NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
A comprehensive overview of the presentation and management of type 2 diabetes.
Diabetes is the most common chronic metabolic disease and a major source of morbidity and mortality. Type 2 diabetes mellitus (T2DM) is the most prevalent form, accounting for around 90 per cent of cases worldwide. Figures released by the International Diabetes Federation (IDF) in December 2021 show that more than half a billion adults globally are living with diabetes. This is a rise of 16 per cent (74 million) since the previous IDF estimates in 2019. Worldwide, 537 million adults aged 20-79 years are living with diabetes, and 541 million adults have pre-diabetes, which places them at high-risk of developing T2DM. The prevalence of diabetes worldwide is growing at an alarming rate, and is predicted to rise to 643 million by 2030, and 784 million by 2045. The diabetes epidemic is unfolding because of increasing obesity rates, sedentary lifestyles and an ageing population.1
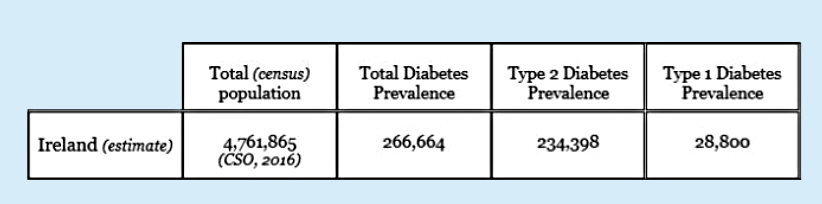
There is still no National Diabetes Registry in Ireland, therefore national estimates are not fully accurate. The figures provided by Diabetes Ireland (Table 1, January 2022) use data modelled from the Scottish Diabetes Register. In Scotland, the prevalence of diabetes was 5.6 per cent of the total census population in 2020. Table 1 estimates the total diabetes prevalence in Ireland at approximately 266,664 people. The prevalence of T2DM is estimated at 234,398 people (87.9 per cent of the total diabetes population) and type 1 diabetes at 28,800 (10.8 per cent of the total diabetes population), based on the Scottish prevalence. The true prevalence of T2DM in Ireland, however, is likely to be higher, as hyperglycaemia develops gradually, and at the early stage many cases go undiagnosed.1
According to the 2015 Irish Longitudinal Study on Ageing (TILDA), 10 per cent of adults aged 50 and over in Ireland have T2DM, rising to 16 per cent in those aged 80 and over. The TILDA study revealed that 1:10 people with diabetes in this population are undiagnosed, and that a further 5.5 per cent of the older population have pre-diabetes, which puts them at an increased risk of developing T2DM in the future.2 The study also found that T2DM is more common in men (12 per cent) than women (7 per cent), and those with a self-reported history of hypertension, high cholesterol, and being centrally obese, while having low levels of physical activity also has a strong correlation with both diabetes and pre-diabetes.2
The IDF Atlas 2021 ranked Ireland seventh in the world for diabetes-related health expenditure per person.3 The economic burden of diabetes on the Irish healthcare system is a major challenge for Government and the HSE. National estimates comparing health-service use between people over 50 years of age with and without diabetes (2009-2011) show that diabetes was associated with an 87 per cent increase in outpatient visits, a 52 per cent increase in hospital admissions, and a 33 per cent increase in emergency department attendances.1
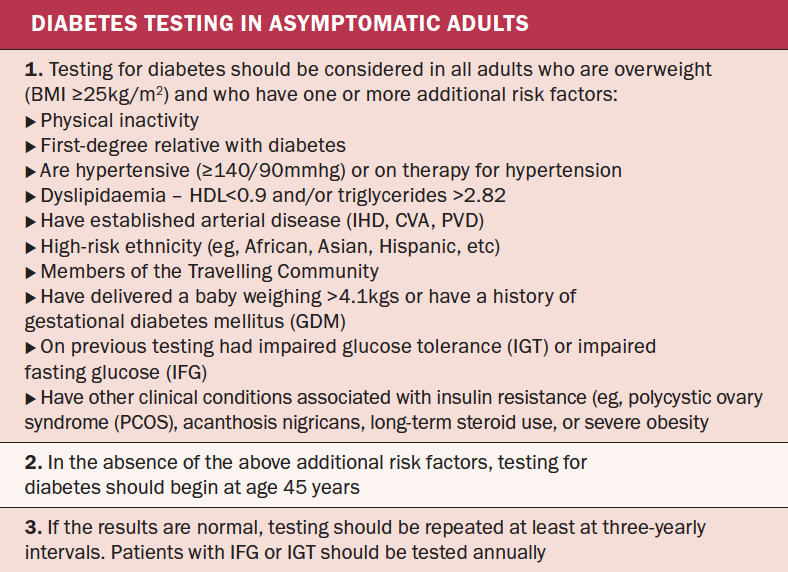
TABLE 2: Criteria for testing for diabetes in asymptomatic adults. Source: ICGP (2016)10
