NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Mary Kearney, Dr Martin Ruttledge and Ms Esther Tomkins
- 11th Jun 2023
New daily persistent headache (NDPH) is a not uncommon form of chronic daily headache (CDH) and is increasingly recognised in specialised headache clinics (Kearney 2019). It is also occasionally seen in primary care in adults and children. In recent years, it is being diagnosed much more often, as headache specialists and primary care physicians become aware of the existence of this unusual headache disorder, which was first described in 1986.
NDPH is a neurological condition that typically starts abruptly (over hours or days) and often continues for many months or even years. The day or week of onset is clearly remembered in approximately 80-to-90 per cent of cases and is considered to be a cardinal feature of this disorder. Clinically, NDPH can be a very debilitating neurological disorder, as it is often unremitting, can be severe on a daily basis, and is frequently refractory to standard headache/migraine treatments. Internationally, psychology and/or psychiatry input is often additionally sought by neurologists, due to the persistent and debilitating nature of this unusual condition.
In our experience, neurologists and clinicians who specialise in headache disorders generally see far more patients each year with NDPH than with cluster headache. However, the exact prevalence of NDPH is unknown. In one report from 2017, NDPH was diagnosed in 0.4 per cent of an adult population of patients from Estonia.
Since the awareness of this condition is increasing and the third version of the International Classification of Headache Disorders (ICHD) (published in 2018) has broader criteria for NDPH, the prevalence of NDPH is likely to increase.
Aetiology
The aetiology of NDPH is unknown, but a number of theories have been proposed. However, no universally-accepted cause or mechanism of onset has been identified or accepted internationally. Approximately half of all patients appear to have a trigger or provoking factor such as stress or a flu-like illness.
The natural history of NDPH is considered to be two-fold:
1) A self-limiting subtype that typically resolves spontaneously within one-to-two years.
2) A refractory or persistent subtype that continues for several years.
In headache clinics, we tend to see the latter subtype more frequently, and, unfortunately, it does not typically respond well to standard or conventional treatment regimens. NDPH, going by the name, is generally an unremitting continuous disorder, but there are reports of relapsing remitting variants in some individuals. In terms of the headache location, it can be unilateral or bilateral.
In our experience, most patients with NDPH have an associated migraine phenotype and can display common migraine symptoms, especially with worsening or exacerbations of their daily symptoms. Many of these patients have a prior history of (infrequent) episodic migraine or a strong family history of migraine. These patients appear therefore to have dual biological phenotypes, with one condition likely to be exacerbating or aggravating the other. The diagnosis in these cases can be referred to variously as:
NDPH with migrainous features;
NDPH with a migraine phenotype;
Chronic migraine disorder with a new daily persistent onset.
Currently, NDPH is listed as a primary headache disorder, and is separate from migraine in the ICHD. There are also patients with NDPH who have a more featureless or bland clinical phenotype (tension type-variant).
In a review of NDPH in 2019 by Yamani and Olsen, it was found that NDPH is:
More common in children and adolescents.
More common in women.
Mostly bilateral in location.
Associated with a 30-to-50 per cent family history of unspecified headache disorders.
Associated with several co-morbid symptoms or conditions including sleep disturbance, light-headedness, blurred vision, neck stiffness, concentration problems, sensory disturbance, such as numbness or tingling, vertigo, lethargy, and other non-specific syndromes.
Possible precipitating causes of NDPH
Post-viral headache is a well-recognised phenomena and was repeatedly documented after the ‘Russian or Asiatic flu’ in the 1890 pandemic. There may therefore be a common theme with viral infections and the body’s long-term response to these agents.
Prior to Covid, in a review by Rozen (2018), an associated potential precipitating factor or possible triggering factor was found in approximately 50 per cent of NDPH cases:
Infection and flu-like symptoms were noted in 22 per cent of cases. However, one must consider that mild respiratory infections are very common in the general community. Covid-19 appears to be the most recent reported infective trigger factor for NDPH.
Stressful life events were recorded in 9 per cent of patients. Again, stress is very common in the general population and therefore may not have a causative link.
Surgical procedures with intubation appeared to trigger a further 9 per cent of cases. Such procedures are relatively rare each year in terms of overall lifespan and therefore this may be a significant factor.
Given that stress and infection were considered the most common causes for NDPH prior to Covid-19, one can easily see how Covid-19 could be implicated in the causation of NDPH since 2020.
Covid-19 and headaches
Headache can present as the first symptom of Covid-19 infection and is a significant clinical feature of 10-to-30 per cent of those hospitalised with this viral infection. Since April 2020, reports have emerged of some patients developing NDPH or ‘NDPH-type symptoms’ after having Covid-19.
