NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Theresa Lowry-Lehnen, GPN, RNP, CNS, PhD, PRO of the IGPNEA and Associate Lecturer at Institute of Technology Carlow
- 04th Jun 2021
Shot of a young woman sneezing in a pharmacy
One of the most common autoimmune conditions, allergic rhinitis can significantly impact quality-of-life, but a range of effective treatments are available
Allergic rhinitis (AR) is an inflammatory disorder of the nasal mucosa induced by immunoglobulin E (IgE)-mediated reactions to inhaled allergens. It is one of the most common chronic conditions globally causing a major health burden and is associated with substantial economic costs. AR often co-occurs with asthma and conjunctivitis and is also associated with atopic dermatitis and nasal polyps.
It is estimated that up to 50 per cent of people with asthma and up to 30 per cent of people with eczema also have AR. Classic symptoms of the disorder are nasal congestion, nasal itch, rhinorrhoea and sneezing. A less recognised symptom is post-nasal drip. AR is frequently associated with allergic conjunctivitis with redness, tearing, and itching of the eyes. Approximately 60 per cent of patients with AR have concomitant allergic rhino conjunctivitis. AR symptoms can be debilitating, resulting in sleep disturbance, fatigue, depressed mood and decreased function that impairs quality-of-life and productivity.
AR adversely affects the daily living activities of nearly 1.38 million Irish people and affects up to 30 per cent of adults and 40 per cent of children in industrialised countries. Approximately 80 per cent of individuals diagnosed with the condition develop symptoms before the age of 20 years. Older children have a higher prevalence than younger children with a peak occurring at ages 13-to-14 years. During early childhood, boys are more likely to be affected by AR than girls, during puberty girls have a higher incidence and by age 20 and over the prevalence rates among men and women are equal.
AR has long been considered a disorder of the nose and nasal passages, however, evidence suggests that it may represent a component of a systemic airway disease involving the entire respiratory tract. Allergen provocation of the upper airways not only leads to a local inflammatory response, but may also lead to inflammatory processes in the lower airways, and this is supported by the fact that rhinitis and asthma frequently co-exist. AR affects 60-to-80 per cent of people with asthma.
Some patients have AR alone, whereas others have AR and asthma with or without other allergic manifestations, although few patients have asthma alone. Although it is well established that rhinitis can lead to asthma, the exact phenotype of AR prone to developing asthma is still unclear. It is possible that poly-sensitised individuals can more commonly develop asthma.
Traditionally categorised as seasonal or perennial, AR is better classified according to symptom duration (intermittent or persistent) and severity (mild, moderate or severe). ARIA (Allergic rhinitis and its impact on asthma) guidelines classify AR as intermittent or persistent depending on the duration of symptoms, with persistent rhinitis occurring for more than four days a week for more than four weeks in a row and as mild, moderate or severe, depending on whether sleep and daily activities are affected or whether symptoms are troublesome.
Risk factors for AR include antibiotic use, inhalant and occupational allergens, as well as genetic factors. Common triggers include dust mites, animal allergens, pollens, spores, and moulds.
Pathophysiology
AR is an autoimmune condition and symptoms occur when the immune system overreacts to a normally harmless substance such as pollen. When the body encounters an allergen, cells in the lining of the nose, mouth and eyes release histamine-triggering symptoms of an allergic reaction. Allergic reactions do not occur the first time a person comes into contact with an allergen. The allergic immune response begins with a sensitisation phase when the patient is first exposed to an allergen without experiencing clinical symptoms.
In AR, numerous inflammatory cells, including mast cells, CD4-positive T-cells, B-cells, macrophages, and eosinophils, infiltrate the nasal lining upon exposure to an allergen. In allergic individuals, the T-cells infiltrating the nasal mucosa are predominantly Th2 and release cytokines, eg, interleukin [IL]-3, IL-4, IL-5, and IL-13 that promote immunoglobulin E (IgE) production by plasma cells. Crosslinking of IgE bound to mast cells by allergens, in turn, triggers the release of mediators, such as histamine and leukotrienes, which are responsible for arteriolar dilation, increased vascular permeability, itching, rhinorrhoea, mucous secretion, and smooth muscle contraction in the lung. The mediators and cytokines released during the early phase of an immune response trigger a further cellular inflammatory response, which results in the recurrent symptoms that often persist.
Diagnosis
Treatment
A thorough history and physical examination are important for establishing a diagnosis of AR. History should include questions regarding a family background of atopic disease, the impact of symptoms on quality-of-life and the presence of comorbidities, such as asthma, mouth breathing, snoring, sleep apnoea, sinus involvement, otitis media, and nasal polyps. Clinical history should note when and where symptoms occur and any exacerbating and relieving factors. Chest, ears, throat, abdomen and skin should be examined for other symptoms and a review of any treatments and their efficacy carried out.
