







It is repeatedly emphasised in the literature that these conditions share many common features
CASE STUDY
The patient in this case study has been created based on an amalgamation of symptoms and circumstances common to recently referred patients. Patient A, as they will now be referred to, is in their 70s and was medically admitted for a number of weeks prior to referral to liaison psychiatry. At the time of our initial engagement, they had been given a new diagnosis of multiple myeloma and were quite unwell.
Although stabilising, the patient had experienced a number of medical issues (acute kidney injury, hypercalcaemia, hospital-acquired pneumonia, sepsis, low haemoglobin requiring transfusion) over the course of their admission. Patient A had required a brief ICU admission for intubation shortly after their initial admission date. Treatment at the time of referral involved chemotherapy, steroids, and regular dialysis.
In addition to poor engagement and confusion, the patient was experiencing agitation, impaired judgement, inattention, disturbed sleep, and affective lability. Subjectively, Patient A reported feeling intermittently very anxious and fearful, and was seeking frequent reassurance from staff and family members. There was a fluctuating pattern to their presentation, and it was a stark change from their baseline behaviour prior to hospital admission.
At baseline, Patient A had no cognitive impairment, had been fully independent, and was an active member in their society. Patient A had a history of depression and there was reference to a possible previous diagnosis of bipolar affective disorder (as per GP impression) – however, on assessment and through collateral, there was not sufficient evidence to support this.
Liaison psychiatry, also referred to as consultation-liaison psychiatry, is a specialised branch of psychiatry. These services are delivered in general or acute hospital settings and provide specialist medical expertise for conditions occurring at the intersection of mental and physical healthcare.1
In the acute hospital setting, referrals are commonly made by different medical teams/specialities on the basis that medically admitted patients are engaging poorly with treatment and rehabilitation, alongside elements of confusion or altered mental state, with an inference that a mental health condition is negatively impacting their engagement.
Such a presentation is more common among, but not confined to, the older adult population (>65 years). The liaison psychiatry consultation is often required to determine whether or not a mental health or other brain-related condition is impacting the patient’s ability to engage, and thus, negatively affecting their treatment and rehab potential.
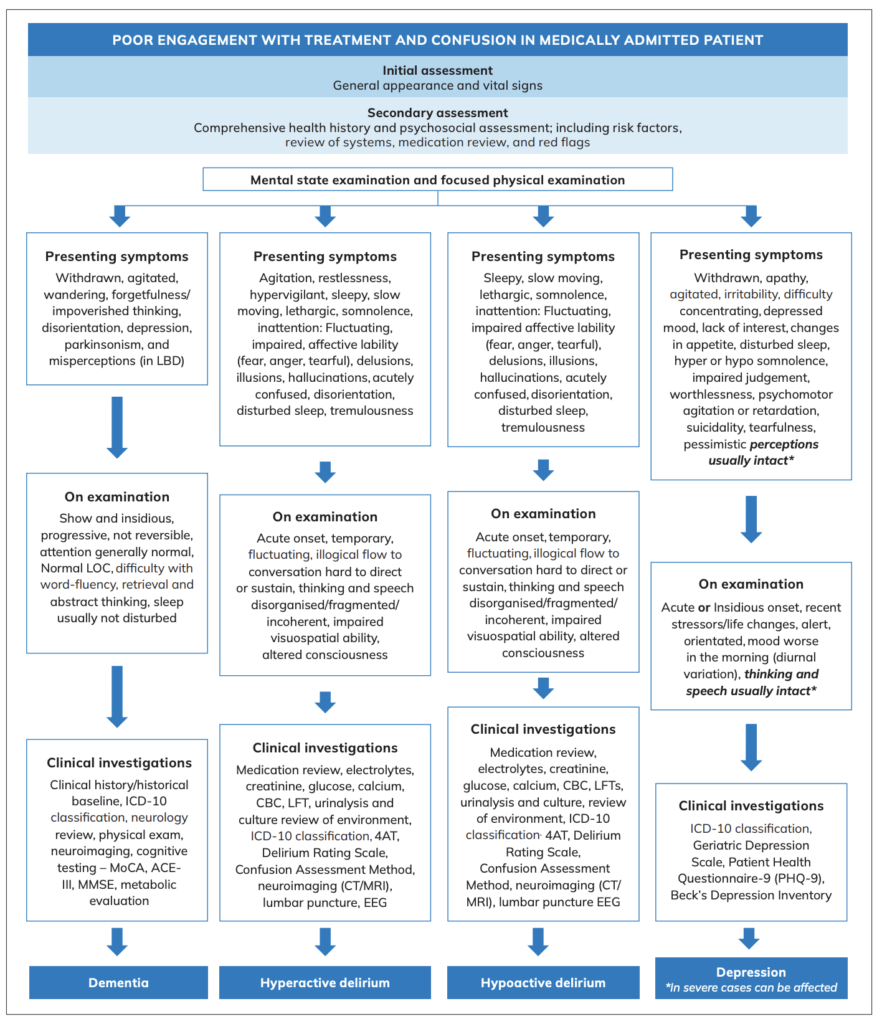
A diagnostic algorithm (Figure 1) was created in response to this common presentation, including the issues identified in the case study, to consider the typical differentials that are in mind when assessing a patient in such a situation. The overall aim was to produce a structured method that could be systematically followed to correctly diagnose the condition based on the patient’s information and clinical findings. Evidence was gathered to support the algorithm by completing an in-depth review of the pertinent literature and the clinical presentation itself.