A December 2020 review article from the UK found that one-in-10 people who have had Covid-19 had persistent symptoms that lasted longer than 12 weeks. Headache and dizziness are the most common neurological symptoms associated with long-term effects of Covid-19, (‘long Covid’ – more than four weeks) or post-Covid-19 syndrome (more than 12 weeks).
Additional clinical symptoms associated with NDPH after Covid-19 include lack of smell/taste and persistent gastrointestinal symptoms (Uygun 2020). As for all patients with NDPH, the headache is more often bilateral and is typically analgesic or treatment resistant.
Investigations for those with a clinical diagnosis of NDPH
As with all of these neurological (headache/migraine) conditions, the diagnosis is based on history, general examination, and appropriate investigations. Neuroimaging studies are generally unremarkable. However, it is important to rule out other secondary conditions, which are considered to be NDPH mimics. Therefore, the following tests may need to be undertaken:
MRI brain and cervical spine with contrast (possible CSF leak).
Intracranial magnetic resonance venogram (MRV) to rule out central cerebral venous sinus thrombosis.
From a general practice perspective, most doctors would not be familiar or have seen a case of cerebral venous thrombosis (CVT) prior to the Covid-19 pandemic, as it is a very rare condition and an uncommon cause of headache. In fact, headache specialists would infrequently see this condition. It is usually diagnosed clinically by a general neurologist or physician in the acute hospital setting and confirmed by contrast-enhanced MRI and intracranial MRV. However, CVT has now become a household term because of the increased risk of this condition with Covid-19 infection and the very rare association with Covid-19 vaccines.
Reported cases of central venous sinus thrombosis per million population
Headache is present in 80-to-90 per cent of those who have CVT and it is also the most frequent inaugural symptom. The headache has no specific characteristics (Olsen 2018), but it is often:
Diffuse, progressive, and severe;
Or unilateral and sudden (even thunderclap);
Or mild and sometimes migraine-like.
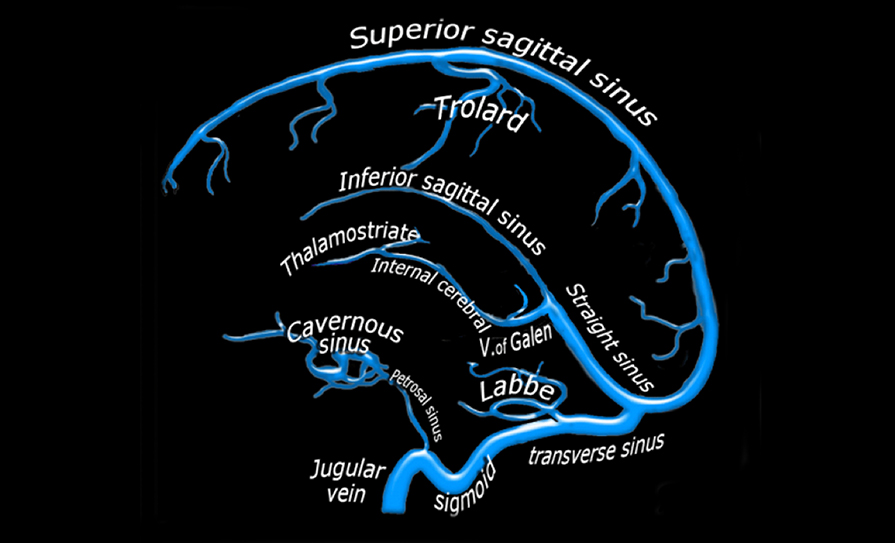
Major sinus (veins) in the brain
In over 90 per cent of cases, CVS is associated with:
Focal neurological symptoms or signs including visual deficits, seizures; and/or
Signs of intracranial hypertension;
Subacute encephalopathy; or
Cavernous sinus syndrome (CSS), which is a rare condition. (It is characterised by ophthalmoplegia, proptosis, ocular and conjunctival congestion, trigeminal sensory loss, and Horner’s syndrome).
In 2020, there was a case report documenting a patient with Nutcracker syndrome by Stubberud, who presented with abdominal pain, food intolerance, and an NDPH phenotype headache clinically. This is a very unusual association, but this case highlights the complexity of this condition and the potential for mimics and secondary causes of NDPH.
Nutcracker syndrome results most commonly from the compression of the left renal vein between the abdominal aorta and superior mesenteric artery, although other variants exist. It can cause many symptoms in both children and adults, such as flank pain and blood in the urine. Rarely is headache the presenting sign. Common treatments for Nutcracker syndrome include stenting, surgery, and routine urine tests.