Testing for allergen-specific IgE using skin prick or blood tests to identity the allergen can support the diagnosis. Other tests may include a nasal endoscopy, nasal inspiratory flow test, and CT scan. Rhinitis has important co-morbidities. Asthma should always be assessed for in patients with AR and if needed an objective measurement, such as spirometry, carried out owing to the frequent co-occurrence of these disorders. Patients should also undergo ear inspection as otitis media with effusion may be a co-morbidity in children with rhinitis and in adults with severe forms of rhinosinusitis.
The general examination should include skin examination for atopic dermatitis and assessment of thyroid function by checking for slow relaxation after the ankle jerk and for eye signs, such as puffiness, redness and/or bulging (hypothyroidism) in patients with obstructive rhinitis. Children’s growth should be assessed, as the combined use of INCS and inhaled corticosteroids can reduce height at high doses. The presence of features such as conjunctivitis, nasal allergic crease, allergic salute or double creases beneath the eyes all suggest an allergic diathesis. Nasal examination is required in patients with moderate to severe AR or in those with uncontrolled symptoms despite optimal treatment.
Examination should include assessment of the external appearance followed by internal examination, preferably with a nasoendoscope although an otoscope may suffice in children. Position of the nasal septum, size and colour of the inferior turbinates together with the appearance of the mucosa and the presence and nature of any secretions, polyps, bleeding, tumours, crusting or foreign bodies should be noted.
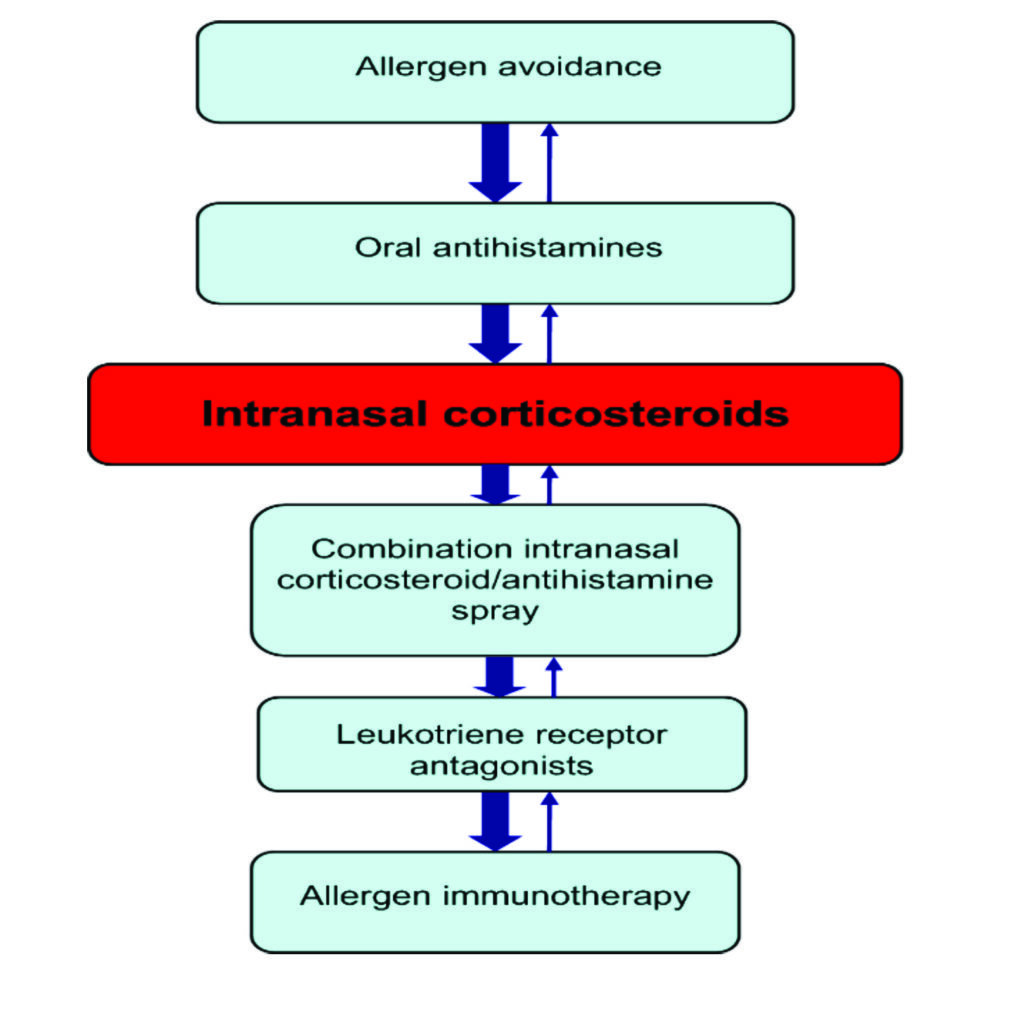
Figure 1: Stepwise treatment approach to allergic rhinitis
Treatment
Therapeutic options for AR include avoidance measures, nasal saline irrigation, oral antihistamines, intranasal corticosteroids, combination intranasal corticosteroid/antihistamine sprays, leukotriene receptor antagonists (LTRAs), and allergen immunotherapy. Other therapies that may be useful for some patients include decongestants and oral corticosteroids.
