NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
THERESA LOWRY-LEHNEN, RGN, GPN, RNP, BSc, MSc, M Ed, PhD, Clinical Nurse Specialist and Associate Lecturer, Institute of Technology, Carlow
Hyperlipidaemia is among the leading risk factors associated with cardiovascular disease (CVD)
Hyperlipidaemia is characterised by an increase in one or more of the plasma lipids, including cholesterol, cholesterol esters, triglycerides, phospholipids and/or plasma lipoproteins including very low-density and low-density lipoprotein along with reduced high-density lipoprotein levels.1
Hyperlipidaemia, in particular elevated LDL cholesterol (low-density lipoprotein), is one of the most prevalent risk factors contributing to atherosclerosis and consequent vascular disease. In contrast, high-density lipoprotein (HDL) cholesterol assists in regulating cholesterol levels to prevent imbalances. Atherosclerosis is a pathologic process characterised by the accumulation of lipids, cholesterol and calcium and the development of fibrous plaques within the walls of large and medium arteries.
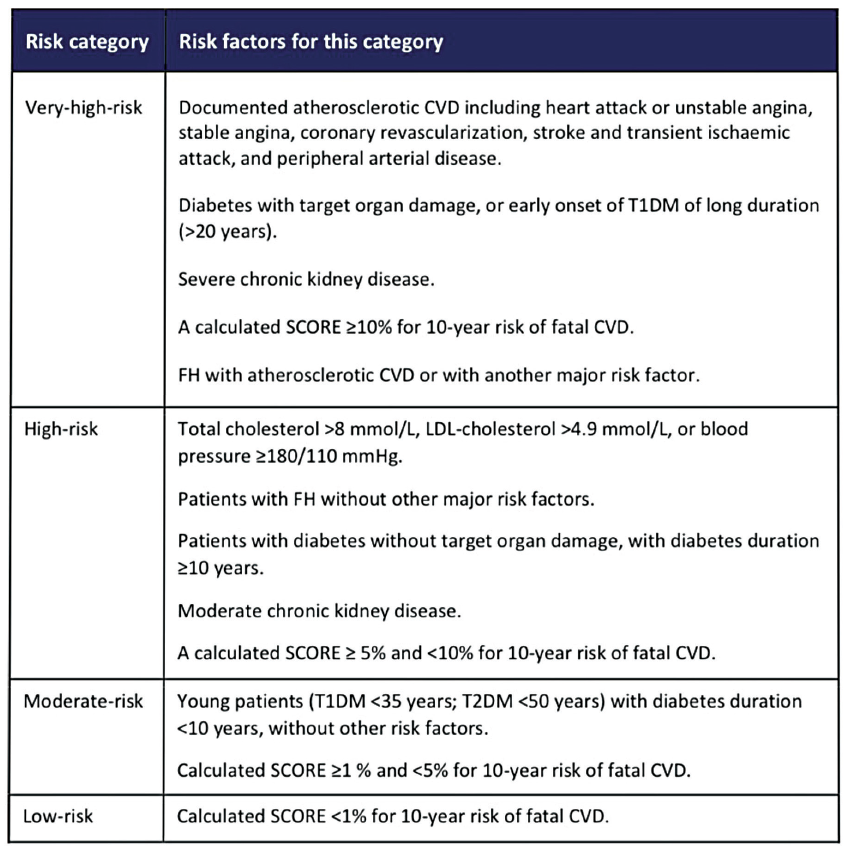
FIGURE 1: Risk categories for dyslipidaemia and patient groups in each of these categories (ESC/EAS, 2019)5
Hypercholesterolaemia and hypertriglyceridaemia are the main cause of atherosclerosis, which is strongly related to ischaemic heart disease (IHD).1,2 Atherosclerosis often remains asymptomatic until plaque stenosis reaches 70-to-80 per cent of the vessel’s diameter. It originates after underlying endothelial damage occurs, which stems from loss of nitric oxide within the endothelium. This process leads to increased inflammation directly around the dysfunctional site, permitting the accumulation of lipids within the innermost layer of the endothelial wall. The lipids are then engulfed by macrophages, leading to the establishment of ‘foam cells’ or debris. Cholesterol build-up within the foam cells causes subsequent mitochondrial dysfunction, apoptosis, and necrosis of the underlying tissues. Smooth muscle cells encapsulate the pack of foam cells, which produces a fibrotic plaque that inhibits underlying lipids from being destroyed.2
Cholesterol is naturally produced within the body and can also be obtained from animal fats in food. Cholesterol is absent in plant-based foods, however, plant products such as flax seeds may contain cholesterol-like compounds called phytosterols which are beneficial in the body. Cholesterol is an essential substance in the body necessary for the production of cell structures and plasma membranes, energy expenditure and bile formation and it is important for the synthesis of steroids, hormones, vitamin D and other substances.3 Adults typically synthesise about 1g of cholesterol per day and the total body content is approximately 35g. The liver is the primary organ that synthesises cholesterol. About 20-to-25 per cent of total daily cholesterol production occurs in the liver. It is also synthesised to a smaller extent in the adrenal glands, intestines and reproductive organs. The predominant route of cholesterol elimination from the body is by excretion into the bile. Cholesterol from cells is transported from the plasma membranes of peripheral cells to the liver HDL-mediated process termed reverse cholesterol transport.3
