Reference: June 2026 | Issue 6 | Vol 12 | Page 14
Arthritis refers to swelling, pain, and stiffness of one or more joints.1-3 It is an umbrella term which encompasses over 100 conditions.4 Axial spondyloarthritis is an inflammatory form of arthritis which primarily affects the joints of the axial skeleton. It typically affects the sacroiliac joints first. Although other joints – such as the shoulders and hips – as well as organs – such as the eyes, bowels, and skin – can become involved.5,6
Axial spondyloarthritis can be subclassified as radiographic or non-radiographic. In radiographic axial spondyloarthritis, which is more commonly referred to as ankylosing spondylitis (AS), damage to the joints of the axial skeleton is visible on x-ray. In non-radiographic axial spondylarthritis, x-rays do not show damage to the axial skeleton, yet the clinical presentation – such as symptoms, blood tests, and imaging – is suggestive of axial spondyloarthritis.1,6
The most common extra-articular manifestation of AS is uveitis (inflammation of the middle layer of the eye which includes the iris, ciliary body, and choroid), which affects up to a third of patients.7-9 This article will explore uveitis in AS, delving into the epidemiology, pathophysiology, clinical presentation, management, and prevention of both uveitis and AS – with particular attention given to the importance of collaboration between ophthalmologists and rheumatologists.
Epidemiology
It is estimated that around 0.1 per cent to 0.2 per cent of people in Ireland have AS.10 The estimated prevalence in Europe is 0.24 per cent, which appears to be slightly higher than the estimated global prevalence of 0.14 per cent.11 It is believed the increased prevalence of AS in areas such as Europe and North America is related to a greater percentage of the populations being HLA-B27-positive.12,13
Some studies have indicated that AS might be on the rise, but it has been noted that this could be due to improved recognition and increased confidence in diagnosing AS.14-16
In the UK, up to 90-95 per cent of individuals with AS are HLA-B27-positive.12,17 However, only approximately 5 per cent of HLA-B27-positive patients develop AS, which highlights the fact that AS is multifactorial, with multiple genetic and environmental risk factors.18-20
The onset of symptoms of AS is most commonly in the second and third decades of life. It is estimated that around 80 per cent of patients with AS experience symptoms by 30 years of age and 95 per cent experience symptoms by 45 years of age. Males are roughly twice as likely to be diagnosed with AS as females.21
Studies indicate that 25-35 per cent of people with AS will eventually develop uveitis. Of those, roughly 90 per cent will have acute anterior uveitis (AAU).22,23 For this reason, we will focus on AAU.
HLA-B27
Patients with AS who are HLA-B27-positive are significantly more likely to develop uveitis, including AAU, versus those who are HLA-B27-negative.24
The HLA-B27 allele (Human Leukocyte Antigen-B27), located on chromosome 6, is a major histocompatibility complex (MHC) class 1 molecule expressed on the surface of nucleated cells. HLA class 1 molecules, such as HLA-B27, present endogenous peptide antigens to CD8+ T cells to support immune surveillance.25 While the aetiology is unclear, possessing the HLA-B27 allele is a significant risk factor for developing several seronegative arthropathies, particularly AS. HLA-B27 has over 100 subtypes of which the association with AS varies.26
There are several hypotheses on how HLA-B27 is involved in the aetiology of AS. One hypothesis is that misfolding of the HLA-B27 molecule inside the cell leads to inflammatory pathways. Another hypothesis is that free heavy chains of HLA-B27 homodimers form a new MHC class II-like molecule, which leads to both innate and adaptive immune responses.