It is important to differentiate over-the-counter (OTC) and prescription therapies for AR. Nasal decongestant sprays are highly effective if used infrequently. Available options include Sudafed nasal spray (xylometazoline HCL), Otrivin (xylometazoline HCL), and Afrin (oxymetazoline HCL). Despite being available OTC, caution should be advised as incorrect use can lead to adverse effects. It is important that patients are aware that these decongestant sprays are not recommended for monotherapy in chronic AR.
First-line treatment of AR involves reduced exposure and avoidance of relevant allergens and irritants, such as house dust mites, moulds, pets and pollens, etc, that trigger the condition. Nasal saline irrigation is most effective when used for mild symptoms or before intranasal glucocorticoid (INGC) application. INGC options include Avamys, Nasonex, and Flixonase. If symptoms remain refractory to an intranasal glucocorticoid, a second generation oral antihistamine will be prescribed.
Second-generation oral anti-histamines such as loratadine and cetirizine are first-line pharmacological treatments recommended for all patients with AR. They require once-daily dosage, are non-drowsy and are available OTC without prescription. Second-generation antihistamines offer several advantages over classical H1 antihistamines, such as lack of sedation and impairment of performance, longer duration of action, and absence of anti-cholinergic side effects. However, loratadine is best avoided in elderly patients and patients with liver problems.
First-generation sedating antihistamines, such as diphenhydramine and chlorpheniramine, are also effective in relieving symptoms, however, they have been shown to negatively impact cognition and functioning, may affect the patient’s ability to drive and operate machinery and are not routinely recommended for the treatment of AR. They should not be used in patients with prostatic hypertrophy or narrow-angle glaucoma. The advantages of oral antihistamines are once-a-day administration, rapid and effective action and low cost. However, they are less effective than intranasal corticosteroids (INCS), particularly for nasal congestion which is a common symptom of AR.
Oral antihistamines are often sufficient for the treatment of mild AR, and many patients prefer oral medications to other formulations. Some oral antihistamines may, with caution, be used in pregnancy or in women who are breastfeeding for example, cetirizine. Other first-line therapeutic options for patients with mild persistent or moderate/severe symptoms are INCS and they can be used alone or in combination with oral antihistamines. When used regularly and correctly, INCS effectively reduce inflammation of the nasal mucosa and improve mucosal pathology. Studies and meta-analyses have shown that INCS are superior to antihistamines and leukotriene receptor antagonists in controlling symptoms of AR, including nasal congestion and rhinorrhoea.
INCS are not systemically absorbed. The most common adverse effects are local, including nasal irritation, stinging and epistaxis, and can usually be prevented by aiming the spray slightly away from the nasal septum. Long-term use does not damage nasal mucosa or induce glaucoma, and growth effects in children seem to be minimal. Some INCS, such as budesonide, can be safely used during pregnancy at the recommended therapeutic dose after a thorough medical evaluation.
If INCS are not effective, a combination corticosteroid/antihistamine spray, such as Dymista, can be used. LTRAs should be considered when oral antihistamines, INCS, and/or combination corticosteroid/antihistamine sprays are not well tolerated or are ineffective in controlling the symptoms of AR. For patients with AR refractory to INGCs and concomitant asthma, a trial of an LTRA, such as montelukast, is advised. If combination pharmacological therapy with oral antihistamines, INCS, combination corticosteroid/antihistamine sprays and LTRAs is not effective or is not tolerated, then allergen immunotherapy should be considered.
