







Acne vulgaris, commonly known as acne, is a chronic inflammatory skin condition affecting millions of people worldwide, particularly adolescents and young adults. Acne presents primarily on the face, chest, and back, and is characterised by various lesions including comedones, papules, pustules, nodules, and cysts.
It affects approximately 9.4 per cent of the global population, ranking it eighth among skin diseases. Prevalence rates are estimated to range from 35-to-90 per cent among adolescents. While prevalence decreases with age, acne can remain a significant dermatological concern for adults. Adolescent acne occurs more frequently in males, however, post adolescent acne predominantly affects females.1,2,3
Aetiology
Acne is a multifactorial skin disorder that arises from the complex interplay of genetic, hormonal, microbial, and environmental factors. Genetics play an important role in acne development, with studies indicating a higher prevalence in individuals with a family history of the condition. Genes influence several aspects of acne pathogenesis, including sebum production, keratinisation processes, and the immune system’s response to Cutibacterium acnes (C. acnes).
Environmental factors include diet, climate, pollution, and lifestyle. Dietary habits, particularly the consumption of high-glycaemic-index foods and dairy products, have been linked to acne severity, possibly due to their role in insulin-like growth factor 1 (IGF-1) signalling, which can exacerbate sebum production and inflammation.1,2,3
Acne is profoundly influenced by hormonal factors, particularly those that alter sebaceous gland function. Androgens are pivotal in stimulating sebocyte proliferation, increasing intracellular lipid droplets, and inducing hyperkeratinisation of the follicular infrainfundibulum, leading to increased sebum production and acne severity. In addition to local hormonal effects on sebaceous glands, systemic hormonal disorders play a role in triggering adult acne.
Additionally, stress has been recognised to exacerbate acne through hormonal fluctuations that increase sebum production. The skin microbiome, including C. acnes, coagulase-negative Staphylococcus, and fungal species, plays a role in maintaining skin health by balancing homeostatic relationships. While the proliferation of C. acnes has been associated with acne, it is the diversity and specific phylotypes of C. acnes that are more directly implicated in development of the condition.1,2,3
Pathophysiology
The pathophysiology of acne is a complex interplay of hyperkeratinisation, sebum overproduction, bacterial proliferation, and inflammation, which interact and amplify each other, leading to the formation of various acne lesions.1,3
Follicular hyperkeratinisation: This is the initial step in acne development. This process involves an abnormal increase in the production and desquamation of keratinocytes within the hair follicle. Under normal circumstances, keratinocytes are shed from the follicular epithelium in a controlled manner.
In acne, there is increased proliferation of keratinocytes, leading to a higher turnover rate. Instead of being shed, the keratinocytes stick together, forming a cohesive plug. This results in the blockage of the follicular ostium, creating a microcomedo. Androgens, particularly dihydrotestosterone (DHT), play a significant role in stimulating follicular keratinocyte proliferation. Other factors such as local cytokine milieu and genetic predisposition also contribute to this process.1,3,4
Sebaceous gland hyperactivity: Sebum production is primarily regulated by androgens, and individuals with acne typically have enlarged sebaceous glands and increased sebum secretion. Androgens, especially during puberty, stimulate the sebaceous glands to produce more sebum. This effect is mediated by androgen receptors on sebaceous gland cells. In acne patients, the composition of sebum may also be altered, with increased levels of squalene and decreased linoleic acid.
This change in lipid composition can promote comedogenesis and inflammation. Conditions such as polycystic ovary syndrome (PCOS), which is characterised by hyperandrogenism, can exacerbate acne by further increasing sebum production.1,3,4
C. acnes proliferation: The anaerobic bacterium C. acnes colonises the follicle, contributing to inflammation. C. acnes is a gram-positive anaerobic bacterium that resides within the pilosebaceous unit. It plays a central role in the inflammatory phase of acne. The blocked follicle provides an anaerobic environment conducive to C. acnes proliferation. C. acnes forms biofilms within the follicle, protecting it from the host immune response and antibiotics.