The CODEIRE study (2006) stated that costs associated with diabetes in Ireland consume between 4-to-6 per cent of annual healthcare expenditure. If the same percentage (4-to-6 per cent) was to be applied to the Irish healthcare expenses in 2019, the costs associated with diabetes would have been as high as €1.2 billion to €1.4 billion, with approximately 50 per cent of the costs associated with hospitalisations and treatment of complications. With the growing prevalence of diabetes in Ireland, comprehensive economic data is required to ensure that appropriate resources are allocated to the management of the disease.4
Pathophysiology
T2DM is an insulin-resistance condition with associated beta-cell dysfunction. It occurs when blood glucose levels are too high (hyperglycaemia) due to insufficient insulin production, or when the insulin that is produced by the pancreas is not working effectively. T2DM results from an interaction between genetic and environmental factors, and ranks high on the international health agenda as a global pandemic, and as a threat to human health and global economies.5
In T2DM, the response to insulin is diminished, and this is defined as insulin resistance. During this state, insulin is ineffective and is initially countered by an increase in insulin production to maintain glucose homeostasis. However, as the disease progresses, beta cells change and insulin secretion is unable to maintain glucose homeostasis, producing hyperglycaemia, resulting in T2DM.6
T2DM is most commonly seen in people over the age of 40. However, it is also now increasingly seen in children, adolescents, and younger adults due to rising levels of obesity, physical inactivity, and energy-dense diets.6 Most patients with T2DM are obese or have a higher body fat percentage, distributed predominantly in the abdominal region. This adipose tissue promotes insulin resistance through various inflammatory mechanisms, including increased FFA release and adipokine dysregulation. Lack of physical activity in people with hypertension or dyslipidaemia also increases the risk of developing T2DM.6
Chronic hyperglycaemia can cause damage to various organ systems, leading to the development of disabling and life-threatening health complications, most prominent of which are microvascular (retinopathy, nephropathy, and neuropathy) and macrovascular complications, leading to a two-to-four-fold increased risk of cardiovascular disease.6
Risk factors
Obesity: Obesity and T2DM are closely linked and are increasing in prevalence worldwide. Both chronic conditions have a multisystem impact and are associated with increased mortality and cardiovascular risk. The mechanisms linking obesity and T2DM are complex and still being understood. It is thought to involve a combination of adipose tissue release of excess circulating fatty acids, glycerol, hormones and pro-inflammatory cytokines, impairing cellular insulin signalling and increasing insulin resistance; and chronically raised lipid levels leading to impaired islet beta-cell function and lower levels of insulin production.7
Smoking, high alcohol consumption, and reduced physical activity: These are key factors that contribute to obesity and insulin resistance.