Major dietary sources of cholesterol include cheese, egg yolks, beef, pork, poultry, and shrimp. Saturated and trans saturated fats in food raise blood cholesterol. Saturated fats are present in full fat dairy products, animal fats, and several types of oil and chocolate. Trans saturated fats are present in hydrogenated oils, which are found in many fast and snack foods and fried or baked products.3
The diagnosis of hyperlipidaemia is often an incidental finding following a routine screening by a patient’s GP or general practice nurse conducting a cardiovascular risk assessment
Hyperlipidaemia can be subdivided into two broad categories: primary (familial) or secondary (acquired). Familial hypercholesterolaemia (FH) is an inherited genetic defect that may lead to early development of atherosclerosis and IHD. Homozygous FH is rare; affecting 1:160,000 people, while heterozygous FH is more common; affecting approximately 1:250 people.4 Familial combined hyperlipidaemia may occur as an interaction of multiple genes and the person’s environment, and occurs in 1:100 to 1:200 people. Secondary hyperlipidaemia accounts for up to 40 per cent of hyperlipidaemia cases and typically originates from an alternate aetiology, such as an unhealthy diet, medications including amiodarone, and glucocorticoids, hypothyroidism, uncontrolled diabetes, and/or a poor lifestyle.2.4
For most patients, hyperlipidaemia is polygenic and influenced by factors such as obesity, saturated fat intake and the cholesterol content within the person’s diet. Another mechanism involves elevated levels of ‘apo B-100’ lipoproteins within the plasma, which may lead to atherosclerotic disease, even when the patient has no other risk factors. There is often a combination of genetic and environmental factors involved that contribute to a person’s risk of developing hyperlipidaemia and cardiovascular disease.2
Diagnosis
The diagnosis of hyperlipidaemia is often an incidental finding following a routine screening by a patient’s GP or general practice nurse conducting a cardiovascular risk assessment. Regularly, patients presenting with underlying hyperlipidaemia remain asymptomatic, therefore obtaining a thorough history is essential. It is important to assess a patient’s family history of cardiovascular disease, hyperlipidaemia, and/or familial hypercholesterolaemia, the patient’s diet and exercise habits, tobacco, alcohol or drug use, the presence of coronary artery disease (CAD), risk factors or history of CAD; and/or symptoms of peripheral arterial disease or angina.2