C. acnes produces lipases that hydrolyse triglycerides in sebum into free fatty acids, which are pro-inflammatory and comedogenic. C. acnes stimulates toll-like receptor 2 (TLR2) on keratinocytes and immune cells, triggering the release of pro-inflammatory cytokines (eg, interleukin (IL)-1, IL-8, tumour necrosing factor (TNF)-α, and chemokines, leading to an influx of inflammatory cells production. The immune response to C. acnes and its metabolic products leads to inflammation, resulting in the clinical manifestations of acne.1,3,4
Inflammation: Inflammation is both a consequence of and a contributing factor to the other pathogenic processes in acne. The activation of TLR2 by C. acnes results in the production of inflammatory mediators, including IL-1, IL-8, and TNF-α. These mediators recruit neutrophils and other immune cells to the site, leading to the formation of papules and pustules.
Neutrophils release enzymes and reactive oxygen species that contribute to follicular wall rupture and the spilling of follicular contents into the dermis, exacerbating inflammation. T-helper (Th)-1 and Th17 cells are also involved in the inflammatory response, producing additional cytokines such as interferon gamma (IFN-γ) and IL-17, which sustain inflammation. As inflammation resolves, the healing process can result in scarring, especially in cases of severe or nodulocystic acne. Atrophic scars form due to tissue loss, while hypertrophic scars and keloids result from excessive collagen deposition.1,3,4
The interactions among these four pathogenic factors create a cycle that sustains and exacerbates acne lesions. Environmental and lifestyle factors also play a significant role in modulating acne severity.
Clinical presentation
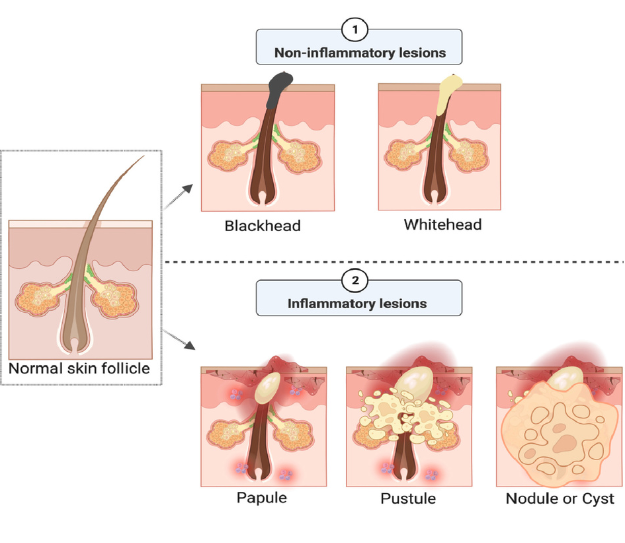
Acne affects the pilosebaceous units, predominantly on the face, chest, back, and shoulders. Severity and types of lesions vary widely, influencing the approach to diagnosis and treatment. Lesions are broadly categorised into non-inflammatory and inflammatory types.5
Non-inflammatory lesions: Comedones:
Open comedones3,5 or blackheads occur when the follicle is partially blocked by keratin and sebum. The open nature of the follicle allows the material to be oxidised by air, giving it a black appearance. Closed comedones or whiteheads are formed when the follicle is completely blocked, preventing oxidation and maintaining a white or flesh-coloured appearance.
Inflammatory lesions:
- Papules are small, raised, red bumps that may be tender to the touch. They indicate inflammation lesions3,5 within the follicle.
- Pustules are like papules, but contain visible pus at their tips, indicating a more intense inflammatory response.
- Nodules are large, solid, painful lesions that are deeper within the skin. They result from severe inflammation and often involve the rupture of the follicle wall, leading to a more extensive inflammatory reaction.
- Cysts are deep, painful, pus-filled lesions that can lead to significant scarring. They represent the most severe form of acne and are often associated with nodules (nodulocystic acne).