A third hypothesis is that arthritogenic peptides derived from microbes are presented by HLA-B27 to stimulate CD8+ T cells, which subsequently interact with HLA-B27-bound self-peptides, leading to chronic inflammation.27
Being HLA-B27-positive is also considered a risk factor, to a lesser degree, for several other conditions, including psoriatic arthritis and inflammatory bowel disease.26
Pathophysiology
AS is a complex immune-mediated condition of which the pathogenesis is not fully understood. The development of AS is heavily associated with the HLA-B27 allele which studies have suggested alters immune response and increases susceptibility to inflammation.28
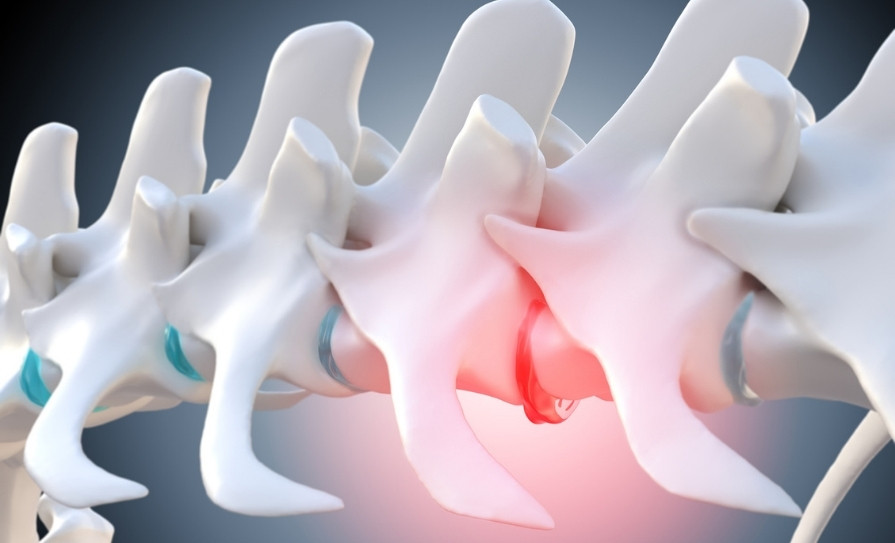
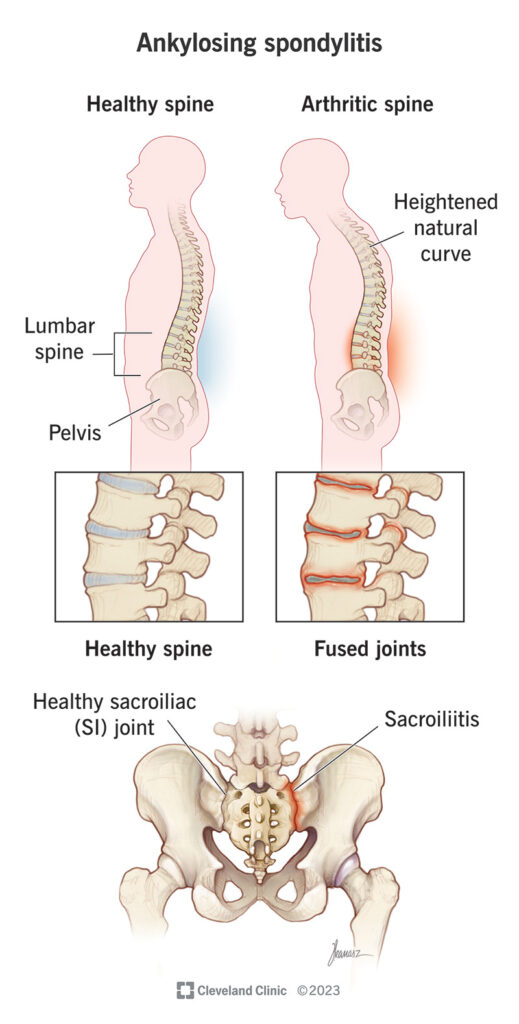
AS causes inflammation of the sites where ligaments and tendons join to bone, also known as enthesitis, as well as inflammation of the joints of the axial skeleton, particularly the sacroiliac joints. Eventually bone formation, in response to chronic inflammation, begins to fuse sections of vertebrae together, leading to stiffness and a hunched posture, as depicted in Figure 1.7
Signs of chronic inflammation such as sacroiliitis and sacroiliac joint fusion can be seen on x-ray.29 Patients can also experience temporary acute worsening of symptoms, known as flares, normally lasting days to weeks.30
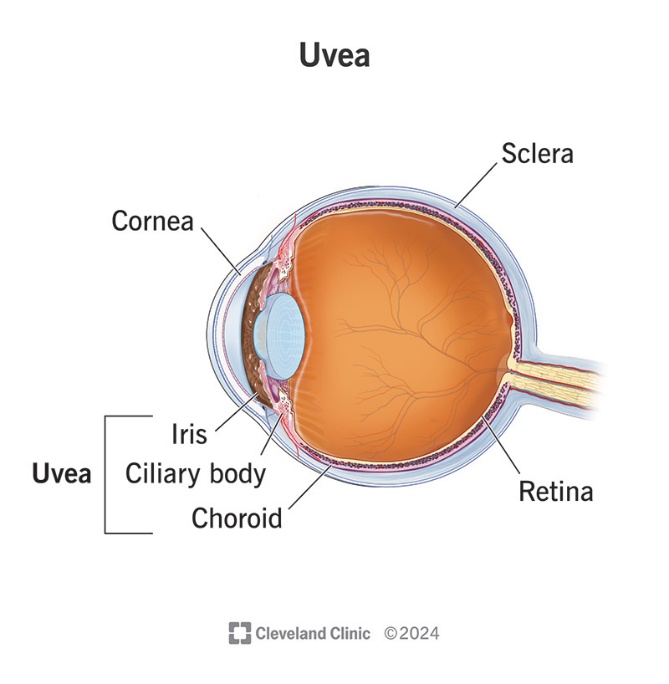
As previously mentioned, the most common extra-articular manifestation of AS is uveitis, most commonly AAU. The anatomy of the uvea is depicted in Figure 2. AAU in AS is typically acute and unilateral, with recurrent inflammation of the iris and ciliary body, although the reasons for this are not completely understood.32 This recurrent ocular inflammation represents a condition of interest to, and warranting collaboration between, both rheumatologists and ophthalmologists.