Age: Although T2DM can occur at any age, older age from >40 years is associated with the progressive reduction in glucose tolerance, partly owing to the gradual decrease in responsiveness of beta-cells to carbohydrates.7
Genetics: Other risk factors include first-degree relatives of someone with diabetes, and women with GDM or PCOS, which increases the risk of impaired glucose regulation. The risk of first-degree relatives of people with T2DM developing the condition is 40 per cent compared with just 6 per cent for the rest of the general population.7
Ethnicity: T2DM is two-to-four times more likely in people of south-Asian, Afro-Caribbean or black-African descent than people of white-European origin. Migration of various ethnic subgroups has led to a change in dietary habits, with a higher consumption of calories and fat than in their countries of origin; hence the prevalence of diabetes is often higher in immigrant communities than in their country of origin.7
Inflammation: Systemic inflammation also contributes to insulin resistance as an improvement in inflammatory markers, such as C-reactive protein and interleukin-6, are linked to an improvement in beta-cell function.7
Signs and symptoms
Symptoms of T2DM originate from persistent hyperglycaemia and the impaired ability to use glucose as fuel, and include polyuria, nocturia, polydipsia, fatigue, and weight loss. A person with diabetes may also experience other symptoms, such as blurred vision, reduced sensations or pain in the hands and feet, along with recurrent genitourinary infections.7
Owing to insulin deficiency and altered energy metabolism, diabetes increases the risk of developing hyperosmolar hyperglycaemic states and ketoacidosis, both of which are life-threatening emergencies that require prompt hospital treatment. Diabetic ketoacidosis is less common in people with T2DM, because most people are insulin resistant rather than insulin deficient.7
Criteria for testing for diabetes in asymptomatic adult individuals
T2DM has a long pre-clinical phase and may be asymptomatic until well after long-term microvascular and macrovascular complications have occurred. T2DM can be detected before the onset of symptoms and clinical signs by identifying people who are at risk and performing diagnostic testing (see Table 2). The onset of T2DM is subtle and early detection in general practice requires clinical suspicion combined with systematic and opportunistic findings. Early identification of patients and initiation of treatment can reduce the development of complications, and therefore testing for diabetes in asymptomatic patients with risk factors associated with the development of diabetes is recommended.10
Diagnosis
A thorough medical history, physical examination and investigative tests are required to form a diagnosis for T2DM. The patient’s history will include an assessment for risk factors such as a family history of diabetes, ethnicity, and increased age >40 years old. The patient’s vital signs and height, weight, and BMI should be recorded. The skin should be examined for wounds and signs of infection. Pulses should be palpated to examine for peripheral arterial disease, and microfilament testing to determine the presence of peripheral neuropathy. The eyes should be examined with an ophthalmoscope and assessed for retinopathy. A series of blood tests will be carried out including a fasting blood glucose. Urinary glucose should not be used as a diagnostic test owing to its low sensitivity. Additional diagnostic tests are often required, such as ‘GAD’ autoantibody tests or C-peptide tests, to distinguish between T1DM and T2DM. Other types of DM must also be excluded, such as maturity-onset diabetes of the young, which is characterised by impaired insulin secretion with minimal or no defects in insulin action resulting from genetic defects in beta-cell function.7
