NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
In November 2022, the Global Initiative for Chronic Lung disease (GOLD) released their updated guidelines with some significant changes. This article reviews these changes and how they impact on the initial and ongoing pharmacological management of chronic obstructive pulmonary disease (COPD).
The definition of COPD has been revised – “COPD is a heterogenous lung condition characterised by respiratory symptoms (dyspnoea, cough, sputum production) due to abnormalities of the airways (bronchitis, bronchiolitis) and alveoli (emphysema) that cause persistent and often progressive airflow obstruction.”¹
In 2016, Ireland was noted as having the highest hospitalisation rates per 100,000 head of population in the OECD in relation to COPD. It is estimated that 380,000 people are living with COPD in Ireland and yet only 110,000 are diagnosed. It is more prevalent in the more vulnerable in society, including people from areas with high social deprivation.²
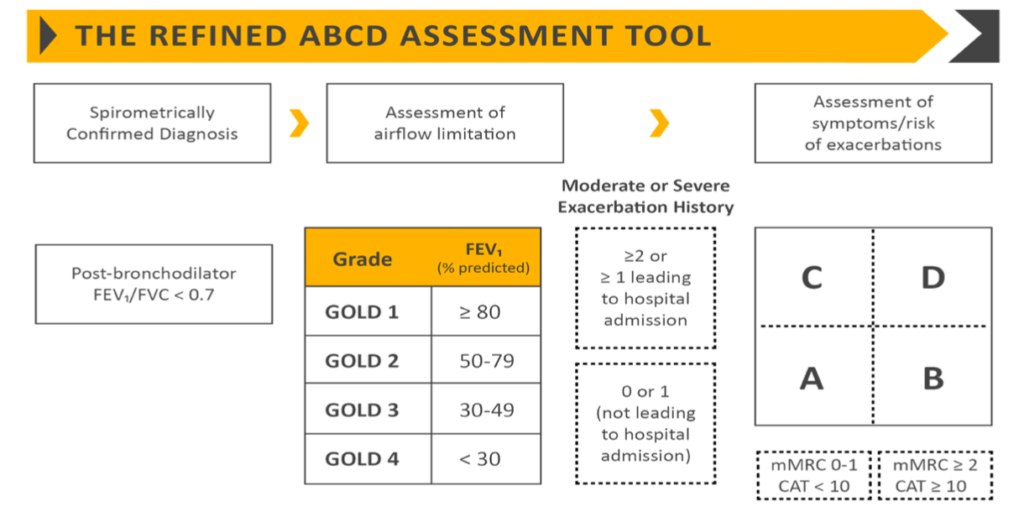
Figure 1: The original refined GOLD ABCD Assessment Tool (2017)
The GOLD Refined Assessment Tool, first introduced in 2017, included spirometric assessment of airflow obstruction and grouping of patients based on symptoms (primarily breathlessness) and recent history of exacerbations (as an indicator of future exacerbation risk). The original model stratified patients into four groups (A, B, C, and D) based on high or low exacerbation risk and high or low symptoms using the COPD Assessment Test (CAT score) and/or Medical Research Council Score (MRC) (Figure 1). Initial pharmacological treatment was based on these groupings. The recommendation for patients with a low exacerbation risk and a low symptom burden (CAT <10) (Group A) was a short-acting bronchodilator. For those with a high symptom burden (CAT >10) and a low exacerbation risk (Group B) was a long-acting