NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
An overview of the latest diagnosis, management, and prevention techniques for COPD.
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disease that is characterised by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.
The chronic airflow limitation that is characteristic of COPD is caused by a mixture of small airways disease (eg, obstructive bronchiolitis) and parenchymal destruction (emphysema), the relative contributions of which vary from person to person (GOLD, 2022).
In 2019, the National Institute for Health Research in the UK carried out a systematic review, which explored the prevalence of COPD from 1990-2019 in 65 countries. The study found that the global prevalence of COPD was 10.3 per cent in 30-to-79 year-olds; equivalent to 391.9 million people.
The study also found that the key risk factors for developing COPD include being male, current smoker, having a BMI of less than 18.5, exposure to biomass fuels, and occupational exposure to dust or smoke (Adeloye et al, 2022). Other contributing factors include genetic factors, lung growth and development, socioeconomic status, asthma and airway hyper-reactivity, chronic bronchitis, and infections.
A shift in the COPD paradigm
The paradigm of COPD as a predominantly male disease is changing as smoking rates in both males and females are now similar, and the number of deaths due to COPD among women has surpassed that of men. Women appear more susceptible to the effects of cigarette smoke, developing COPD earlier and with lower cigarette exposure than men. Women also commonly exhibit a COPD phenotype with airway dominant disease in comparison with emphysema and they also vary in response to treatment.
Diagnosis
The diagnosis of COPD involves a detailed history, spirometry, investigations, assessment of symptoms.
History
The patient history should include:
Medical and surgical history;
Smoking history include pack year history;
Occupational history.
Spirometry
Post-bronchodilator FEV1/FVC ratio of 70 per cent or 0.7 indicates COPD. Table 1 illustrates the severity of obstruction using FEV1.
Investigations
Blood screen to include FBC and TFTs;
Chest x-ray;
ECG.
In patients with FEV1/FVC <70%
GOLD 1
Mild
FEV1 > 80% predicted
GOLD 2
Moderate
50% < FEV1 < 80% predicted
GOLD 3
Severe
30% < FEV1 <50% predicted
GOLD 4
Very severe
FEV1 < 30% predicted
Table 1: GOLD (2022) classification based on FEV1
SCALE
SEVERITY OF DYSPNOEA
0
No breathlessness except with strenuous exercise
1
Shortness of breath when hurrying on the level or walking up a slight hill
2
Walks slower than people of the same age on the level because of breathlessness or has to stop for breath when walking at own pace on the level
3
Stops for breath after walking about 100 metres or after a few minutes on the level
4
Too breathless to leave the house or breathless when dressing or undressing
Table 2: Medical Research Council dyspnoea scale
Eosinophils, FENO testing, and COPD
The measurement of fractional inhaled nitrous oxide (FENO) is a relatively new concept and is now recommended as one of the tools to assess if inhaled corticosteroid therapy (ICS) is indicated for these patients. Approximately 40 per cent of patients with COPD have raised eosinophils. Patients with high eosinophil levels have an increased risk of exacerbations of COPD if they are not on ICS therapy.
Assessment of symptoms
The characteristic symptoms of COPD are chronic and progressive dyspnoea, cough, and sputum production that can be variable from day-to-day. Dyspnoea is usually progressive, persistent, and characteristically worse with exercise. Patients may have an intermittent cough, which may be unproductive, but many patients will commonly cough up white/ clear non-purulent sputum. Symptoms and their impact on quality-of-life can be assessed using the COPD assessment tool (CAT) test and the Medical Research Council Dyspnoea (MRC) scale (Table 2). The CAT test is a validated eight-item measure of health status impairment in COPD (www.catestonline.org).
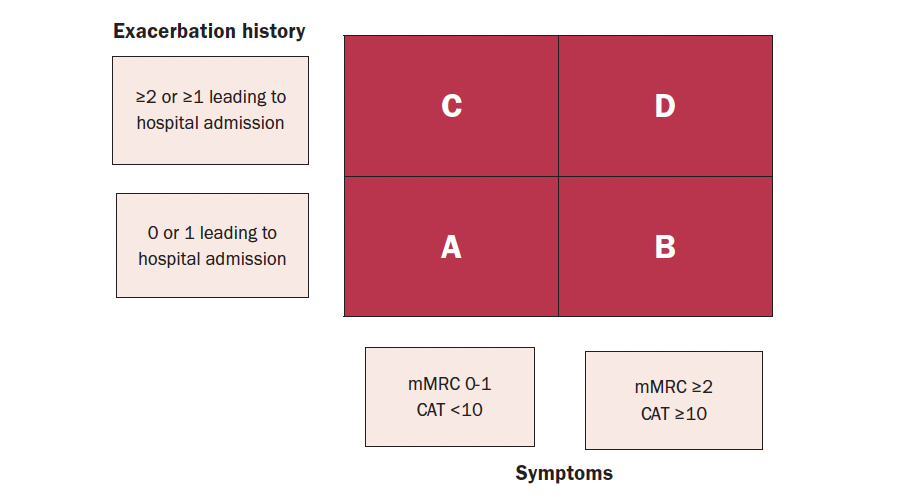
ABCD assessment tool
The ABCD assessment tool is a useful tool for assessing severity of COPD. The assessment of COPD has been refined to include assessment of symptoms and risk of future exacerbations (Figure 1).