Acne typically affects areas with a high density of sebaceous glands. The face is the most common site, with lesions frequently appearing on the forehead, nose, cheeks, and chin. Acne on the chest and back can be more challenging to treat due to the thicker skin and larger sebaceous glands. The shoulders and upper arms are less commonly affected, but can still present with significant lesions.1,3,5 The severity of acne can be classified based on the number, type, and distribution of lesions.
Mild acne is predominantly comedonal with a few inflammatory lesions, limited to small areas on the face or trunk, with minimal risk of scarring.1,3,5
Moderate acne comprises an increased number of inflammatory lesions, including papules and pustules, greater involvement of the face, and may extend to the chest and back. There is potential for post-inflammatory hyperpigmentation and mild scarring.1,3,5
Severe acne displays numerous inflammatory lesions, including nodules and cysts, with extensive involvement of the face, chest, and back. There is a high risk of significant scarring and potential for psychological impact.1,3,5
Acne vulgaris is the most common type, making up 99 per cent of all acne cases, however, certain forms of acne present unique clinical features, including:1,3,5
- Acne conglobata is a severe form of nodulocystic acne characterised by interconnected abscesses and sinus tracts, leading to extensive scarring.
- Acne fulminans is an acute, severe form presenting with sudden onset
of ulcerative acne, systemic symptoms like fever, and elevated inflammatory markers. It often
requires systemic treatment.
- Mechanical acne is caused by physical factors such as friction, pressure, or occlusion. It is common
in athletes or individuals wearing tight clothing or equipment.
- Cosmetic acne is triggered by using certain skincare or cosmetic products that are comedogenic.
- Drug-induced acne is linked to medications such as corticosteroids, lithium, and certain antiepileptics. The distribution is typically monomorphic, with uniform lesion types.
Additional clinical considerations include:1,3,5
- Post-inflammatory hyperpigmentation (PIH): Dark spots that remain after the resolution of inflammatory lesions. PIH is more common in individuals with darker skin tones.
- Scarring, which can be atrophic (ice pick, boxcar, and rolling scars) or hypertrophic/keloidal. The risk increases with the severity and duration of acne.
- The psychological impact of acne can significantly affect an individual’s self-esteem and quality-of-life, leading to social withdrawal, anxiety, and depression.
Diagnosis
Diagnosing acne vulgaris involves a comprehensive approach that includes patient history, physical examination, and, in some cases, laboratory investigations. The goal is to accurately identify the type and severity of acne, differentiate it from other dermatological conditions, and determine any underlying factors that may contribute to its occurrence.1,6,7
A thorough patient history is important for diagnosing acne and identifying potential exacerbating factors. This includes documenting when the acne started and its progression over time. Noting the distribution and types of lesions, such as comedones, papules, pustules, nodules, and cysts, is important. Reviewing treatments previously used, their effectiveness, and any side-effects experienced helps in understanding the patient’s treatment history.
Assessing whether there is a family history of acne or related conditions can provide insights into genetic predispositions. Considering lifestyle factors such as diet, skincare routines, cosmetic use, stress levels, and exposure to potential triggers like occupational or environmental factors is important.
For female patients, noting any correlation between acne flare-ups and menstrual cycles can help identify hormonal influences. Identifying any medications that may contribute to acne, such as corticosteroids, lithium, or antiepileptics, is necessary for a comprehensive evaluation.1,6,7
A detailed physical examination is important to assess the type, distribution, and severity of acne lesions. This involves identifying the presence of non-inflammatory lesions, such as open and closed comedones, as well as inflammatory lesions, including papules, pustules, nodules, and cysts.
Mapping the affected areas is necessary to understand the distribution of acne. The severity of acne should be graded using standardised scales such as the Global Acne Grading System (GAGS) or the Leeds acne grading technique. Evaluating for signs of scarring, including post-inflammatory hyperpigmentation, atrophic scars, and hypertrophic or keloidal scars, is important.1,6,7
Acne vulgaris is diagnosed based on clinical criteria, which include the presence of characteristic lesions and their distribution. Key diagnostic features are:1,6,7
- Presence of comedones – open and closed comedones are hallmark features.