Clinical presentation
A typical presentation for AS is a male in their late 20s with chronic lower back pain and stiffness which improves with exercise but not rest and is worse in the mornings and nights, possibly disturbing sleep and causing fatigue.34
Acute anterior uveitis:
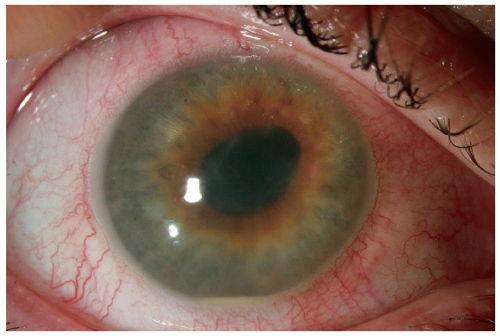
AAU typically may present as a red and painful eye with blurred vision, light sensitivity, and swollen conjunctiva. In more severe cases there may be pupil shape changes and/or white liquid accumulating at the bottom of the front of the eye referred to as hypopyon.35
Figure 3 is a slit-lamp photograph showing AAU with fibrin in the anterior chamber and a hypopyon in a HLA-B27-positive patient with AS.36
Diagnosis:
AS can be difficult to diagnose since it is a slowly developing condition and there is no definitive diagnostic test. Some of the factors considered as part of a diagnosis include symptoms, blood tests (such as ESR and CRP), genetic testing (HLA-B27), as well as imaging (such as MRI, x-ray, and ultrasound to assess for signs of joint inflammation).
According to the NHS, “a diagnosis of AS can usually be confirmed if an x-ray shows inflammation of the sacroiliac joints (sacroiliitis) with at least one of the following:37
1. At least three months of lower back pain that gets better with exercise and does not improve with rest.
2. Limited movement in the lumbar spine.
3. Limited chest expansion compared to expected for age and sex.
The diagnosis of AAU is a clinical diagnosis based on a careful history and slit-lamp examination. It is also a diagnosis of exclusion made after posterior ocular involvement has been ruled out.