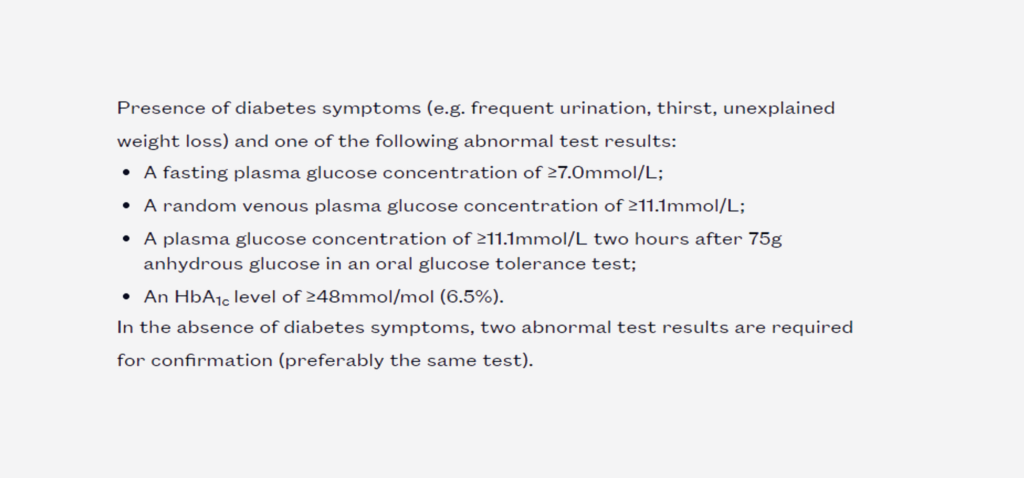
Diagnosis can be made when fasting plasma glucose is ≥7.0mmol/L or random plasma glucose is ≥11.1mmol/L in the presence of symptoms, such as frequent urination, thirst, and unexplained weight loss.7, 8
The oral glucose tolerance test (OGTT) can also be used as a diagnostic tool, where a diagnosis is made if a plasma glucose level of ≥11.1mmol/L is measured two hours after the ingestion of a 75g glucose solution. The OGTT has largely been replaced by the HbA1c test, and is now mainly used in the diagnosis of GDM. An HbA1c result of 48mmol/mol (6.5 per cent) is recommended as the threshold for diagnosing diabetes.7, 8
In an asymptomatic person, diagnosis should be confirmed with a repeat HbA1c or plasma glucose test, preferably using the same test. However, if both HbA1c or plasma glucose measurements are in diabetic range, a diagnosis can be made. If only one measurement is in range, a second abnormal result using the same test is required to confirm the diagnosis.7,8
There are patient groups in whom HbA1c is inappropriate for diagnosis, including:
Children;
Pregnant women;
People who are taking medicines such as steroids or antipsychotics that can cause an acute glucose;
People with acute pancreatic damage;
People with haematological conditions that may influence HbA1c and its measurement, eg, haemoglobinopathies, decreased erythropoiesis/administration of erythropoietin, erythrocyte destruction, alcoholism, chronic kidney disease, and chronic opioid use.7
FIGURE 1: The International Diabetes Federation and World Health Organisation criteria for T2DM8,9
ANNUAL REVIEW10
Along with the areas monitored at the regular review, surveillance of the following should also be carried out annually, according to the ICGP guidelines:
SYMPTOMS
Ischaemic heart disease, peripheral vascular disease – neuropathy, erectile dysfunction. All patients with symptoms that might reflect vascular disease, particularly ischaemic heart disease, should be investigated
Visual acuity and retinal review by ophthalmologist/ retinal screening programme
KIDNEY
Renal damage, albumin excretion, serum creatinine and calculate EGFR
ARTERIAL RISK
Blood glucose, blood pressure, blood lipids, and smoking status, ECG
ATTENDANCES
Podiatry/dietitian/other as indicated
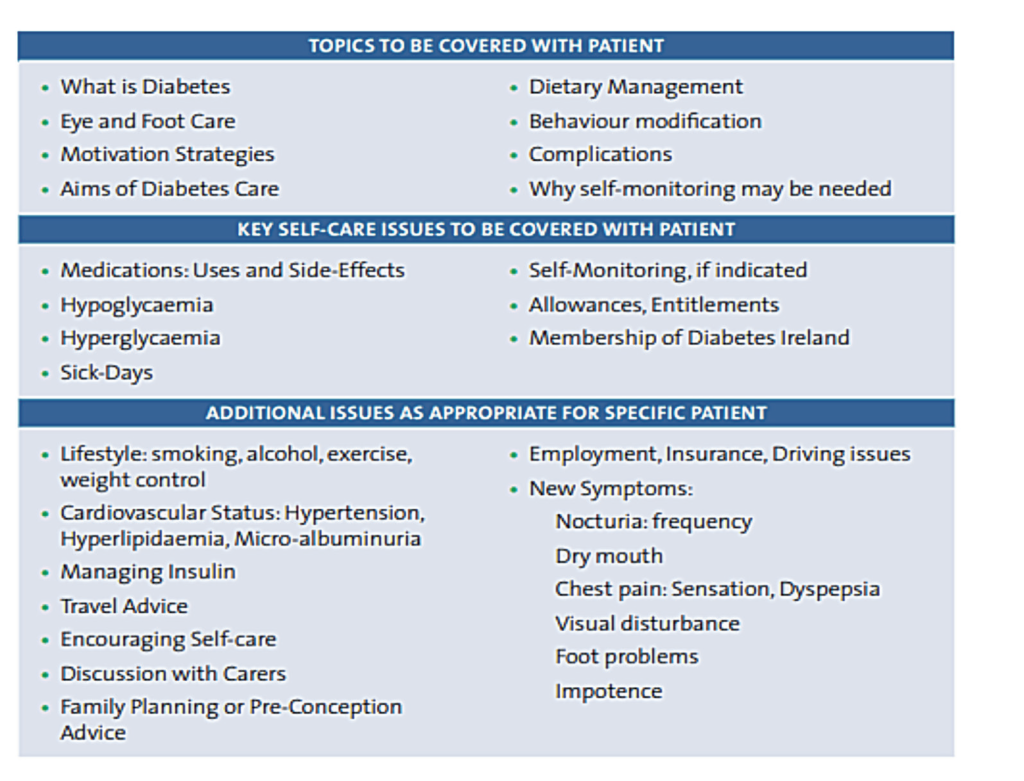
TABLE 3: Structured education programme tailored to the patient’s individual needs10
Treatment and management
The introduction of the HSE’s Cycle of Care for diabetes in October 2015 was the first step in the provision of reimbursement for structured diabetes care in general practice. To support the implementation of the Cycle of Care, A Practical Guide to Integrated Type 2 Diabetes Care was updated by GP Dr Velma Harkins on behalf of the ICGP with the support of the HSE’s National Clinical Programme for Diabetes (2016). The Programme then published its Model of Integrated Care for Patients with Type 2 Diabetes18 document in 2018, which outlines the framework for the delivery of evidence-based practice guidelines to people with T2DM in Ireland.