A focused physical exam is very important, including accurate blood pressure measurements, observing the patient’s skin for xanthomas, listening for carotid and femoral bruits for evidence of stenosis, listening for an S4 heart sound, and palpating for intact peripheral pulses in all four extremities. Bloods including a lipid profile (fasting) will be carried out which routinely includes LDL, HDL, triglycerides and total cholesterol. Other blood tests may include LFTs, HbA1c and TFTs. Urinalysis can be collected to screen for albuminuria.2
Treatment and management
The treatment of hyperlipidaemia involves both primary and secondary prevention. Primary prevention concerns people with high cholesterol at risk of CVD with comorbidities, such as high blood pressure, type 1 and 2 diabetes, or kidney disease, who do not yet have established CVD. Secondary prevention involves treating individuals with established CVD.4
The European Society of Cardiology and European Atherosclerosis Society (ESC/EAS) 2019 guidelines for the management of dyslipidaemia outline the risk categories and patient groups in each of these categories (Figure 1), and intervention strategies for primary and secondary prevention as a function of total cardiovascular risk and untreated low-density lipoprotein cholesterol levels.5
Initial treatment modalities are focused on diet and lifestyle modification, with the addition of lipid-lowering medications if needed. Patients with mild hyperlipidaemia and low CVD risk should focus on a low fat, low carbohydrate diet, and moderate to high-intensity physical activity. Heart health diets are low in saturated and trans fats, sodium, added sugars and refined grains. Weight loss and regular exercise do not result in significant LDL reduction; however, they play an important part in good cardiovascular health and are associated with reduced triglyceride levels. Smoking cessation, lowering blood pressure, and losing weight are beneficial to lowering vascular disease risk. For patients at moderate-to-high CVD risk, the above lifestyle modification applies and lipid-lowering statin medications should be added. There is a clear and proven benefit to statin therapy for the vast majority of patients from low-risk to high-risk, therefore these drugs’ side-effects and costs should be weighed against the individual patient’s potential benefit from taking the medication.2,6
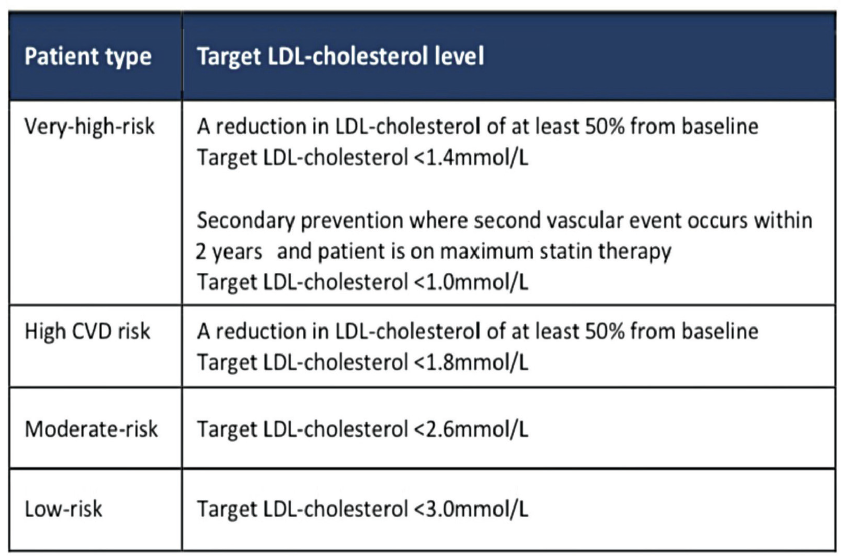
The ESC/EAS 2019 guidelines for the management of dyslipidaemia also outline target plasma LDL cholesterol levels according to the patient’s risk level (Figure 2).4,5
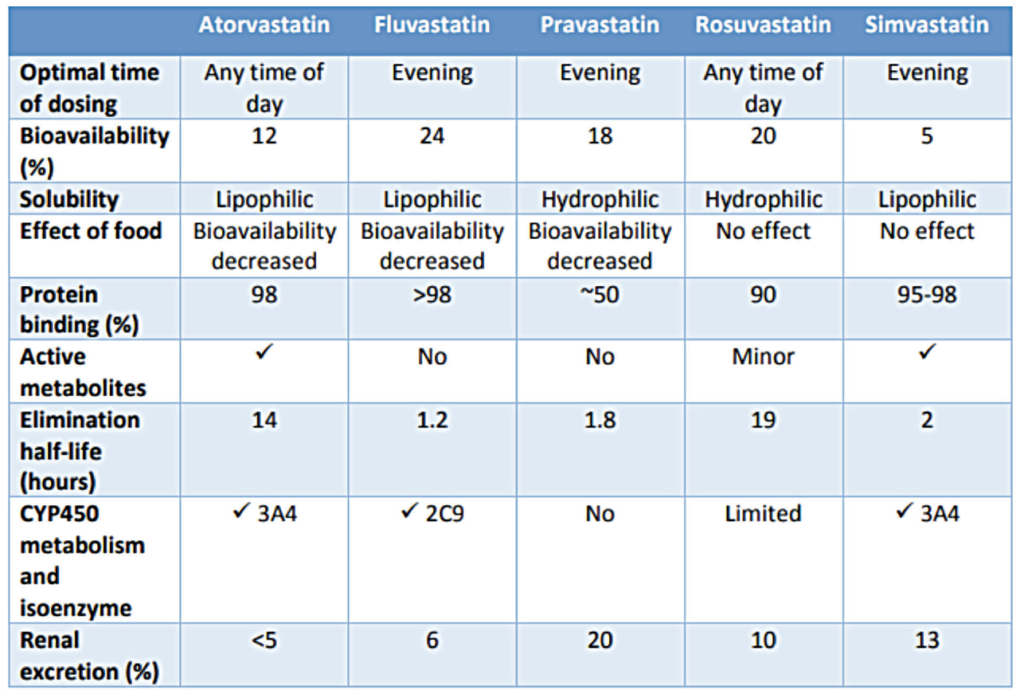
