NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Dean Moore & Dr Eoin Brennan
- 04th Oct 2022
Diabetes is the most common cause of chronic kidney disease (CKD), with a range of established and incoming treatment options to slow progression and reduce morbidity and mortality.
Just over 101 years ago, in July 1921, Banting and Best first isolated insulin, revolutionising the treatment of diabetes, changing the natural history of the disease from a short, swift and brutal fatal illness to the chronic and manageable disease we have today. In the intervening century the strides in scientific discovery have been remarkable, with the development of continuous glucose monitoring, insulin pumps, and pancreatic transplants.
Concurrently, we have witnessed advances in understanding the aetiology of diabetes at the molecular level and we now see the promise of an artificial pancreas and targeted gene therapy on the horizon. As the medical world has reacclimatised to life in the post-pandemic world, renewed focus on novel treatments for the more ‘mundane’ diseases has resulted in new hope for clinicians and patients alike. Diabetes is a perfect exemplar in this regard.
More than half a billion people worldwide live with diabetes, with prevalent cases having tripled since 2000. The acceleration of incidence is not a phenomenon isolated to high-income countries; it is quickly becoming a disease of low- and middle-income countries. In resource-restricted settings the substantial attendant cardiovascular and microvascular morbidity is likely to exact a high price physically, financially, and psychosocially. While in Ireland no national diabetes registry exists, accepted estimates for prevalent cases in the Republic are more than 250,000, with close to 90 per cent of these cases being type 2 diabetes (T2DM). Interestingly, The Irish Longitudinal Study on Ageing (TILDA) 2015 showed that 10 per cent of adults aged 50 years and over in Ireland have T2DM, with one-in-10 people with diabetes being undiagnosed in this population. Given the magnitude of this visible and invisible disease burden both nationally and internationally, an understanding of recent developments in the treatment of diabetes and associated complications is relevant to most clinicians.
The morbidity and mortality associated with T2DM is attributable to microvascular (nephropathy, retinopathy and neuropathy) and macrovascular disease (cardiovascular disease). The onset of T2DM is often surreptitious and therefore these complications are frequently present at time of diagnosis of diabetes. In many cases the onset of these complications can be delayed through risk factor modification; namely addressing dyslipidaemia, hypertension, and satisfactory glycaemic control. Once these complications have become established their progression can be delayed through similar means.
With regard the rates of microvascular complications in Ireland, the most thorough estimate is from a systematic review and metanalysis in 2016, where prevalence of microvascular complications was varied, ranging from 6.5-to-25.2 per cent for retinopathy; 3.2-to-32.0 per cent for neuropathy; and 2.5-to-5.2 per cent for nephropathy. While these figures are similar to rates found internationally (apart from nephropathy, which is underrepresented), care must be exercised given the wide margin of variation, which is likely in part attributable to the varied study settings and heterogeneity in the diagnostic criteria for microvascular and macrovascular complications.
Current treatment options for DKD
Diabetic nephropathy will complicate diabetes in 40 per cent of cases. Separately, diabetes is the most common cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD), both worldwide and in Ireland. As already mentioned, prevention of diabetic complications can be achieved with good glycaemic control in both type 1 diabetes mellitus (T1DM) and T2DM. However, intensive glycaemic control in established microvascular disease has not been shown to improve cardiovascular outcomes or slow progression.
When considering treatment options for established DKD, several agents are effective in slowing progression and reducing morbidity and mortality
When considering treatment options for established DKD, several agents are effective in slowing progression and reducing morbidity and mortality. In patients with albuminuria or proteinuria, the strong evidential basis for renin-angiotensin-aldosterone system (RAAS) inhibitor use has remained as a cornerstone in the treatment of DKD, regardless of the presence of hypertension. The dual use of both an angiotensin receptor blocker (ARB) and an angiotensin converting enzyme (ACE) inhibitor confer no clinical benefit across several trials, while increasing the risk of hyperkalaemia and acute kidney injury.