Under the HSE’s National Integrated Model of Care,18 patients with uncomplicated T2DM are seen three times a year in primary care in a structured fashion. Visits are every four months with an annual review. Patients who develop complications are referred from primary to secondary or tertiary care for an expert specialist opinion and their care will become shared between primary and secondary or tertiary care. These patients will be seen at least once a year in secondary care for their annual review or more frequently according to the severity of the diabetes-related complication and up to twice a year in primary care at four-monthly intervals.10
Diabetes care should encompass patient education, dietary and lifestyle advice, management of cardiovascular risk, skin and foot care, as well as detection and management of long-term complications. Patients with T2DM should be encouraged to eat high-fibre, low glycaemic index sources of carbohydrates such as fruit, vegetables, wholegrains and pulses, as well as low-fat dairy products and oily fish. They should be advised to maintain a healthy weight to maintain a BMI of between 20 and 25kg/m2.10,11 Patients should be taught how to measure and understand their blood glucose levels. Quality control of the glucose monitor should be checked four times a year and monitors should be changed or upgraded every two years. Patients should be advised to record home glucose readings in their patient record book and to bring the book to each of their diabetic reviews.10
The UK’s NICE guidelines recommends that all patients with T2DM should be referred to a diabetes structured education programme at or around the time of diagnosis. Structured diabetes education is a group programme that provides patients with the knowledge, skill and ability to manage their diabetes.
All patients with diabetes should receive the following checks at least once per year to reduce the risk of long-term complications: HbA1c level; blood pressure; cholesterol; retinal screening (depending on risk); foot examination; kidney function; urinary albumin; BMI; and smoking status. Reducing glucose levels lowers the risk of all long-term complications of diabetes, while reducing cholesterol levels lowers the risk of heart attacks and strokes.12
Blood glucose targets
Tight control of blood glucose with diet and/or medication reduces long-term diabetes-related complications and is central to the overall management of diabetes. Blood glucose targets should be individualised and discussed with the patient. A HbA1c ≤53mmol/l is appropriate for most people with T2DM and has been shown to reduce diabetes-related complications.18
A HbA1c ≤ 58mmol/l or less stringent A1c goals may be appropriate for:
People with a history of:
Severe hypoglycaemia;
Limited life expectancy;
Advanced microvascular or macrovascular complications;
Extensive co-morbid conditions; or
Where social circumstance may prevent tight glucose control.
A HbA1c ≤48mmol/l may be appropriate for newly-diagnosed people with T2DM and no significant co-morbidities.
Targets should be set in consultation with the individual and should be seen as a guide because a person’s individual circumstances need to be considered when setting and agreeing targets, according to the HSE’s Model of Care.18
The HbA1c should be checked more than twice a year in patients to maintain treatment targets.