Statins are associated with a 30-to-60 per cent reduction in LDL cholesterol; a reduction of 20-to-40 per cent in triglyceride levels; and an increase in HDL cholesterol levels of approximately 3-to-12 per cent.4 Statins are the first-line pharmacological intervention for abnormal lipid profiles. They work by inhibition of the enzyme HMG-CoA reductase, which is involved in the production of mevalonic acid in the cholesterol biosynthesis pathway. By preventing the endogenous production of cholesterol, the expression of LDL receptors in liver cells is up-regulated, enhancing the clearance of the circulating LDL-C particles from the blood.6 Five statins are marketed for use in Ireland – atorvastatin, fluvastatin, pravastatin, rosuvastatin, and simvastatin. Atorvastatin is the preferred statin for the treatment of hypercholesterolaemia and prevention of cardiovascular events under the HSE’s Medicine Management Programme (MMP) guidance.6
The usual starting dose of atorvastatin is 10mg once daily, and the dose can be adjusted at intervals of four weeks or more to achieve the target LDL cholesterol level. In secondary prevention, 30mgs daily should be initiated after diagnosis.4
FIGURE 3: Pharmacokinetic properties of statins6 (HSE Medicines Management Programme)
Prior to commencing cholesterol-lowering therapy, baseline cholesterol, LDL and HDL, and triglycerides must be measured. TFTs should also be checked and hypothyroidism treated if present before commencing cholesterol-reducing medication. LFTs should be measured and statins should not be commenced if liver transaminases are ≥3 times the upper normal limit.4
Ezetimibe, co-administered with an HMG-CoA reductase inhibitor (statin) is indicated as an adjunctive therapy to diet for use in patients with primary (heterozygous familial and non-familial) hypercholesterolaemia who are not appropriately controlled with a statin alone.8 PCSK9 inhibitors, evolocumab and alirocumab, are monoclonal antibodies administered subcutaneously, which have shown an LDL cholesterol-reducing effect of up to 60 per cent when used alone and up to 70 per cent when used in conjunction with a statin. They can lower triglycerides by over 25 per cent. PCSK9 inhibitors are associated with reductions in the risk of heart attack and stroke. Evolocumab and alirocumab are both indicated for use in adults over the age of 18 years, and evolocumab is indicated for use in patients over the age of 12.4
Complications
Patient education and information regarding lifestyle modification and pharmacological therapy is the key to success for improved cholesterol control and to prevent complications. Weight management, proper diet, increased physical activity, and smoking cessation are important factors to address, to decrease cardiovascular risk. If pharmacological therapy is required, discussion of the risks and benefits of each medication should be explained to the patient before initiation. Primary care clinicians and pharmacists have a duty to educate the patient on medication compliance, side-effects, interactions, and overall risks versus the benefits of the medications prescribed. The patient must also understand the potential risks related to not taking the medication and what alternatives they may have as treatment options.