Since the initial trials of sodium-glucose cotransporter-2 (SGLT2) inhibitors reported improvements in declining renal function and proteinuria in 2016, there has been a large volume of randomised control trials and real-world data to support the use of SGLT2 inhibitors as an effective therapy in slowing DKD progression and reducing major adverse cardiac events. While the improvement with glycaemic control is modest, the improvement in renal and cardiac outcomes have demonstrated a strong class effect and have been incorporated as standard care in most proteinuric CKD and heart failure. Interestingly, recent data suggests that the effect of SGLT2 inhibitors seems to be more pronounced in patients with more advanced CKD. Safety data regarding initial greater rates of amputation in early trials have not been replicated since or in real world data, but the increase in UTIs and fungal genital infections have been widely observed. While the incidence of euglycaemic diabetic ketoacidosis is increased with the use of SGLT2 inhibitors, the absolute risk remains relatively low.
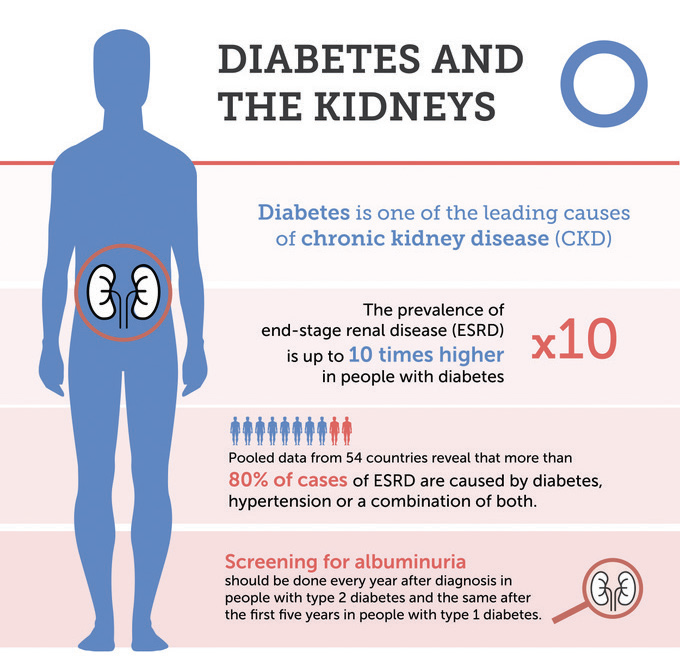
IMAGE 1: Diabetes and kidney disease
Apart from SGLT2 inhibitors, the glucose-lowering agents with the greatest evidence of renal and cardiovascular protection are the glucagon-like peptide 1 (GLP1) receptor agonists. Great interest has arisen in the use of GLP1 mimetics due to the observation that significant weight loss has been associated with their use, particularly given the rapidly rising rates of obesity and its strong association with T2DM. With the emergence of more long-term real-world data, the use of GLP1 agonists will likely increase.
Excessive activation of the renal endothelin system (particularly renal endothelin-1) has been shown to be an effective mediator of kidney injury in diabetes. The use of the endothelin receptor antagonist atrasentan had shown initial promise as a potential therapy in DKD. Pre-clinical studies demonstrated the efficacy of endothelin-A receptor antagonism in downregulating the inflammatory and fibrotic effect of endothelin-1.
Phase 2 trials showed atrasentan decreased albuminuria in DKD already on maximum RAAS inhibition, however, a large phase 3 trial showed that despite very selective inclusion criteria the adverse effect of oedema and worsening of heart failure was significant. While it may have a role in a highly selected patient population, its side-effect profile will preclude its adoption as a standard therapy.
With the role of RAAS inhibition in DKD being well elucidated, the downstream inhibition of aldosterone has been examined in the treatment of DKD in patients on a maximally tolerated ACE inhibitor or ARB. The mineralocorticoid receptor (MR), which binds aldosterone, has been studied in detail and its overactivation in both cardiac and renal disease is well established and implicated in inflammation, fibrosis, and cardiovascular disease.
The MR is a nuclear receptor expressed in a variety of tissues throughout the body, most pertinently in this case the kidney and heart. The MR is a promiscuous receptor and can be activated by other steroid hormones, namely cortisol and progesterone. The steroidal MR antagonists (MRAs) spironolactone and eplerenone have been shown to improve morbidity and mortality in heart failure with reduced ejection fraction (HFrEF), but not heart failure with preserved ejection fraction (HFpEF). The main limitation in the use of spironolactone is gynaecomastia and hyperkalaemia. Eplerenone was developed as a more selective MRA with trial data showing an incidence of gynaecomastia no different than placebo.