- Inflammatory lesions like papules, pustules, nodules, and cysts.
- Seborrheic areas – lesions predominantly occur in areas with a high density of sebaceous glands.
Laboratory tests are not typically required for diagnosing acne vulgaris, but may be considered in certain scenarios. Hormonal evaluation may be carried out in female patients with signs of hyperandrogenism (eg, hirsutism, irregular menstrual cycles), and assessing levels of androgens, luteinising hormone (LH), follicle-stimulating hormone (FSH), and prolactin can help identify underlying conditions like PCOS.
Microbiological tests are rarely indicated, but may be used to rule out bacterial folliculitis or fungal infections if the diagnosis is unclear. Skin biopsy is not routinely performed for acne, but may be indicated to exclude other diagnoses if the presentation is atypical.1,6,7
Differentiating acne from other skin conditions like rosacea, folliculitis, perioral dermatitis, seborrheic dermatitis, keratosis pilaris, and hidradenitis suppurativa is important for an accurate diagnosis.1,6,7
Treatment and management
The treatment and management of acne involves a multifaceted approach tailored to the type and severity of the condition, individual patient characteristics, and potential underlying factors.
Topical treatments are often the first-line of therapy for mild-to-moderate acne and can be used in combination with systemic treatments for more severe cases.8,9,10
- Topical retinoids are effective in normalising follicular keratinisation, promoting cell turnover, and reducing comedone formation. They are beneficial for both inflammatory and non-inflammatory lesions.
- Benzoyl peroxide, an antimicrobial agent, reduces C. acnes colonisation and has anti-inflammatory properties. It is often used in combination with topical antibiotics or retinoids to reduce the risk of antibiotic resistance.
- Topical antibiotics are commonly used to reduce bacterial load and inflammation. They are most effective when combined with benzoyl peroxide to mitigate resistance.
- Azelaic acid has antibacterial, anti-inflammatory, and comedolytic properties, making it useful for treating mild-to-moderate acne, particularly in patients with sensitive skin.
- Salicylic acid as a beta-hydroxy acid helps to exfoliate the skin and clear clogged pores, making it effective for comedonal acne.8,9,10
Systemic treatments are indicated for moderate-to-severe acne or when topical treatments have failed.8,9,10
- Oral antibiotics: Tetracyclines and macrolides are commonly used for their antibacterial and anti-inflammatory effects. They are typically prescribed for three-to-six months to reduce bacterial load and inflammation.
- Hormonal therapies: Oral contraceptives and anti-androgens are effective for female patients with hormonal acne. These therapies help regulate hormone levels, reduce sebum production, and decrease androgen-mediated skin effects.
- Oral isotretinoin: A potent retinoid, is reserved for severe, recalcitrant acne. It reduces sebaceous gland size and sebum production, normalises keratinisation, and has anti-inflammatory properties. It requires careful monitoring due to potential side-effects, including teratogenicity.