Potential statin medication complications include myopathy, renal injury, arthralgia, extremity pains, nausea, myalgia, elevated liver enzymes/hepatotoxicity, diarrhoea, and rhabdomyolysis. Up to 5-to-20 per cent of patients taking a statin medication report experiencing a muscle-related intolerance. A lower dose of the statin should be tried or a transition to another lipid-lowering medication such as ezetimibe or a PCSK9 inhibitor such as evolocumab or alirocumab attempted.2
FIGURE 2: ESC/EAS (2019). Guidelines for the management of dyslipidaemia5
Benefits and monitoring
Based on a 20-year follow up of the West of Scotland Coronary Prevention Study, patients who received statin therapy for five years demonstrated improved survival rates and a clinically significant reduction in CVD over the 20 year period. This data and numerous other studies and clinical trials have shown a significant cardiovascular risk reduction when statin therapy is used appropriately.7
Patients should be monitored regularly in practice to prevent hyperlipidaemia progression and improve patient outcomes. Patients receiving lipid-lowering medications should be reviewed after three months of initiating treatment and then at least once yearly. In those receiving statin therapy, liver function needs to be assessed three months after commencing therapy and again at 12 months. Patients should be monitored for medication compliance, tolerance, adherence, and adverse effects. If hyperlipidaemia is left untreated or undertreated, the condition is progressive and can lead to severe CVD, which can be fatal.
References
1. Shattat, G. A review article on hyperlipidemia: Types, treatments, and new drug targets. Biomed Pharmacol J 2014; 7 (2)
2. Hill M, Bordoni B. (2021). Hyperlipidemia. StatPearls Publishing. Available from: www. ncbi.nlm.nih.gov/books/NBK559182/
3. Mandal A. (2019). Cholesterol Physiology. In News, Medical Life Sciences. Available at: www.news-medical.net/health/Cholesterol-Physiology.aspx
4. Bermingham M. (2022). Managing cholesterol in the community setting. Irish Pharmacy News. January 2022
5. ESC/EAS (2019). Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The taskforce for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). European Heart Journal, Volume 41, Issue 1, 1 Jan 2020, Pages 111–188, https://doi. org/10.1093/eurheartj/ehz455
6. HSE (2020). Medicines Management Programme Preferred Drugs. Statin monotherapy for the treatment of hypercholesterolemia and prevention of cardiovascular events in adults. Health Service Executive. Available at: www. hse.ie/eng/about/who/cspd/ncps/medicines-management/latest-updates/statin-preferred-drug-report-july-2020.pdf
7. Ford I, Murray H, McCowan C, Packard C. Long-term safety and efficacy of lowering low-density lipoprotein cholesterol with statin therapy: 20-Year follow-up of West of Scotland coronary prevention study. Circulation. 2016 Mar 15; 133(11):1073-80
8. EMC (2022). Ezetimibe 10mg tablets. Medicines.org. UK. Available at www.medicines.org. uk/emc/product/8618/smpc#gref












Leave a Reply
You must be logged in to post a comment.