Immunotherapy
Allergen-specific immunotherapy (AIT) is currently the only potential treatment for allergies including AR that can modify the underlying course of the diseases. AIT is indicated for AR, allergic rhino-conjunctivitis and/or asthma when symptoms remain uncontrolled with avoidance measures and appropriate pharmacotherapy in adherent patients. The aim of AIT is to induce tolerance to the allergens and therefore reduce the symptoms of allergic diseases. By gradually increasing the patient’s exposure to the allergen that causes the allergy, the patient becomes tolerant to it. Immunotherapy is only used in patients with severe symptoms and must be done by a specialist. AIT for the management of allergic disease has entered a new phase.
Safe, effective, oral sub-lingual immunotherapy (SLIT) preparations are becoming increasingly available for use in allergy de-sensitisation as opposed to allergy injections. The use of AIT by ‘allergy shots/injections’ was severely curtailed in Ireland and the UK from 1986 when a number of deaths were reported with its use in general practice, particularly in those patients who had unstable underlying asthma. The situation has changed over the past decade however, with strong evidence that AIT can effectively treat AR , eradicate it and even prevent the development of asthma in allergic children if used early enough.
For a sustained effect, AIT should be applied for a minimum of three years, either continuously or pre-seasonally. Benefit may not appear until the end of the first year of treatment, but may persist for many years beyond the course of treatment. Prolonged desensitisation using increasing doses of the culprit allergen both by subcutaneous immunotherapy (SCIT) and SLIT reduces rhinitis symptoms which have been refractory to INGC and oral antihistamines. Grazax and Oralair are two licenced SLIT preparations available for grass pollen AR in Ireland.
If patients have co-existing asthma, it must be recognised and treated and their lung function test must be normal. Patients must be advised to place the tablet under the tongue for one-to-two minutes and then swallow it. Grazax should be commenced two-to-four months before the pollen season starts in late May/June and continued daily for a total of three years. Oralair is commenced at the same time for a period of six months per year for three successive years if there is an effect seen after the first season.
SLIT is now viewed as a significant advance in the treatment of allergic diseases. It is very effective in the treatment of rhinitis with long-lasting benefits seen after the treatment is discontinued. It is the only treatment that offers the possibility of reducing long-term costs and the burden of allergies by changing the natural course of the disease.
Other emerging therapies
Biological therapies represent a potential step forward in providing individualised care for patients with uncontrolled severe upper airway diseases. Biologics like omalizumab and dupilumab have demonstrated efficacy in patients with chronic AR and with nasal polyps. These monoclonal antibodies target type 2 inflammatory cytokines, including IL-4, IL-5, 1L-13 and IgE and have convincing evidence in proof of concept studies.
The immediate goals in biologic therapies for allergies and asthma are to develop biomarkers to identify patients most likely to respond to these therapies and to monitor disease severity. As experience with biological therapies continues to grow, they are expected to move from their current position as add-on therapies for severe allergic disease to play a more prominent role in treatment strategies for many more allergy patients.
House dust allergy tips
Allergy-proof covers for mattresses, duvets and pillows;
Choose wood or hard vinyl floor coverings instead of carpet;
Fit roller blinds that can be easily wiped clean;
Regularly clean cushions, soft toys, curtains and upholstered furniture, either by washing or vacuuming them;
Use synthetic pillows and acrylic duvets instead of woollen blankets or feather bedding;
Using a vacuum cleaner fitted with a high-efficiency particulate air (HEPA) filter can remove more dust than an ordinary vacuum cleaner;
Use a clean damp cloth to wipe surfaces – dry dusting can spread allergens further.
Pets
If a pet cannot permanently be removed from the house:
Keep pets outside as much as possible or limit them to one room, preferably without carpet;
Do not allow pets in bedrooms;
Wash pets at least once a fortnight;
Groom dogs regularly outside;
Regularly wash bedding and soft furnishings a pet has been on;
Taking an antihistamine one hour before entering a house with a pet can help reduce symptoms.
Pollen
To avoid exposure to pollen:
Check weather reports for the pollen count and stay indoors when it is high;
Avoid line-drying clothes and bedding when the pollen count is high;
Wear wraparound sunglasses to protect eyes from pollen;
Keep doors and windows shut during mid-morning and early evening, when there’s most pollen in the air;
Shower, wash hair and change clothes after being outside;
Avoid grassy areas, such as parks and fields, when possible;
If you have a lawn, consider asking someone else to cut the grass for you.
Mould spores
To help prevent mould spores:
Keep your home dry and well ventilated;
When showering or cooking, open windows, but keep internal doors closed to prevent damp air spreading through the house, and use extractor fans;
Avoid drying clothes indoors, storing clothes in damp cupboards and packing clothes too tightly in wardrobes;












Leave a Reply
You must be logged in to post a comment.