A history suggestive of AAU may include eye pain, photophobia, eye redness, tearing, and blurred vision, as well as a prior history of similar symptoms.
Examination findings suggestive of AAU include a miotic pupil, perilimbal injection, irregular pupil shape (if synechiae present), cells/flare in anterior chamber, and hypopyon (in severe cases).32,39
Management
The management of AS involves both pharmacological and non-pharmacological treatments.
Non-pharmacological:
Staying active helps to maintain good posture and movement of the spine, as well as muscle strength and balance, which can help to reduce pain and stiffness of the spine, often experienced by those with AS.
Physiotherapists are highly beneficial for many patients with AS as they can advise on what exercises are appropriate and will work best for each patient and help them to come up with an exercise plan. Many AS patients benefit from physiotherapy programmes such as group exercise, individual exercise, and hydrotherapy. Consistent exercise is an important part of effective management for AS.40-42
Pharmacological:
NSAIDs are the preferred form of analgesia for pain associated with AS. Additionally, they can help to reduce some of the inflammation in affected joints. Examples of NSAIDs used to treat pain in ankylosing spondylitis include naproxen, ibuprofen, and diclofenac.
Normally one NSAID will be prescribed at the lowest dose which adequately relieves the patient’s symptoms. If the NSAID being used has been titrated to the maximum tolerated dose, and there is still inadequate pain relief, another NSAID should be considered.
When prescribing NSAIDs it is important to consider appropriate clinical assessment, ongoing management of risk factors, and gastroprotection.43 If NSAIDs are not suitable, paracetamol can also be considered.40
In patients who have responded inadequately to, or cannot tolerate NSAIDs, biological DMARDs can be considered. Treatment should be reviewed, usually after 12 weeks, and continued only if there is evidence of an adequate response. One way of monitoring response is patients’ self-reported symptoms severity which can be assessed using tools such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scale and Visual Analogue Scale (VAS). If there is inadequate response to treatment, an alternative TNF-alpha inhibitor can be considered.44
If a patient’s AS cannot be adequately managed with the above treatments, alternative pharmacological – for example, codeine, corticosteroid injections, monoclonal antibody treatment, or JAK inhibitors – or surgical management, for example, joint replacement – options may need to
be considered.40,44
While long-term disability from AS is uncommon, some people with the condition can develop severely restricted movement of the spine. Damage to joints, particularly the sacroiliac joints, can also cause pain and difficulty moving.
Additionally, there is an increased risk of uveitis, osteoporosis, and cardiovascular disease in those with AS. It is common for those with AS to also have certain conditions such as inflammatory bowel disease and psoriasis.45

Anterior uveitis:
The treatment of AAU involves managing inflammation and elevated intraocular pressure (IOP) and attempting to break synechiae. Inflammation is generally managed with intensive topical steroids such as G prednisolone acetate or dexamethasone. In more severe presentations, subconjunctival corticosteroid injections, for example, dexamethasone or betamethasone, may be considered.
Elevated IOP can be managed with topical antihypertensive drops, eg, certain beta-blockers, alpha agonists, and carbonic-anhydrase inhibitors. Miotics and prostaglandins are relatively contraindicated in an inflamed eye since they can potentially worsen the inflammation.
Topical mydriatics such as phenylephrine, tropicamide, and cyclopentolate are used to break synechiae by dilating the pupil. If adequate pupil dilation cannot be achieved using topical agents, subconjunctival injection of a mydriatic such as mydricaine can be considered.39,46
The most important potential complication of AU is vision loss and blindness, potentially due to complications such as synechiae, cataracts, and glaucoma.35
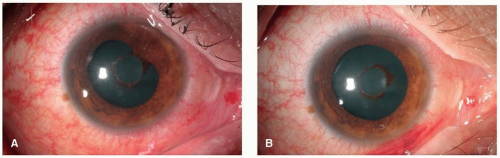
Figure 5 shows an eye with anterior uveitis.
