NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Dr Robert Harrington explores this common presentation in general practice, providing best practice guidance on management and when to refer for expert input
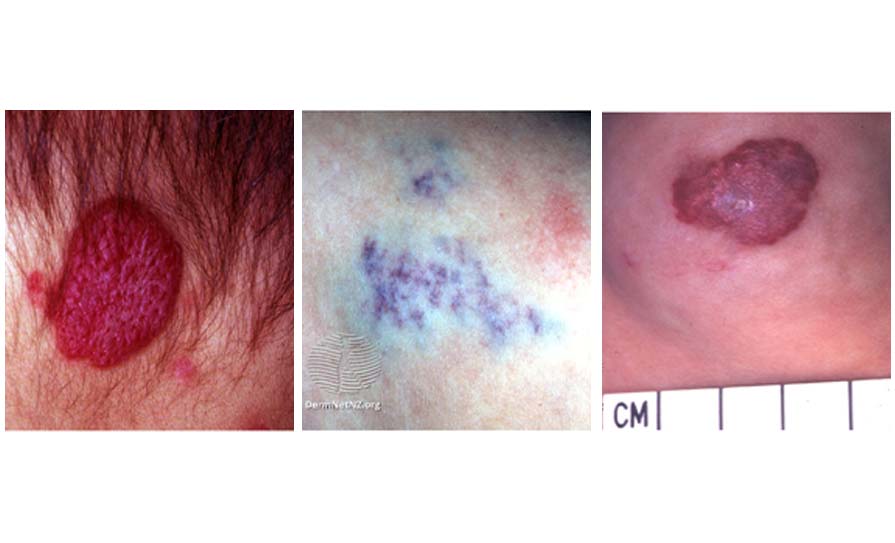
Infantile haemangiomas (IH), commonly known as strawberry birthmarks or strawberry naevi, are benign vascular tumours that occur in approximately 5 per cent of Caucasian infants. They are more common in females and their incidence is increased in pre-term infants as well as in twins. There is a genetic component, with a family history of IH being reported in about a third of cases. IH can be classified as superficial, deep, or combined based on their depth within the skin and their clinical appearance. The classic, strawberry-like, bright-red nodule or plaque is the most easily identified type of IH and represents the superficial subtype. Deep IH are raised, skin-coloured nodules and often have a blueish hue. Combined haemangiomas have features of both superficial and deep haemangiomas. Multiple lesions occur in up to 20 per cent of cases and are more commonly seen in twins.
Segmental haemangiomas are a rarer subtype of IH which are occasionally associated with certain neurovascular syndromes, dysraphisms, and other structural anomalies. Segmental lesions are generally plaque or patch-like and cover a specific cutaneous territory. PHACE (posterior fossa anomalies, haemangioma, arterial anomalies, cardiac anomalies, and eye anomalies) syndrome is the most common such condition, but fortunately is quite rare.
Natural progression
In most cases, IH are uncomplicated and follow a predictable clinical course. They are usually first noted by a parent or physician in the first few days of life. It is important to note that a haemangioma which is clearly present at birth may represent a congenital haemangioma rather than an IH. Work-up, management, and potential complications of congenital haemangiomas are different from those associated with IH and should thus be managed by paediatricians or dermatologists with expertise in the area.
After being noticed in the days to weeks after birth, IH will usually go through a rapid proliferation phase. During this period, the lesion grows quickly, often increasing in both diameter and height. Generally, this proliferative phase continues for three months, and in most cases, is completed by six months. At around one year of age, spontaneous involution of the haemangioma begins to occur. The earliest sign of involution is often a colour change from bright- red to a darker red or purple. Often a lighter grey colour can start to appear centrally as the lesion begins to shrink. Deep IH become less blue during involution. Unlike the proliferative phase, involution is a long and slow process which continues over years rather than months. The vast majority of IH have completely involuted by age four with rare cases taking a little longer. Up to 50 per cent of patients will have some residual change in the area after resolution of the lesion. These are very often quite subtle, but include scarring, atrophy, telangiectasias, and discolouration. Larger and pedunculated lesions are more likely to lead to these sorts of changes.