Figure 1: The revised ABCD assessment tool (GOLD)
Pharmacological treatment
Pharmacological therapies are used to reduce COPD symptoms, reduce the severity and frequency of exacerbations, and improve exercise tolerance and health status.
Bronchodilator therapy remains the mainstay of the management of stable COPD and has been shown to reduce hyperinflation.
The main groups of COPD medications include:
Beta-agonists – these relax smooth muscle by stimulating the beta2 adrenergic receptors. Beta-agonists can be classified into short-acting (SABA) and long-acting (LABA); eg, salbutamol (SABA), salmeterol (LABA), indacaterol (LABA), vilanterol (LABA), formoterol (LABA), olodaterol (LABA).
Antimuscarinic drugs block the bronchoconstrictor effects of acetylcholine on M3 muscarinic receptors. These can also be classified into short-acting (SAMA) and long-acting (LAMA); eg, ipratropium (SAMA), tiotropium (LAMA), umeclidinium (LAMA), aclidinium bromide (LAMA), glycopyrronium (LAMA).
Combining bronchodilators may increase the degree of bronchodilation, whilst lowering the risk of side-effects compared to increasing the dose of a single bronchodilator agent.
Methylxanthines – this group of drugs remain controversial as to their mechanism of action. There is evidence of bronchodilation in stable COPD. Theophylline is the most commonly used methylxanthine. However, there are significant drug interactions with its use and clearance of the drug declines with age.
ICS should not be used as a single agent in the management of COPD. In patients with moderate to severe COPD, the use of ICS combined with a LABA is more effective than using either agent alone in improving lung function, health status and reducing exacerbations. Their use in patients with high eosinophil levels have been shown to be beneficial (GOLD, 2022).
To-date, there is no conclusive clinical trial evidence that any existing medications for COPD modify the long-term decline in lung function (GOLD, 2022).
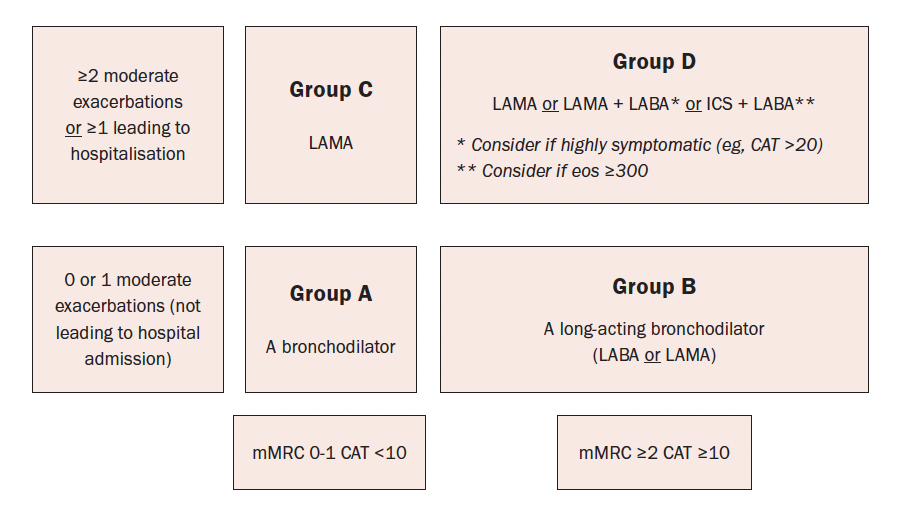
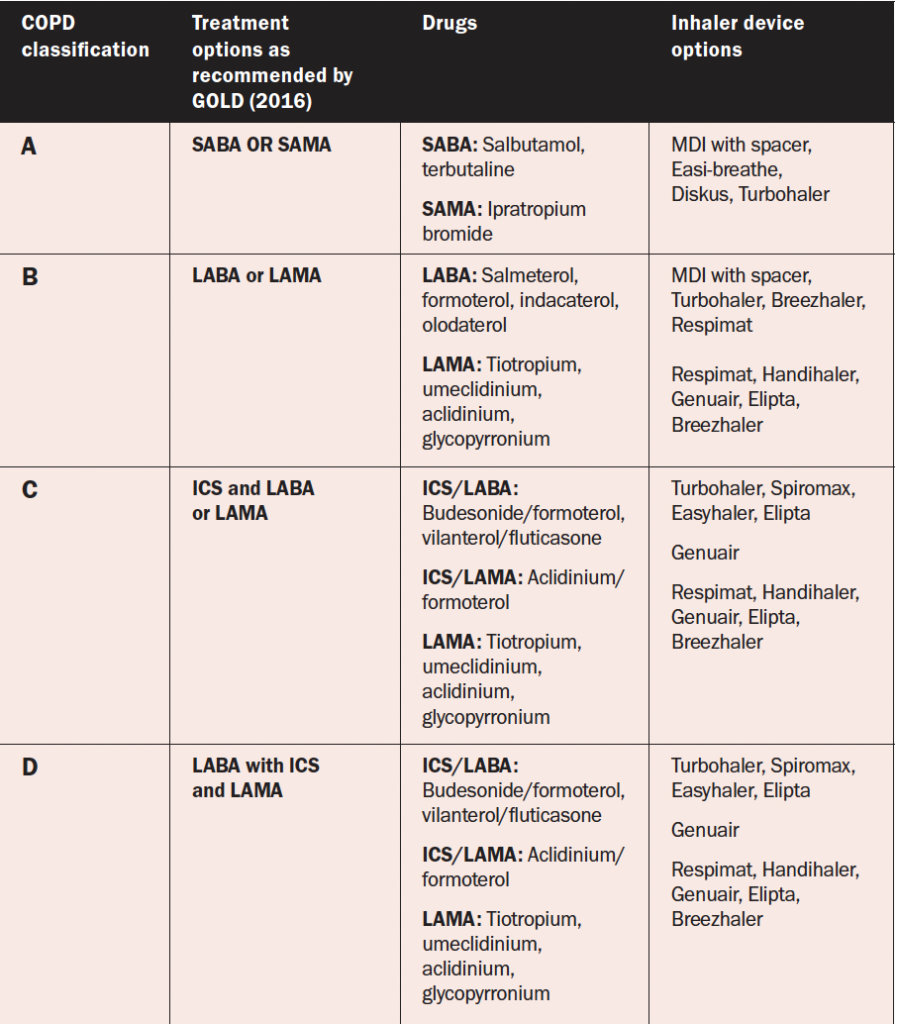
Pharmacological algorithms are given for the initiation, escalation, or de-escalation of treatment according to the individual assessment of symptoms and exacerbation risk. In previous publications of GOLD reports, recommendations were only given for treatment initiation. Table 3 illustrates the pharmacological treatment options according to the patient’s COPD classification.
Inhaler technique