A: There is diffuse conjunctival injection with ciliary flush and posterior synechiae.
B: After a few days of topical steroids and cycloplegic medication, there is less injection, and the posterior synechiae released.36
In a patient under 45 years old with a history of joint pain, referral for HLA-B27 testing is recommended.39 Additionally, effective management of AS might reduce the recurrence and severity of associated anterior uveitis episodes.47
Prevention
The SENTINEL study, published in 2016, was a multicentric observational prospective study conducted in Spain which included 798 patients (59 per cent male; mean age 45 years) who had experienced more than one episode of AU separated by at least three months and had no previous diagnosis of spondyloarthropathy.
The study found that a significant percentage of HLA-B27-positive patients with recurrent AU had undiagnosed axial or peripheral spondyloarthritis based on the Assessment of SpondyloArthritis International Society (ASAS) criteria.48
In this regard, it appears that appropriate risk stratification may allow for improved recognition of AS in HLA-B27-positive patients with recurrent AU. Studies have also suggested that AAU might precede the onset of AS symptoms by up to three years.26,49 These studies highlight the importance of collaboration between ophthalmologists and rheumatologists in both the prevention and management of uveitis in AS by increasing diagnosis and allowing for earlier treatment.
Summary
This has been a brief overview of AS, AAU, and the relationship between the two. AS is an inflammatory arthritis which affects thousands of people in Ireland. It is a significant risk
factor for AAU. By not viewing AAU in ‘eye-solation’, ophthalmologists can aid in the diagnosis of AS, potentially improving prognosis for both conditions.
This article is intended for educational purposes only. Clinicians should consult specialists and local guidelines as appropriate before making any decisions about patient care.
References:
- NHS. Overview – Arthritis [Internet]. NHS. 2022. Available at: www.nhs.uk/conditions/arthritis/
- Johns Hopkins Medicine. Arthritis [Internet]. Johns Hopkins Medicine. 2023. Available at: www.hopkinsmedicine.org/health/conditions-and-diseases/arthritis.
- Arthritis: MedlinePlus Medical Encyclopedia [Internet]. medlineplus.gov. Available at: https://medlineplus.gov/ency/article/001243.htm
- Arthritis Foundation. Types of arthritis pain [Internet]. www.arthritis.org. Available at: www.arthritis.org/health-wellness/healthy-living/managing-pain/understanding-pain/sources-of-arthritis-pain
- Axial Spondyloarthritis: Symptoms and treatment [Internet]. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/24843-axial-spondyloarthritis
- Overview of spondyloarthritis: What you need to know | SPONDYLITIS.ORG [Internet]. Spondylitis Association of America – ankylosing spondylitis. Available at: https://spondylitis.org/about-spondylitis/overview-of-spondyloarthritis/
- Mayo Clinic. Uveitis: Symptoms and causes [Internet]. Mayo Clinic. 2023. Available at: www.mayoclinic.org/diseases-conditions/uveitis/symptoms-causes/syc-20378734
- Uveitis: Symptoms, causes, treatment and types [Internet]. Cleveland Clinic. 2024. Available at: https://my.clevelandclinic.org/health/diseases/14414-uveitis
- Sharma SM, Jackson D. Uveitis in the spondyloarthopathies. Best Practice & Research Clinical Rheumatology. 2017 Dec;31(6):846-62.
- Pharmacist I. AS: Spotlight on ankylosing spondylitis – Irish Pharmacist [Internet]. Irish Pharmacist. 2022 [cited 2026 Apr 2]. Available at: https://irishpharmacist.ie/clinical/spotlight-on-ankylosing-spondylitis/
- Dean LE, Jones GT, MacDonald AG, et al. Global prevalence of ankylosing spondylitis. Rheumatology. 2013 Dec 9;53(4):650-7.
- Sheehan NJ. The ramifications of HLA-B27. JRSM. 2003 Dec 31;97(1):10-4.