Thankfully, most IH are uncomplicated and require no intervention outside of parental reassurance
Complications
Thankfully, most IH are uncomplicated and require no intervention outside of parental reassurance. However, approximately 12 per cent will be associated with some complications, the most common of which is ulceration. Ulceration of an IH is extremely painful and greatly increases the risk of permanent scarring. Early signs of impending ulceration include darker, haemorrhagic-looking spots inside the lesion, or a greyish-white discolouration. Any sign of skin breakdown or ulceration warrants urgent review and often requires hospital admission for analgaesia and dressings. Other potential complications arise when IH affect internal structures.
Airway haemangiomas are commonly associated with segmental haemangiomas of the face or neck area, but can occur in isolation, or in patients with multiple other inoffensive haemangiomas. The obvious concern in these cases is that of airway obstruction. If airway haemangiomas are suspected, a diagnosis should be made via laryngoscopy and they should be aggressively treated.
Outside of the airway, IH are sometimes present in the liver. A large burden of hepatic haemangiomas can lead to high-output cardiac failure, abdominal compartment syndrome, and consumptive hypothyroidism. Another potential complication of cutaneous IH is impairment of normal growth or function of adjacent structures. A large periorbital haemangioma, for example, can compromise the development of normal vision. Mass effect can cause astigmatism, ptosis, proptosis, and strabismus.
Cosmetic concerns arise when haemangiomas appear on the face or on the breasts in females. Scarring, atrophy, and telangiectasias are possible, particularly after large haemangiomas. Lesions near the ear can lead to asymmetrical growth of one ear and may obstruct the auditory canal. Any haemangioma that is likely to be complicated in any of these ways warrants treatment as early as possible.
Figure 1: From top to bottom: Superficial, deep, and mixed type haemangiomas. Images from Dermnet NZ
Treatments
Prior to 2007, the treatment options for IH were limited and often disappointing. Corticosteroids were the mainstay of treatment with other options including interferon alpha-2a, vincristine, and plastic surgery. The discovery of propranolol as a treatment for IH is a great tale of medical serendipity. In 2007 in France, an infant was being treated for a nasal IH with corticosteroids. The patient developed iatrogenic obstructive cardiomyopathy secondary to the steroids and was thus treated with propranolol. A very obvious and rapid change was noted in the colour and size of the haemangioma and after withdrawal of the corticosteroids, it continued to flatten and shrink. A second child had a plaque-like IH affecting the right upper arm and face. MRI showed intraconal and extraconal orbital involvement. Echocardiography showed high output failure due to the large burden of haemangiomas and propranolol was commenced. Once again, a huge improvement in the haemangiomas was noted. The French team then trialed propranolol in nine further patients with severe or disfiguring IH. Clinical and ultrasonographic improvement was seen in all patients.
Propranolol has now become the first-line treatment for IH that require intervention, as it quickly shrinks the lesion and reduces the risk of associated complications. It is dosed according to weight and age, and treatment is generally initiated by dermatologists or paediatricians in an inpatient setting. The reason for commencing propranolol in hospital is to monitor for bradycardias, hypotension, and hypoglycaemia, which can occur in a small number of infants. Once the patient has been safely commenced on the medication, they can continue treatment at home, with regular follow-up to assess for complications of the haemangioma, medication adverse effects, and dose adjustment of the propranolol.
In general, propranolol is well-tolerated, but other side-effects include sleep disturbance, gastrointestinal upset, and cool peripheries. There is a drug interaction between propranolol and lidocaine, which leads to increased effect of lidocaine. For this reason, parents are warned not to use lidocaine-containing teething gels concomitantly with propranolol. Treatment is usually continued until around one year of age, at which point natural involution should begin. On stopping the medication, there can often be slight recurrence or increase in size of the haemangioma. If the recurrence is significant, then the course of propranolol can be extended as needed. Options outside of propranolol include topical beta blockers such as timolol. As a topical treatment, it is likely slightly less effective, but has fewer side-effects. However, the side-effects are largely similar to those seen with propranolol, suggesting that the drug still has a systemic effect.