The novel agent finerenone has been developed as a non-steroidal MRA in an effort to mitigate the off-target effects of MR inhibition, with two large RCTs demonstrating its efficacy in DKD and cardiovascular disease (CVD) with no increase in sex hormone mediated side-effects. Higher rates of hyperkalaemia compared to placebo were again noted, particularly in patients with lower eGFRs, but perhaps lower when compared to spironolactone.
Targeting inflammation in DKD
While the established therapies discussed above focus primarily on neurohormonal modulation in an effort to slow and ameliorate end organ damage in diabetes, the role of inflammation in the pathogenesis of diabetes and DKD has become increasingly apparent. Inflammation is a vital element in the armamentarium of the host defence, with several highly conserved pathways conducting its initiation, progression, and resolution to ensure an effective and effectively controlled process to remove pathogens and enable tissue repair.
This is a regulated and finite process in the healthy host under physiological conditions. A dysregulated inflammatory response is notable and notorious as the underlying mechanism for sepsis in an acute setting, but chronic and low-grade inflammation results in fibrosis, functional decline and ultimately can lead to organ failure.
With regard to T1DM, the role of inflammation and autoimmunity in its aetiology has been well established. Inflammation in pancreatic islet beta-cells results in cell depletion and loss of function.
Findings from experimental models and observational studies in humans demonstrate a key role for macrophages in islet beta-cell inflammation in obesity and T2DM, driven largely by responses to a family of cytokines including IFN-, TNF- and IL-1. Islet autoimmunity might also contribute to the functional decline of beta-cells during the course of T2DM.
The role of obesity as a driver of inflammation has been delineated and the mechanisms by which it contributes to insulin resistance has been identified in several studies. The metabolic function of adipose tissues is the storage of fat, with the expansion of adipose deposits, especially abdominal deposition, being associated with T2DM, CVD and insulin resistance.
Adipose tissue is an active endocrine organ, which expresses a variety of cytokines and chemokines to regulate energy utilisation, with derangements in its function having demonstrable effects. In situations where the ability to store calories as white fat is exceeded, ectopic deposition in non-adipose tissues (skeletal muscle, liver, kidney, pancreas) occurs where it exerts what has been termed a lipotoxic effect on the non-adipose tissue in question, by invoking an inflammatory response, an example of sterile inflammation.
The role of inflammation in the development of microvascular and macrovascular damage in diabetes has led to the investigation of anti-inflammatory-based therapies. Such approaches are well known in the contemporary practice of medicine, from the use of NSAIDs in acute inflammatory pain, to the corticosteroid dexamethasone and the IL-6 receptor antibody tocolizumab in the cytokine storm of severe Covid-19.
However, despite the use of anti-inflammatory strategies in certain circumstances, concerns exist regarding impairing the host response in other circumstances leading to inadequate response to exogenous pathogens.
Several examples of this are evident in the literature, for example, the TESTING trial, which examined the use of methylprednisolone in IgA nephropathy. A statistically-significant reduction in kidney function decline was noted with the use of the steroid, but excess infections and mortality in the treatment group mandated termination of the trial prematurely and redesign at a lower dose of steroid in an effort to reduce this adverse effect (which was ultimately unsuccessful).
Baricitinib, an inhibitor of the JAK-STAT inflammatory pathway, has been investigated in patients with DKD, with phase 2 trial data demonstrating a significant reduction in albuminuria, a key indicator of DKD progression. In patients with T2DM and kidney disease, a randomised phase 2 trial demonstrated therapeutic potential of the anti-inflammatory CCR2 antagonist CCX140-B, with significant reductions in albuminuria when given in addition to standard care.
While there is caution with respect to targeting DKD with anti-inflammatories, inflammation remains a plausible target to pursue, and it is worth noting that many of the established medicines currently used in practice, such as RAAS and SGLT2 inhibitors, have been demonstrated to exert anti-inflammatory effects.
Looking ahead: How can we improve the diagnosis and treatment of DKD?