The assessment of inspiratory effort is important to ensure that the patient has sufficient inspiratory flow to optimise deposition of medication to the lungs. Inspiratory effort can be assessed using the In Check Dial metre. Inhaler devices have different inspiratory flow requirements, with dry powder devices requiring a greater effort that soft mist or metre dose inhalers. To improve technique, it is recommended that patients are educated and trained with the appropriate devices. The choice of device should be tailored to the individual, depending on the patient’s ability to use it, their manual dexterity, cognitive function, and taking their preference into account.
Ongoing monitoring and follow-up
GOLD (2022) recommends that regular review of COPD should focus on dyspnoea and exacerbations. Whichever is the most problematic for the patient should be the focus of the review. For patients with persistent breathlessness or exercise limitation on LABA/ICS treatment, LAMA can be added to escalate to triple therapy. Alternatively, switching from LABA/ICS to LABA/LAMA should be considered if the original indication for ICS was inappropriate (eg, an ICS was used to treat symptoms in the absence of a history of exacerbations), or there has been a lack of response to ICS treatment, or if ICS side-effects warrant discontinuation (GOLD, 2021). At all stages, dyspnoea due to other causes (not COPD) should be investigated and treated appropriately. Inhaler technique and adherence should be considered as causes of inadequate treatment response.
Where exacerbations are the predominant trait, prophylactic macrolide antibiotics should be considered following cardiovascular assessment. Assessment of eosinophils can be useful when the patient is experiencing exacerbations. If the eosinophils are above 0.3 or 0.1 if the patient has experienced two or more exacerbations with one hospitalisation, initiating or escalating ICS can be beneficial (GOLD, 2021). Roflumilast, another treatment option, is a selective inhibitor of phosphodiesterase-4 (PDE-4) that has unique anti-inflammatory activity and is used to treat and prevent exacerbations.
Non-pharmacological measures
1. Smoking cessation
Smoking cessation is of paramount importance in the management of COPD regardless of disease severity. Support given by health professionals significantly increases quit rates over self-initiated strategies. Even a brief (three-minute) period of counselling to urge a smoker to quit results in smoking quit rates of 5-to-10 per cent. Smoking cessation should be encouraged at all severities of the condition. Nicotine replacement therapy (nicotine gum, nasal spray, transdermal patch, sublingual tablet, or lozenge) as well as treatment with varenicline reliably increases long-term smoking abstinence rates and are significantly more effective than placebo (GOLD, 2022).