Treatment of NDPH
Internationally, the best treatment options for NDPH are not clear or consistent, and unfortunately there is no standard of care. This is mainly because most standard or conventional migraine treatments have limited benefit, or are only helpful in a small fraction of cases. The goal of treatment in headache disorders generally is to try and achieve as many, completely symptom-free (crystal clear) days as possible each month for patients or to reduce the severity by at least 50 per cent (with concomitant improvement in quality-of-life).
As there are no international or European standard evidence-based guidelines for treatment, a sensible approach is to treat these conditions as one would do for the nearest headache phenotype. The position with medication overuse is unclear, but it should be borne in mind in these patients as overuse of painkillers or acute medication make it difficult to make the diagnosis of NDPH. Medication overuse usually causes more harm than good, even in NDPH.
Many NDPH patients do improve in terms of severity and disability with a combination of treatments including:
Oral prophylactic medications (such as topiramate, venlafaxine, nortriptyline, or amitriptyline);
Inpatient treatment with dihydroergotamine or lidocaine;
More recently the novel CGRP monoclonal antibodies (especially in patients with significant migrainous features). The CGRP monoclonal antibodies are not widely available in Ireland at the time of writing. They can only be prescribed by some neurologists after a person has failed to respond to three different preventative drugs.
When to refer NDPH to secondary care
If NDPH is suspected in primary care, bearing in mind that the diagnosis can only be made after three months of continuous headache and associated symptoms, the patient should be referred to an appropriate specialist clinic for diagnostic confirmation, appropriate investigations, and guidance on future management (including non-pharmacological treatments and a multidisciplinary approach to care).
In the Republic of Ireland, there are five established migraine/headache clinics or services (Beaumont, Mater, and St Vincent’s Hospitals, Dublin; and Cork and Galway University Hospitals), and there are pilot clinics/services in Tallaght University Hospital and St James’s Hospital, Dublin (supported by Sláintecare funding). In addition, the Migraine Association of Ireland provides support and advice for headache/migraine sufferers.
There is an unmet need for additional multidisciplinary services with a specialist neurologist, specialist nurses, psychologists, and other ancillary healthcare professionals. It is important that physicians in primary care and hospital settings recognise NDPH early. They will then be able to advise patients about this complex disorder and refer them to the appropriate specialist for investigations and management in the medium- to long-term.
References
Olesen J, Bendtsen L, Dodick D, Ducros A, Evers S, First M, et al. The International Classification of Headache Disorders 3rd Edition; International Headache Society 2018
Kearney M, Ruttledge M, Tomkins E. Migraine: Diagnosis and management from a GP perspective. 2019. www.icgp.ie
Elrington GE. Tension type headache is dead; long live chronic migraine. J Headache Pain. 2013 14 (1) P48
Al-Hashel JY, Ahmed SF, Alroughani R, Goadsby PJ. Migraine misdiagnosis as a sinusitis, a delay that can last for years. J Headache Pain. 2013 14:97
Papetti L, Sforza G, Tarantio S, Moavero R, Ruscitto C, Ursitti F, et al. Features and management of new daily persistent headache in developmental-age patients. Diagnostics. 2021;11:385
Yamani N, Olsen J. New daily persistent headache: A systematic review on an enigmatic disorder. J Headache Pain. 2019 20:80
Rozen T. Triggers may guide treatment of new daily persistent headache. Neurology Reviews from 8th Annual Scientific meeting on the Southern Headache Society. 2018 26 (11)53-4
Venkatesan P. NICE guideline on long Covid. Lancet Respir Med. 2021 Feb;9(2):129
Rozen T. Daily persistent headache after a viral illness during a worldwide pandemic may not be a new occurrence: Lessons from the 1890 Russian/Asiatic flu. Cephalalgia. 2020;40(13) 1406-09
Uygun Ö, Ertas M, Ekizoglu, Bolay H, Özge A, Orhan EK, et al. Headache characteristics in Covid-19 pandemic – a survey study. J Headache Pain. 2020 21:21
National Institute for Health and Care Excellence. Covid-19 rapid guideline: Managing the long-term effects of Covid-19. December 2020. www.nice.org.uk/guidance/ng188
Stubberud A, Cheema S, Tronvik E, Matharu N. Nutcracker syndrome mimicking new daily persistent headache: A case report. Cephalalgia. 2020 40 (9) 1008-11
Nagel MV, Cavanagh S, Olivier M, Larripa N, Gutierrz T, Grandinette M, et al. Frequency of diagnosis in a specialised headache clinic in Buenos Aires. 2019. International Headache Conference
DR MARY KEARNEY, GP with extended role in headache; DR MARTIN RUTTLEDGE, Headache Neurologist, Beaumont Hospital, Dublin; and MS ESTHER TOMKINS, Advanced Nurse Specialist, Beaumont Hospital













Leave a Reply
You must be logged in to post a comment.