Medications
Healthy eating and exercise are the cornerstones of T2DM management, but frequently people need the addition of medications to help improve blood glucose control. When lifestyle modification fails to achieve the targeted blood glucose levels, the first-line medication prescribed is metformin,18 both for those who are overweight (BMI >25.0kg/m2) and not overweight. Metformin is contraindicated in those with renal impairment and with end-stage cardiac and hepatic failure. Metformin should be stopped in patients with eGFR <30mls/ min and at possibly higher values in patients prone to dehydration.10
The HSE’s Model of Care contains an algorithm with a step-wise treatment approach, with second-line and other agents including DPP-4 inhibitors, sulphonylureas, GLP-1 receptor agonists, pioglitazone, acarbose, meglitinides, sodium glucose co-transporter 2 (SGLT2) inhibitors, and insulin.18
Since 2015, NICE has been advocating a patient-centred approach to glycaemic control and provides best practice advice on setting glycaemic targets and selecting hypoglycaemic agents for treatment intensification after metformin first-line treatment for T2DM in those with inadequate diabetes control.12
Most guidelines recommend the use of insulin alone or in combination with other GLDs when persons with T2DM are unstable, with sign and symptoms of acute decompensation including dehydration, acute weight loss, acute illness, very high glucose levels, and presence of ketones. Basal insulin should be preferred and it can be temporary. Most insulin algorithms start with 10 units or 0.2 units/kg and titrate once or twice weekly at one-to-two units each time to achieve a target fasting blood glucose between 3.9-and-7.2mmol/L (70-and-130mg/dL).8
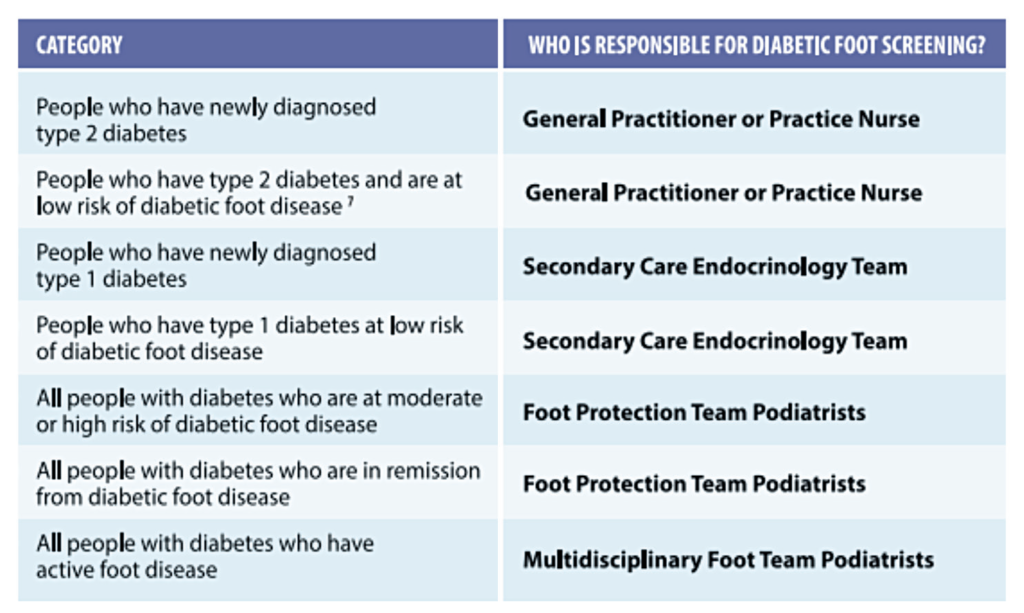
Diabetic Foot Model of Care 2021: T2DM
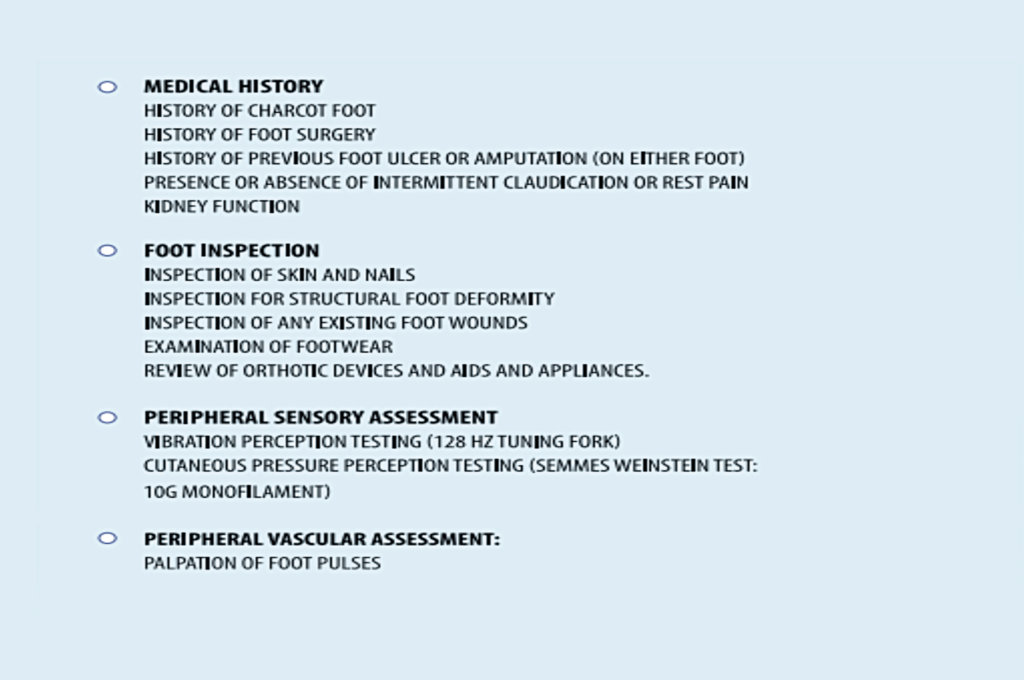
In 2021 the HSE published its Diabetic Foot Model of Care13 document. The aim of diabetic foot screening and risk classification is to establish the person’s risk of diabetic foot ulceration. All persons with diabetes are assigned a risk category and where appropriate referred for ongoing foot screening, a foot assessment, and a clinical care plan. The care plan ensures that all people with diabetes receive annual or more frequent foot screening, foot care education and review according to their clinical needs and in the most appropriate setting.13
Exception: Those with very complicated T2DM should have annual foot screening and care provided by the endocrinologist and their team.
Based on the findings of this screening the person is categorised as being low-, moderate- or high-risk of future diabetic foot ulceration, or if known to have prior foot ulceration will be categorised as being in remission or categorised as active foot disease, if foot ulceration is present or active Charcot is suspected.13
Long-term complications of T2DM include diabetic retinopathy, diabetic nephropathy, diabetic neuropathy, and macrovascular problems.