In both clinical practice and in the literature, some of the possible differential diagnoses for this presentation include dementia, delirium (hyperactive or hypoactive), and depression.2,3,4,5,6,7 These four differentials were used to create the diagnostic algorithm (Figure 1).
Algorithms can assist practitioners in the development of a valid approach in differential diagnosis by indicating, in a structured manner, frequently encountered decisions in the diagnostic reasoning pathway. These are especially helpful when presentations have overlapping or similar symptomatology, as is the case for dementia, delirium, and depression.
Underlying pathological processes
The anatomical and physiological origins of psychiatric symptoms are less clearly defined than the origins of those in other major systems, with a less clear progression of cause and effect, which makes narrowing down the source of a mental disorder to any one component highly challenging.8 Engagement with treatment is not something that can be described specifically in terms of a pathological process. Similarly, the pathology of confusion is not easily defined. What is known is that confusion results in global impairment of brain function.
If looking through the lens of delirium, the main hypothesis is a reversible impairment of cerebral oxidative metabolism and multiple neurotransmitter abnormalities.9,10 The pathophysiology of dementia is broadly typified by the aggregation of misfolded proteins (such as amyloid-β plaques and neurofibrillary tangles in Alzheimer’s disease) and cerebrovascular disease.11 In terms of depression, confusion itself is not a particular cognitive deficit, but the components of confusion such as slow thinking and indecision are.12
Differential diagnosis: Dementia, delirium, and depression
Dementia is characterised by a decline in one or more cognitive domains of memory, language, learning new skills, executive function, complex attention, social cognition, and perceptual-motor skills.13 The majority of dementia syndromes are related to Alzheimer’s disease (60-80%). Other major syndromes include dementia with Lewy bodies, frontotemporal dementia, vascular dementia, and Parkinson’s disease with dementia.13
Behavioural and psychological symptoms of dementia or neuropsychiatric symptoms of dementia occur in up to 90 per cent of patients with the disorder.14 Neuropsychiatric symptoms can range from mild (depression, anxiety, irritability, and apathy) to severe (agitation, aggression, hallucinations, and disinhibition).
Delirium is a neuropsychiatric syndrome with an acute onset and a fluctuating course.15 It describes a reversible state of acute brain dysfunction, usually, but not solely, associated with medical and/or surgical conditions.16 Delirium can be described as hyperactive, hypoactive, or mixed – which presents with alternating symptoms of those found in hyperactive or hypoactive.2 Development of delirium is dependent on complex inter-relationships between vulnerable patients and several predisposing factors including exposure to noxious insults.17
One of the key features of depression is a disturbance of emotions or feelings. The diagnosis of depression depends on the presence of two core symptoms – persistent and pervasive low mood and a loss of interest or pleasure in usual activities.18
Depressive symptoms are considered to be of clinical significance when they interfere with normal activities and persist for at least two weeks.2,18 Depression can affect anyone, and can present as a confounding factor in elderly patients with functional and cognitive decline.3
Each of these diagnoses are detailed in the ICD-10 (International Classification of Diseases 10th Revision) Classification of Mental and Behavioural Disorders.19 Within the overarching diagnoses and further sub-classifications within them, there is a set of key features and/or criteria that should be present in order to meet the threshold for their diagnosis.
Following the diagnostic algorithm
It is repeatedly emphasised in the literature that dementia, delirium, and depression have many common features. Diagnosis can be further complicated by the fact that these presentations can coexist or be superimposed. Differentiating between them requires knowledge and awareness of the characteristic features of each condition.2,4,5,6,7,15
The shared symptoms exhibited by Patient A which could be considered across the differentials included agitation, impairment of judgement and attention, disturbed sleep, and affective lability. Although there are commonalities, there are also notable differences to be aware of.
These are important in directing the clinician towards the correct diagnosis because they identify pertinent positive and absent symptoms.8 It is therefore relevant to determine what other symptoms were present, and their potential aetiology, to determine what may be impacting the patient’s symptomatology.
In order to do this, as detailed in the diagnostic algorithm, this process begins with the completion of a comprehensive biopsychosocial assessment. This clinical interview style is a conversation with a purpose that allows the interviewer to gather a detailed and individualised patient history.8 The secondary assessment requires further investigation, which includes obtaining collateral, a focused systematic history, review of systems, medication review, identification of risk factors, and red flags.
