’, with prevalence expected to double by 2040 and triple by 2060 due to the ageing population. Under-detection is a key problem. In many patients, symptoms of heart valve disease are difficult to identify and may be confused with general signs of ageing, leading to under-detection.
The timing of interventions for heart valve disease is a key determinant of their effectiveness. The selection of the most appropriate intervention depends on the person’s risk profile and their individual preferences. Even though there has been considerable research on different types of surgery and catheter-based information, there are still gaps in the evidence base.
Research priorities include how to best identify and treat asymptomatic illness, standardised assessment tools to confirm diagnosis, and gathering patient perspectives and preferences regarding their care to inform clinical guidelines and optimise care pathways. Ongoing research is investigating novel therapeutic approaches for MVD, including gene therapy, tissue engineering, and targeted pharmacological interventions. These approaches aim to address the underlying pathophysiology and improve long-term outcomes.11,12
References
- Santangelo G, Bursi F, Faggiano A, et al. The global burden of valvular heart disease: From clinical epidemiology to management. J Clin Med. 2023;12(6):2178.
- Harky A, Botezatu B, Kakar S, et al. Mitral valve diseases: Pathophysiology and interventions. Prog Cardiovasc Dis. 2021;67:98-104.
- Lung B, Delgado V, Rosenhek R, et al. Contemporary presentation and management of valvular heart disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation. 2019;140(14):1156-1169.
- Shah S, Sharma S. Mitral stenosis. StatPearls Publishing: Treasure Island; 2023. Available at: www.ncbi.nlm.nih.gov/books/NBK430742/.
- Douedi S, Douedi H. Mitral regurgitation. StatPearls Publishing: Treasure Island; 2023. Available at: www.ncbi.nlm.nih.gov/books/NBK553135/.
- Willacy H. Mitral regurgitation. Patient Info: UK; 2023. Available at: www.patient.info/heart-health/heart-valves-and-valve-disease/mitralregurgitation/.
- Robinson S, Ring L, Augustine DX, et al. The assessment of mitral valve disease: A guideline from the British Society of Echocardiography. Echo Res Pract. 2021;8(1):G87-G136.
- Mayo Clinic. Mitral valve disease: Diagnosis. Mayo Clinic; 2024/ Available at: www.mayoclinic.org/diseases-conditions/mitral-valve-disease/diagnosis-treatment/drc-20355112.
- Gardezi SK, Coffey S, Prendergast BD, Myerson SG. Serum biomarkers in valvular heart disease. Heart. 2018;104(4):349-358.
- National Health Service. Mitral Valve Problems. National Health Service: UK; 2023 Available at: www.nhs.uk/conditions/mitral-valve-problems/.
- Sitges M, Borregaard B, De Paulis R, et al. Creating a better journey of care for patients with heart valve disease. Eur Heart J Open. 2021;1(3):oeab034.
- Lindman BR, Arnold SV, Bagur R, et al. Priorities for patient-centered research in valvular heart disease: A report from the National Heart, Lung, and Blood Institute Working Group. J Am Heart Assoc. 2020;9(9):e015975.