- Other systemic agents: In certain cases, systemic corticosteroids or dapsone may be used for specific forms of severe or refractory acne, such as acne fulminans or acne conglobata.8,9,12
The HSE treatment guidelines for acne are outlined in Table 1.11
| Mild Acne | |||
|---|---|---|---|
| Drug | Dose | Duration | Notes |
| First Line Treatment | |||
| Benzoyl peroxide (5 per cent w/w gel, Acnecide) | Apply twice weekly to affected area and slowly increase frequency as tolerated. Once tolerated, it can be applied every 24 hours | Can take up to 2 months to take effect. If effective, consider ongoing treatment. | This product may bleach hair and colour fabrics. Can cause photosensitivity. |
| Predominantly Comedones | |||
| Adapalene 0.1 per cent w/w gel or cream, (Differin) | Apply twice weekly to affected area to start and slowly increase frequency as tolerated. Once tolerated, it can be applied every 24 hours. | Review after 3 months. If effective, consider ongoing treatment. | Contraindicated in pregnancy. Apply after washing to dry skin. Can cause photosensitivity. |
| Adapalene can be used in combination with Benzoyl Peroxide or as a combination product | |||
| Adapalene 0.1 per cent/benzoyl peroxide 2.5 per cent gel (Epiduo) | Apply twice weekly to affected area to start and slowly increase frequency as tolerated. | Review after 3 months. If effective, consider ongoing treatment. | Contraindicated in pregnancy. Apply after washing to dry skin. This product may bleach hair and colour fabrics. Can cause photosensitivity. |
| Inflammatory Lesions (Pustules) | |||
| Clindamycin/benzoyl peroxide 10mg/g + 50mg/g Gel (Duac) | Apply twice weekly to affected area to start and slowly increase frequency as tolerated. Once tolerated, it can be applied every 24 hours. | Review and limit use to 3 months if possible (max 6 months) | Topical antibiotics should not be used alone nor in combination with oral antibiotics as there is an increased risk of antibiotic resistance. This product may bleach hair and colour fabrics. Can cause photosensitivity. |
|
Combination of inflammatory lesions and comedones 1st choice option |
|||
| Adapalene 0.1 per cent/benzoyl peroxide 2.5 per cent gel (Epiduo) | Apply twice weekly to affected area to start and slowly increase frequency as tolerated. Once tolerated, it can be applied every 24 hours. | Review after 3 months. If effective, consider ongoing treatment. |
Contraindicated in pregnancy. Apply after washing to dry skin. This product may bleach hair and colour fabrics. Can cause photosensitivity. |
| 2nd line option: if above causes severe irritation or for hyperpigmentation | |||
| Azelaic acid 15 per cent gel (Skinoren) | Apply every 12 hours. | Review after 3 months. If effective, consider ongoing treatment. |
|
| MODERATE ACNE NOT RESPONDING TO TOPICAL TREATMENT | |||
|---|---|---|---|
|
Seek specialist advice in pregnancy. Oral antibiotics should be reviewed if no response is seen after 12 weeks of therapy. *Oral and topical antibiotics should not be used in combination, as there is an increased risk of antibiotic resistance. |
|||
| Drug | Dose | Duration | Notes |
| 1st choice options | |||
| Lymecycline PLUS Topical agent from table above (except Duac*) |
408mg every 24 hours As above |
Review and limit use to 3 months if possible (6 months max) To be continued during and after for maintenance |
Contraindicated for children <12 years old and pregnancy Can cause photosensitivity Lymecycline 408mg equivalent to 300mg of tetracycline base |
| 2nd choice option | |||
| Doxycycline PLUS Topical agent from table above (except Duac*) |
100mg every 24 hours As above |
Review and limit use to 3 months if possible (6 months max) To be continued during and after for maintenance |
Not suitable for children <12 years old and pregnancy Can cause photosensitivity |
| OR | |||
| Trimethoprim | 200mg every 12 hours for 1 month then 300mg every 12 hours for 3 months |
Not suitable in pregnancy Caution re Stevens-Johnson syndrome/ toxic epidermal necrolysis Monitor full blood count when on trimethoprim long-term |
|
| PLUS Topical agent from table above (except Duac*) |
As above, to continue during and after oral antibiotic to prevent recurrence | ||
|
Please note: Minocycline is not routinely used for management of acne vulgaris, but if transcribing from secondary care advise patient of, and monitor for, abnormal LFTs, irreversible cutaneous pigmentation, and reversible drug-induced lupus. Minocycline can cause a blue-grey discoloration of inflamed skin. |
|||
| SEVERE ACNE | |||
|
Treatment as per moderate acne but refer for specialist advice. Consider referral for isotretinoin in the following instances: • Presence of nodulocystic acne • Failure of two different oral antibiotic courses (two 3–6-month courses) with appropriate topical agent • Presence of scarring |
|||
TABLE 1: HSE treatment guidelines for acne
Adjunctive treatments can enhance the effectiveness of pharmacologic therapies and address residual issues such as scarring. Superficial chemical peels using glycolic acid or salicylic acid can help improve comedonal acne and post-inflammatory hyperpigmentation.