- Sen R, Goyal A, Bansal P, Hurley JA. Seronegative spondyloarthropathy. PubMed. Treasure Island (FL): StatPearls Publishing; 2020. Available at: www.ncbi.nlm.nih.gov/books/NBK459356/
- Jung YS, Cho SK, Choi SR, et al. Evolving trends in the prevalence and treatment of ankylosing spondylitis in Korea from 2010 to 2023: A population-based study. Scientific Reports. 2025 Jan 20;15(1).
- Crossfield SSR, Marzo-Ortega H, Kingsbury SR, et al. Changes in ankylosing spondylitis incidence, prevalence, and time to diagnosis over two decades. RMD Open. 2021 Dec;7(3):e001888.
- Curtis JR, Winthrop K, Bohn RL, et al. The annual diagnostic prevalence of ankylosing spondylitis and axial spondyloarthritis in the United States using Medicare and MarketScan databases. ACR Open Rheumatology [Internet]. 2021 Sep 22;3(11):743-52. Available at: www.ncbi.nlm.nih.gov/pmc/articles/PMC8593814/
- Rath L. HLA-B27 gene and arthritis Arthritis Foundation [Internet]. www.arthritis.org. 2022. Available at: www.arthritis.org/diseases/more-about/hla-b27-gene-and-arthritis
- Ankylosing spondylitis : Symptoms, diagnosis and treatment [Internet]. Johns Hopkins Arthritis Center. 2016. Available at: www.hopkinsarthritis.org/arthritis-info/ankylosing-spondylitis/
- NHS. Ankylosing spondylitis: Causes [Internet]. www.nhs.uk. 2018. Available at: www.nhs.uk/conditions/ankylosing-spondylitis/causes/
- Hwang MC, Ridley L, Reveille JD. Ankylosing spondylitis risk factors: A systematic literature review. Clinical Rheumatology. 2021 Mar 22;40(8).
- Ankylosing Spondylitis: OrthoInfo – AAOS [Internet]. www.aaos.org. 2021. Available at: https://orthoinfo.aaos.org/en/diseases–conditions/ankylosing-spondylitis/
- Zeboulon N, Dougados M, Gossec L. Prevalence and characteristics of uveitis in the spondyloarthropathies: A systematic literature review. Annals of the Rheumatic Diseases, 67, 955-959.
- Clinic C. Why ankylosing spondylitis causes eye pain [Internet]. Cleveland Clinic. Cleveland Clinic; 2022. Available at: https://health.clevelandclinic.org/eye-pain-ankylosing-spondylitis.
- Khan MA. HLA-B27 and its pathogenic role. JCR: Journal of Clinical Rheumatology. 2008 Feb;14(1):50-2.
- HLA-B27: An overview | ScienceDirect Topics [Internet]. www.sciencedirect.com. Available at: www.sciencedirect.com/topics/medicine-and-dentistry/hla-b27
- Parameswaran P, Lucke M. HLA B27 syndromes [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020. Available at: www.ncbi.nlm.nih.gov/books/NBK551523/
- Braun J, Sieper J. Fifty years after the discovery of the association of HLA B27 with ankylosing spondylitis. RMD open [Internet]. 2023 Aug 1;9(3):e003102. Available at: https://pubmed.ncbi.nlm.nih.gov/37652557/
- Kim SH, Lee S-H. Updates on ankylosing spondylitis: Pathogenesis and therapeutic agents. J Rheum Dis [Internet]. 2023 [cited 2026 Apr 8];30(4):220–33. Available at: www.jrd.or.kr/journal/view.html?uid=1553&vmd=Full
- Imaging of musculoskeletal disorders: Spondyloarthropathy [Internet]. Available at: www.radiologymasterclass.co.uk/tutorials/musculoskeletal/imaging-joints-bones/ankylosing-spondylitis-xray
- Examining flares in spondyloarthritis, Spondylitis Association of America – ankylosing spondylitis 2025. Available at: https://spondylitis.org/spondylitis-plus/examining-flares-in-spondyloarthritis/.