Red flags are specific signs or symptoms that rule a diagnosis in or out. Collateral is often an invaluable tool in the assessment process and should never be overlooked. It is also worth noting that the assessment does not refer to a once-off interaction, rather it should be done over time in order to get diagnostic clarity.
The diagnostic algorithm (categorised under ‘presenting symptoms’) details the symptoms common to each of the potential differential diagnosis. When assessing the patient in this case, what stood out in regards to presenting symptoms was that this patient was at times acutely confused, with evidence of a fluctuating pattern to her behaviours and symptoms.
This indicated some red flags for a presentation of hyperactive or hypoactive delirium, which is noted to incur fluctuating and impaired attention alongside acute confusion.2,3,13,19,20
Moreover, rather than a pervasive depressed mood, there was affective lability personified in fear, anger, and tearfulness, which again supports a delirium presentation.2,4 Delirium is seen to be short and fluctuating, often worse at night and on waking2 – as was the case in this presentation.
Having considered the presenting symptoms, attention then turns to examination. In this formulation, it was of vital importance to have a defined history and collateral of this patient in regard to their baseline cognitive functioning, which as previously mentioned was not impaired prior to Patient A becoming acutely physically unwell.
Driven by logical decision-making, one could therefore conclude that the onset was acute rather than slow and insidious – as would be the case in dementia.2,4,15,19,20 It is important to note here that the onset of depression can be acute of insidious,2,15,20 so onset alone would not be a definitive diagnostic determinant across these differentials.
As per the algorithm, delirium can be divided into hyperactive and hypoactive. Hyperactive delirium is commonly associated with agitation, restlessness, and hypervigilance,2,3,4 while hypoactive delirium is normally related to sleepy, slow moving, lethargic, and somnolent presentations.2,3 This patient’s presenting symptoms, with reference to the diagnostic algorithm, led the assessor to believe that this presentation was more appropriately classed as a hyperactive delirium.
Clinical investigations
Following the diagnostic algorithm, consideration was then given to what clinical investigations would support the assumed diagnosis. The initial tests outlined in the diagnostic algorithm are indicated based on the knowledge that delirium may be precipitated by infections (eg, sepsis, pneumonia, urinary tract infections), dehydration, electrolyte imbalances, metabolic disturbances (eg, hypoxaemia, hypercarbia), side effects or interactions of anaesthesia and medication, or due to accumulated doses.15,21
This association can, at times, cause confusion as there is not always a marker or test that indicates delirium. The author feels that these precipitants are more widely accepted in the hospital setting.
There are, however, other origins of delirium which include:
- Sleep disturbances
- Immobilisation due to altered care setting
- Sensory impairment due to a change in environment and restricted access to usual aids
- Injury or severe pain.15,21
If severe enough, delirium can be detected during a clinical interview. Although there are no definitive quantitative markers available to diagnose delirium, qualitative tools such the 4AT,22 Delirium Rating Scale23 and the Confusion Assessment Method17 can be used. The 4AT is the most validated delirium detection tool used globally.7,11 Unfortunately, these tools are underused and healthcare providers often simply record the patient’s mental status in narrative.26
It has also been suggested in regard to clinical investigations of delirium that neuroimaging such as CT and MRI, lumbar puncture, and electroencephalogram can be used as diagnostic tools.27 However, these may not be necessary or cost-effective, and were not requested in this patient’s case.
Risks of misidentification/misdiagnosis
It is essential to differentiate between the aforementioned conditions, particularly if delirium is present, because this is an acute medical emergency that requires rapid assessment and management.3
Moreover, delays in investigating and treating underlying reasons for cognitive impairment, or initiating inappropriate treatment, can have serious consequences for an older person’s health and wellbeing while they are in hospital and on discharge.2 Depression is underdiagnosed despite it being one of the most common geriatric psychiatric disorders and a major risk factor for disability and mortality in elderly patients.28
In practice, hypoactive delirium is often missed or mistaken for depression or fatigue. In fact, delirium is under-diagnosed in almost two-thirds of cases or is misdiagnosed as depression or dementia.26 Delirium and depression can also cause cognitive changes that may be mistaken for dementia.15
Conclusion
This discussion highlights the similarities and differences across the diagnoses of dementia, hyperactive delirium, hypoactive delirium, and depression. Without detailed assessment and collateral, the symptoms presenting in this case could have been misattributed to the incorrect diagnosis.
The details and guided decision-making process facilitated by the diagnostic algorithm provides valuable guidance and education, especially given the delays and problems that appear to persist in the recognition and documentation of delirium by healthcare providers.
It is anticipated that the algorithm will be made available as a learning resource on the hospital’s intranet system, presented at upcoming education sessions, and, if feasible, developed into a learning module for nursing practice.









Leave a Reply
You must be logged in to post a comment.