Diabetic retinopathy is one of the most common causes of blindness in the working age population in Ireland. Up to 10 per cent of people with diabetes are at risk of sight-threatening retinopathy. Diabetic retinopathy may have no obvious symptoms in its early stages, but when caught early, treatment is effective at reducing or preventing damage to sight.10 The national diabetic retinopathy screening programme, Diabetic RetinaScreen, has been providing free retinal screening to all diabetes patients in Ireland over the age of 12 years since 2013.18 Since the programme’s launch, prevalent, undiagnosed, and untreated diabetic retinopathy and maculopathy have been successfully identified and referred for evidence-based treatments at the programme’s seven treatment centres before any significant visual symptoms occur. Adding patients to the register to be screened is easy, and can be done by a patient’s GP, or allied health professionals using the free phone number: 1800 454 555 or email info@diabeticretinascreen.ie. Full screening information is available at www. diabeticretinascreen.ie.
Diabetic nephropathy is a significant cause of chronic kidney disease and end-stage renal failure globally. If untreated, diabetic nephropathy can lead to impaired kidney function, dialysis, and/ or kidney transplant. Diabetic nephropathy is identified when eGFR is <60mL/ min/1.73m² and albuminuria >30mg/g creatinine.8,14 Annual assessment (at least) with urine ACR, serum creatinine and eGFR) is recommended.18
Diabetic neuropathy is the most common complication associated with diabetes mellitus. Diabetes causes a broad spectrum of neuropathic complications, including peripheral, autonomic, proximal, and focal. Diabetic peripheral neuropathy (DPN) is the most common form of nerve damage, and it most often affects the nerves to the hands and feet. DPN leads to distressing and expensive clinical sequelae, such as foot ulceration, leg amputation, and neuropathic pain. DPN is often diagnosed late when irreversible nerve injury has occurred, and its first presentation may be with a diabetic foot ulcer.1 DPN may be present at time of diagnosis in more than 10 per cent of patients and may affect up to 50 per cent of patients with long-standing diabetes. In 50 per cent of cases, DPN may be asymptomatic, but for 16-to-26 per cent of patients with diabetes the neuropathy is painful. Patients should be examined for DPN from time of diagnosis.18
Macrovascular: T2DM can also affect the large blood vessels, causing plaque to build up, leading to a heart attack, stroke and peripheral vascular disease. Cardiovascular disease (CVD) is the leading cause (∼70 per cent) of death in people with T2DM. People with diabetes have a four-fold greater risk for having a CVD event than people without diabetes after controlling for traditional risk factors for CVD, such as age, obesity, tobacco use, dyslipidaemia, and hypertension.16
Prevention and patient education
Patient education and effective lifestyle modifications including weight loss and adoption of a healthy diet together with increased physical activity are the cornerstones for the prevention of type 2 diabetes mellitus. Emphasis must be placed on promoting a healthier lifestyle and finding solutions for increased adherence and compliance, especially for high-risk individuals.