Figure 2: Initial pharmacological treatment with the ABCD assessment tool (GOLD, 2022)
2. Pulmonary rehabilitation
Pulmonary rehabilitation has been proven to show significant benefits in reducing dyspnoea, fatigue and exacerbations and improving quality-of-life in people with COPD. Although an effective pulmonary rehabilitation programme is six weeks, the longer the programme continues, the more effective the results. If exercise training is maintained at home, the patient’s health status remains above pre-rehabilitation levels (McCarthy et al, 2015).
3. Exercise
Patients should be encouraged to be as physical active as possible. The aim is to achieve 30 minutes of aerobic activity daily, eg, walking, cycling, and swimming. Exercises such as chest and shoulder exercises, shoulder raises, step ups, and sit-to-stand exercises should be encouraged as this will assist in maintaining upper body strength with the ultimate aim of prevention of muscle wasting.
4. Breathing exercises and energy conservation
Breathing exercises such as pursed-lip breathing and the active cycle of breathing can help manage dyspnoea and assist in expectorating sputum. These techniques are available on www.copd.ie.
Energy conservation is based on the 4Ps:
Prioritise
Make a list of what you have to do;
Place the task in order of importance, into what you need to do, want to do, and should do;
Get rid of any unnecessary tasks;
Decide if someone else can do some tasks for you;
Change between light and heavy tasks.
Pacing
Work at a slow steady pace;
Allow plenty of time for rest and relaxation, at least five-to-10 minutes every hour;
Use breathlessness as a guide;
Space difficult and heavy tasks evenly throughout the week.
Planning
Change the activities to keep the energy you use low to do the job;
Sit rather than stand when possible, use a perching or high stool when possible;
Organise yourself, your home, and your working environment;
Put items you frequently use in an easy to reach place;
Consider using a bag or basket to carry things;
Plan tasks around when help is available and when your energy levels are high.
Posture
Push or pull objects, rather than lifting;
Use your legs, not your back;
Use your strongest, largest joints;
Keep your arm movements at a low rate;
Avoid bending, reaching or twisting.
5. Education
Patients require ongoing education and support to assist them to live and maintain optimal lifestyles. Education about the disease process, inhaler technique, adherence to medication, immunisations, pulmonary rehabilitation, smoking cessation, and long-term oxygen therapy are required. All patients should have a COPD communication card, which outlines their treatment, including oxygen therapy, and gives guidance on how to recognise worsening COPD. (Available at www.COPD.ie)
Table 3: Pharmacological treatment options based on COPD classification (GOLD, 2022)
Oxygen therapy
Long-term oxygen therapy is indicated for stable patients who have:
PaO2 at or below 7.3kPa (55mmHg) or SaO2 at or below 88 per cent, with or without hypercapnia confirmed twice over a three-week period; or
PaO2 between 7.3kPa (55mmHg) and 8.0kPa (60mmHg), or SaO2 of 88 per cent, if there is evidence of pulmonary hypertension, peripheral oedema suggesting congestive cardiac failure, or polycythaemia (haematocrit >55 per cent).
Once placed on long-term oxygen therapy (LTOT) the patient should be re-evaluated after 60-to-90 days with repeat arterial blood gas (ABG) or oxygen saturation while inspiring the same level of oxygen or room air to determine if oxygen is therapeutic and still indicated, respectively (GOLD, 2022).
Management of co-morbidities
Many patients with COPD have co-existing illness such as diabetes, cardiovascular disease, osteoporosis, and depression to mention but a few. In general, the presence of co-morbidities should not affect COPD treatment and co-morbidities should treated according to standards and guidelines. Lung cancer is common in patients with COPD due to smoking history. About 50 per cent of patients who experience exacerbations of their COPD and require hospital admission have undiagnosed cardiovascular disease (Steer et al, 2022). Addressing this reduces subsequent admissions to hospital. It is recommended that these patients should have an echocardiograph, BNP and cardiac MRI. Gastroesophageal reflux is common and is associated with an increased risk of exacerbations and therefore should be managed optimally. Osteoporosis is common due to recurrent use of oral steroids, lack of weight-bearing exercise, smoking, and being over or underweight. GOLD recommends that treatments for co-morbidities should be kept as simple as possible to avoid polypharmacy (GOLD, 2022).
Conclusion
This article has focused on the diagnosis, management, and prevention of COPD. The definition, classification, pharmacological, non-pharmacological, the importance of inhaler technique, and co-morbidities have been addressed. There have been significant changes to the assessment tool which has simplified the classification of COPD, which will enable practitioners to individualise the patient’s management and treatment, and ultimately improve patient outcomes and quality-of-life.












Leave a Reply
You must be logged in to post a comment.