- Cleveland Clinic. What is ankylosing spondylitis? [Internet]. Cleveland Clinic. 2023. Available at: https://my.clevelandclinic.org/health/diseases/ankylosing-spondylitis
- Rademacher J, Poddubnyy D, Pleyer U. Uveitis in spondyloarthritis. Therapeutic advances in musculoskeletal disease. 2020 Jan;12:1759720X2095173.
- Clinic C. Uvea: Definition, parts, function, and common conditions [Internet]. Cleveland Clinic. 2024. Available at: https://my.clevelandclinic.org/health/body/uvea
- NHS Choices. Symptoms: Ankylosing spondylitis [Internet]. NHS. 2023. Available at: www.nhs.uk/conditions/ankylosing-spondylitis/symptoms/
- Uveitis: Symptoms, causes, treatment, and types [Internet]. Cleveland Clinic. 2017 [cited 2026 Apr 4]. Available at: https://my.clevelandclinic.org/health/diseases/14414-uveitis#symptoms-and-causes
- UFO Themes. Anterior uveitis [Internet]. Ento Key. 2019 [cited 2026 Apr 8]. Available at: https://entokey.com/anterior-uveitis-4/
- NHS. Ankylosing spondylitis: Diagnosis [Internet]. 2018. Available at: https://www.nhs.uk/conditions/ankylosing-spondylitis/diagnosis/
- How axSpA is diagnosed – Axial Spondyloarthritis (AS) support programme. Arthritis Australia [Internet]. 2021. Available at: https://myas.org.au/article/your-axspa-diagnosis/how-axspa-diagnosed
- Clinical guideline for the treatment of anterior uveitis [Internet]. Available at: www.rveeh.ie/app/uploads/2022/06/Clinical-Guideline-Anterior-Uveitis-Final-2022.pdf
- NHS. Ankylosing spondylitis: Treatment [Internet]. 2017. Available at: www.nhs.uk/conditions/ankylosing-spondylitis/treatment/
- Exercise [Internet]. National Axial Spondyloarthritis Society. Available at: https://nass.co.uk/managing-my-as/exercise/
- Quality statement 3: Physiotherapy – Spondyloarthritis quality standards NICE [Internet]. Available at: www.nice.org.uk/guidance/qs170/chapter/quality-statement-3-physiotherapy
- Recommendations – spondyloarthritis in over 16s: Diagnosis and management guidance NICE [Internet]. Available at: www.nice.org.uk/guidance/NG65/chapter/Recommendations#pharmacological-management-of-spondyloarthritis.
- Team A. Management of axial spondylitis [Internet]. Available at: https://gpnotebook.com/en-IE/pages/palliative-care/seronegative-arthritis/management-of-axial-spondylitis
- NHS Choices. Complications: Ankylosing spondylitis [Internet]. NHS. 2019. Available at: www.nhs.uk/conditions/ankylosing-spondylitis/complications/
- Uveitic glaucoma: Pathophysiology and management. American Academy of Ophthalmology. 2008. Available at: www.aao.org/eyenet/article/uveitic-glaucoma-pathophysiology-management
- Guignard S, Gossec L, Salliot C, et al. Efficacy of tumour necrosis factor blockers in reducing uveitis flares in patients with spondylarthropathy: A retrospective study. Annals of the Rheumatic Diseases. 2006 May 25;65(12):1631-4.
- Juanola X, Loza Santamaría E, Cordero-Coma M. Description and prevalence of spondyloarthritis in patients with anterior uveitis: The SENTINEL interdisciplinary collaborative project. Ophthalmology [Internet]. 2016 Aug 1;123(8):1632-6. Available at: www.sciencedirect.com/science/article/pii/S016164201600347X
- D’Ambrosio EM, La Cava M, Tortorella P, et al. Clinical features and complications of the HLA-B27-associated acute anterior uveitis: A metanalysis. Seminars in Ophthalmology. 2016 Jul 12;32(6):689-701.