The decision of whether or not to refer a patient with an IH to a specialist centre can be a difficult one
The IHReS
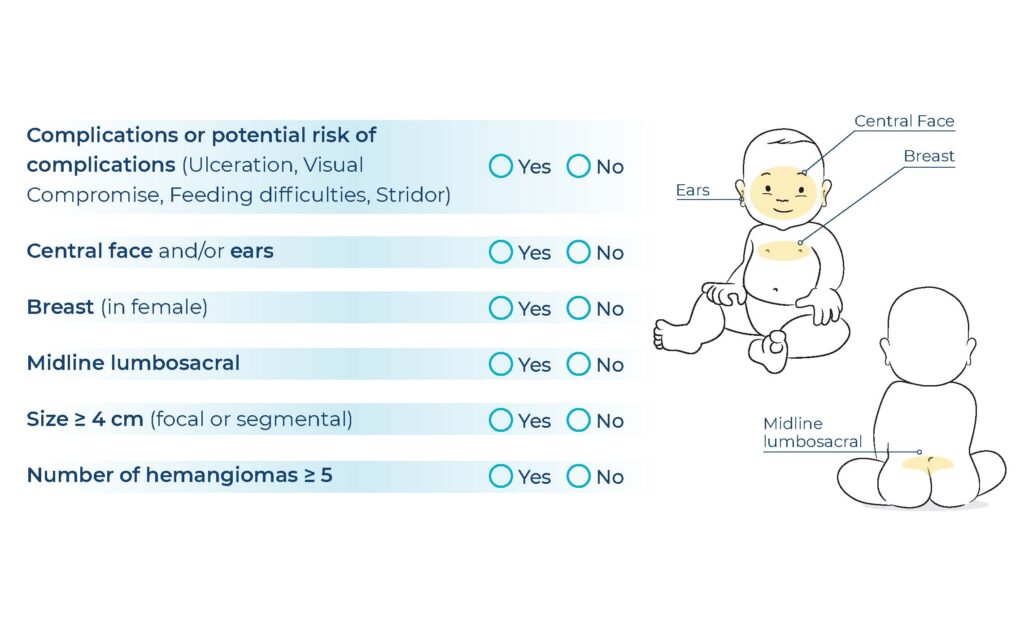
The decision of whether or not to refer a patient with an IH to a specialist centre can be a difficult one. By default, the patients are infants and because of their appearance, haemangiomas can often cause significant parental anxiety. In 2019, a useful scoring system to aid physicians with this decision was designed and validated. The Infantile Haemangioma Referral Score (IHReS) is a simple, six-question scoring system, which is available as a handy online tool (Figure 2). The six questions refer to location, size, and number of haemangiomas. If the answer to any of the six questions is yes, then, quite simply, the patient should be referred. If all the answers are no, there are some follow-up questions regarding size of the IH and age of the patient.
Figure 2: The Infantile Haemangioma Referral Score. A handy online version can be found at www.ihscoring.com
The tool is quick and easy to use and is useful in aiding physicians in the decision-making process. As well as identifying which patients require referral, the score is also useful for identifying those that can be safely managed in the community. A recent study performed in University Hospital Galway looked at the use of the IHReS by referring clinicians, and the potential benefits that an uptake in its use may have. Six months of new IH referrals were analysed and the IHReS was retrospectively applied to each case. The study showed that 39 per cent of IH referred to the paediatric dermatology clinic did not meet the IHReS criteria for referral. The majority of these patients were re-assured and discharged after one clinic visit. The remainder received further follow-up due to parental concerns or unclear diagnosis. None of the patients required treatment. The study shows that increased use of the IHReS may reduce some of the burden on the paediatric dermatology clinic, but also that the score is safe and identifies accurately those patients who need specialist interventions.
Conclusion
IH are common and usually uncomplicated. They generally follow a predictable clinical course and do not usually require intervention. Rarely, complications such as ulceration, airway obstruction, liver haemangiomas, or structural and cosmetic issues can arise. In these circumstances treatment is required. Propranolol is the first-line treatment and is initiated by dermatologists or paediatricians with a special interest in the subject. In the community, when deciding which patients should or should not be referred to specialist centres for consideration of propranolol, the IHReS is a useful tool. It is a quick and easy scoring system that is validated and safe. Further information about IH as well as patient information leaflets can be found at the British Association of Dermatologists website – www.bad.org.uk.











Leave a Reply
You must be logged in to post a comment.