Diabetes SMART is a new free interactive online education course developed by Diabetes Ireland, for people diagnosed with T2DM. The Diabetes SMART programme contains six interactive modules, covering topics that explain what diabetes is, understanding the key medical information, such as blood glucose levels, managing illness, and providing tips on healthy eating, and getting active. The programme was developed by diabetes healthcare professionals and the resource will give people with T2DM the knowledge and accessible tools to learn how to manage their condition and protect their future health.1
The HSE also provides a number of free educational resources and support courses to diabetes patients, both online and in person. See here for more information.
Outlook
While there is still no cure for T2DM, several drugs are in the developmental stages. Perhaps, the most anticipated is the glucagon-like peptide-1 (GLP-1) receptor agonists, which induce insulin production while also suppressing the secretion of glucagon.7
Imeglimin, a drug being developed by the French company Poxel, has shown great promise in a phase 3 clinical trial in Japan. Damage to the mitochondria, the structures that generate energy within cells, plays a key role in the progression of metabolic diseases, and Imeglimin protects mitochondria from damage. With this unique method of action, imeglimin has the potential to treat T2DM by acting in three organs at once: The pancreas, the liver, and the muscles to reduce blood glucose levels.16
Adjustments to dietary nutrient composition, insulin-secreting cell implants, bariatric surgery, and agents primarily designed to suppress appetite and reduce adiposity, will also greatly contribute to the future management of T2DM.
2. Leahy S, O’Halloran AM, O’Leary N, Healy M, McCormack M, Kenny RA, O’Connell J. Prevalence and correlates of diagnosed and undiagnosed type 2 diabetes mellitus and pre-diabetes in older adults: Findings from the Irish Longitudinal Study on Ageing (TILDA). Diabetes Res Clin Pract. 2015 Dec;110(3):241-9. doi: 10.1016/j.diabres.2015.10.015
3. International Diabetes Federation Diabetes Atlas (2021), Available at: https://diabetesatlas.org/
5. Bellou V, Belbasis L, Tzoulaki I, Evangelo E. (2018). Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses. PLoS One. 2018 Mar 20; 13(3):eo194127. doi: 10.1371/journal.pone.0194127
7. Lam M. (2019). Diagnosis and management of type 2 diabetes mellitus. The Pharmaceutical Journal. Vol 303; No 7929; 303. doi: 10.1211/PJ.2019.20206770
9. World Health Organisation. (2011). Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus: Abbreviated report of a WHO consultation. Available at: www.who.int/diabetes/publications/report-hba1c_2011.pdf?ua=1
10. ICGP (2016). A practical guide to integrated type 2 diabetes care. Irish College of General Practitioners, Ireland.
11. Goyal R, Jialal I, Castano M. (2022). Diabetes Mellitus Type 2 (Nursing) In StatPearls Publishing; 2022 Jan. Available from: www.ncbi.nlm.nih.gov/books/NBK568737/
12. National Institute for Health and Care Excellence. Type 2 diabetes in adults: Management. NICE guideline [NG28]. 2019. Available at: www.nice.org.uk/guidance/NG28
14. Lim A. (2014). Diabetic nephropathy – complications and treatment. Int J Nephrol Renovasc Dis. 2014 Oct 15;7:361-81. doi: 10.2147/IJNRD.S40172
15. Yang H, Sloan G, Ye Y, et al (2020). New perspective in diabetic neuropathy: From the periphery to the brain, a call for early detection and precision medicine. Front Endocrinol, 17 January 2020. doi: 10.3389/fendo.2019.00929
16. Cade WT. (2018). Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Physical therapy, 88(11), 1322–1335. doi: 10.2522/ptj.20180008












Leave a Reply
You must be logged in to post a comment.