The precision medicine era promises individual level healthcare decisions whereby your genetic, proteomic and metabolomic biomarker make-up will guide diagnosis and tailored pharmacotherapy. Central to this model of precision medicine is the need for accurate biomarkers, and for a long time this has been a challenge for DKD.
However, technological advances in recent years are beginning to address this problem, now allowing for the simultaneous measurement of numerous proteins and metabolites in DKD patient blood and urine, offering hope for less invasive means of diagnosis and prognosis. As a result, biomarker panels of proteins are being explored as a potential tool to better predict early kidney function decline as compared with or in tandem with more traditional markers – albuminuria and eGFR.
The role of inflammation in the development of microvascular and macrovascular damage in diabetes has led to the investigation of anti-inflammatory-based therapies
While studies of DNA in patients of many single-gene diseases have proven truly transformative, when searching for changes in the DNA code that might be associated with risk of a complex and multifactorial disease such as DKD, this has proven to be much more challenging.
Nevertheless, several large-scale international studies have examined the DNA of patients with DKD, including Irish participants, pointing us to several regions of the human genome that if perturbed may alter one’s risk of developing DKD. One such study led by the GENIE consortium identified a protective DNA variant in the collagen 4-alpha 3 gene, and the presence of this variant was associated with a thinner glomerular basement membrane.
Could carriers of this DNA variant be protected from developing advanced DKD? Armed with this type of genetic information, should we consider such disease-associated DNA variants as simple risk predictors for early diagnosis, or do we attempt to correct the DNA sequence using the latest genome-editing technologies (CRISPR/Cas- 9)? Given the complexity of DKD and the likely contribution of many DNA variants to disease risk, it is unlikely we will see the latter for some time, but this is no longer science fiction and such approaches could be closer than you might expect.
This year, US-based Verve Therapeutics began a human trial using CRISPR DNA-editing technology to modify the PCSK9 gene in people with heterozygous familial hypercholesterolaemia, a condition that can lead to early-onset atherosclerosis and increased risk of CVD. PCSK9 is a protein involved in lowering LDL cholesterol, and several effective, but expensive PCSK9 inhibitors are now available for patients. In parallel with these drug development success stories, genetics studies discovered adults with naturally occurring mutations in their PCSK9 gene that seemed to switch off this gene, resulting in low cholesterol levels and overall excellent cardiovascular health.
These lucky few had won the genetic lottery by coming up with the wining code. Taking advantage of this, Verve Therapeutics wants to introduce mutations into patient DNA and ultimately switch off the PCSK9 gene to lower LDL cholesterol levels. According to Verve Therapeutics, this would represent a ‘single-course, life-long treatment solution’. While we are not quite there yet with DKD, the scenario may arise in the not-too distant future where you can decide on conventional pharmacotherapy or one-shot gene therapy.
Finally, stem cell therapy promises to revolutionise regenerative medicine for the treatment of many diseases, and diabetes management strategies will surely in time benefit from such developments. For T1DM, the holy grail centres on pancreatic beta cell replacement therapies, allowing for the implantation of insulin-producing beta cells. In this space, in June 2022 the US-based company Vertex Therapeutics announced exciting clinical trial data from the first T1DM patients receiving their beta cell therapy VX-880, demonstrating a remarkable lowering of blood glucose, without the need for regular insulin injections.
While we eagerly await more data from this trial and consider the lingering concerns over the necessity for immunosuppressant medications in tandem with stem cell therapies, this has the potential to be a game-changer that could instantly improve the quality-of-life of so many patients with T1DM. This would inevitably have a positive impact on the global prevalence of vascular complications of diabetes, such as DKD.
Conclusion
DKD is a major global health challenge with high prevalence and an absence of predictive biomarkers that allow us to identify those in the population at greatest risk of developing this disease. Current therapies at best halt, but do not reverse kidney damage. Recent advancements in technologies may allow us to identify new diagnostic and prognostic biomarkers, as well as novel gene and cell-based next generation therapies. Such developments may be the only solution to this complex problem.
DR DEAN MOORE, SpR, Department of Renal Medicine, Mater Misericordiae University Hospital; and DR EOIN BRENNAN, Assistant Professor, Diabetes Complications Research Centre, School of Medicine, University College Dublin.











Leave a Reply
You must be logged in to post a comment.