Laser and light therapy options such as pulsed dye laser, intense pulsed light, and blue light therapy target C. acnes and reduce inflammation. Fractional lasers can improve scarring. Photodynamic therapy involves the application of a photosensitising agent followed by light activation to reduce sebaceous gland activity and bacterial load. Micro needling stimulates collagen production and can improve atrophic acne scars.3,8,9
Lifestyle and dietary modifications
While the role of diet in acne is still debated, certain dietary modifications may help some individuals. Reducing the intake of high glycaemic index foods may improve acne in some patients by decreasing insulin and IGF-1 levels. Limiting dairy products, particularly skimmed milk, has been suggested to reduce acne severity in some studies. Stress can exacerbate acne, so incorporating stress-reducing activities such as exercise, meditation, or yoga may be beneficial.3,8,9
Patient education and support
Educating patients about their condition and treatment is important for adherence and success. Advising on gentle, non-comedogenic skincare products and the importance of regular cleansing can help manage acne. Realistic expectations about the timeframe for seeing improvements and the importance of adherence to prescribed treatments should be discussed with the patient. Addressing the emotional and psychological impact of acne is important, as is providing resources or referrals for counselling if needed.3,8,9
Emerging therapies and outlook
Acne is a multifactorial skin disease that requires long-term treatment. A wide range of topical and systemic treatment options have been introduced over the years, however, many patients do not see satisfactory treatment results and experience difficulties adhering to treatment recommendations.
Research into new treatments for acne continues to evolve. Procedural treatments such as laser devices, photodynamic therapy, chemical peels, and intralesional injections present viable alternatives for reducing acne symptoms and scarring. Emerging therapies focus on novel biologics, bacteriophages, probiotics, and peptides, providing promising future options.
The main aim is to create more individualised, effective, and sustainable acne management strategies that tackle the root causes of acne rather than just addressing its symptoms. 12,13
References
1. Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. In StatPearls [Internet]. Treasure Island: StatPearls Publishing; 2024. Available at: www.ncbi.nlm.nih.gov/books/NBK459173/.
2. Wolkenstein P, Machovcová A, Szepietowski JC, et al. Acne prevalence and associations with lifestyle: A cross-sectional online survey of adolescents/young adults in seven European countries. J Eur Acad Dermatol Venereol. 2018;32(2):298-306.
3. Vasam M, Korutla S, Bohara RA. Acne vulgaris: A review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023;36:101578.
4. O’Neill AM, Gallo RL. Host-microbiome interactions and recent progress into understanding the biology of acne vulgaris. Microbiome. 2018;6(1):177.
5. Masterson K. Acne basics. Pathophysiology, assessment, and standard treatment options. Journal of the Dermatology Nurses’ Association. 2018;10(1S):S2-S10.
6. Tan AU, Schlosser BJ, Paller AS. A review of diagnosis and treatment of acne in adult female patients. Int J Womens Dermatol. 2017;4(2):56-71.
7. Oge’ LK, Broussard A, Marshall MD. Acne vulgaris: Diagnosis and treatment. Am Fam Physician. 2019;100(8):475-484.
8. Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006.e1-1006.e30.
9. Chovatiya R. Acne treatment. JAMA. 2021;326(20):2087.
10. Health Service Executive. Acne treatment. Dublin: Health Service Executive; 2023. Available at: www2.hse.ie/conditions/acne/treatment/.
11. Health Service Executive. Acne vulgaris-antibiotic prescribing. Dublin: Health Service Executive; 2023. Available at: www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/skin-soft-tissue/acne-vulgaris/.
12. Tobiasz A, Nowicka D, Szepietowski JC. Acne vulgaris-novel treatment options and factors affecting therapy adherence: A narrative review. J Clin Med. 2022;11(24):7535.
13. Kim H, Kim Y. Exploring acne treatments: From pathophysiological mechanisms to emerging therapies. International Journal of Molecular Sciences. 2024; 25(10):5302.