bronchodilator (LABA) or long-acting muscarinic agent (LAMA). For patients with a high exacerbation risk and a low symptom burden (Group C), a LAMA was recommended. For those with a high symptom burden and a high risk of exacerbation (Group D), combination therapy (LAMA + LABA or LABA + inhaled corticosteroid [ICS]) was recommended. While the assessment of severity based on spirometric evaluation remains, the grouping of patients by symptom burden and future exacerbation risk has changed in the 2023 update (Figure 2), along with the recommended initial pharmacotherapy for each group (Figure 3).¹
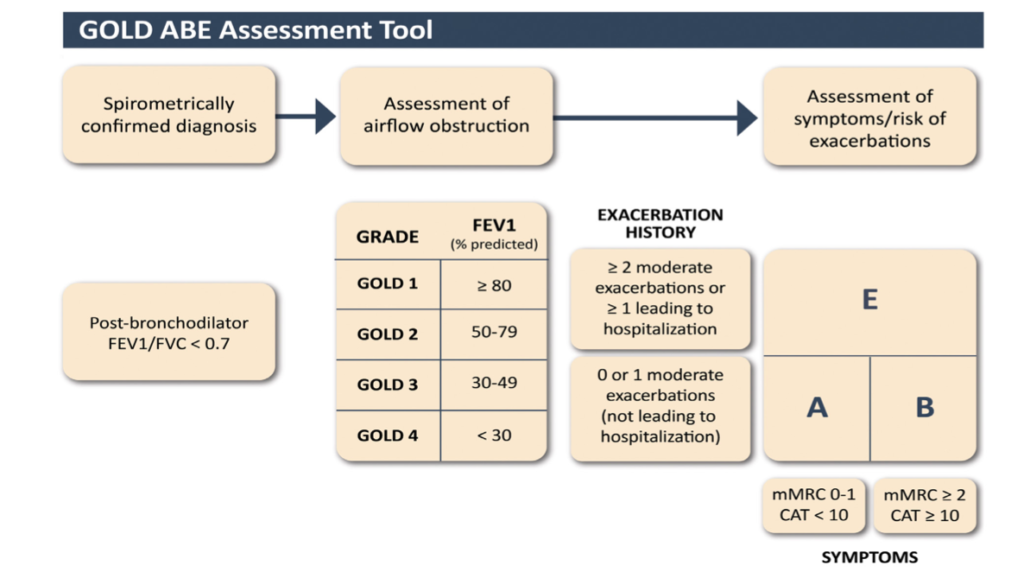
Figure 2: The updated GOLD ABE Assessment Tool
Management of patients with a low risk of future exacerbations
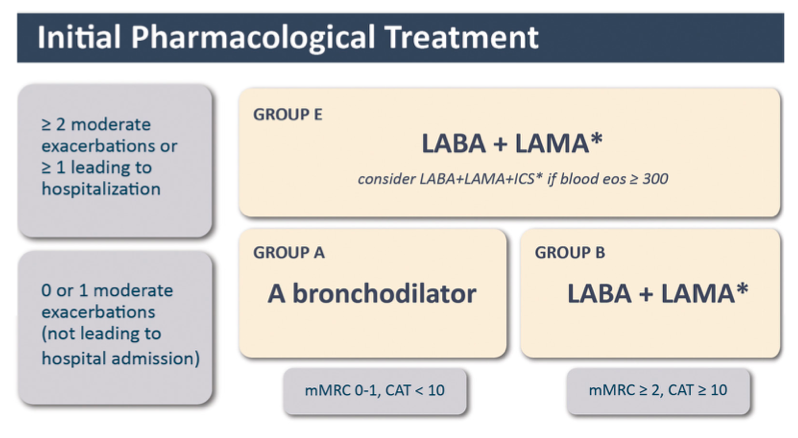
The treatment for patients with a low risk of exacerbation and low symptom burden (Group A) remains the same (Figure 3). The 2023 report is very clear that there is no longer a role for the LABA + ICS combination for the initial treatment of patients with COPD at low risk for exacerbations.1,3
Management of patients with a high risk of future exacerbations
Perhaps the most significant change is that patients at high risk for exacerbations are no longer stratified by symptom burden. Instead, these patients are grouped together as Group E, with initial treatment being a LABA + LAMA combination (Figure 3). For these patients, a more rational approach to ICS use is recommended, guided by clinical factors and blood eosinophil levels. Patients that are unlikely to benefit from an ICS are those with a blood eosinophil count of 300 cells/µL, a history of hospitalisation for COPD exacerbations with ≥2 moderate exacerbations a year or with a history of, or concomitant asthma. When considering starting an ICS, blood eosinophils are not the only useful factor. There are known harms of ICS use, including an increased risk of pneumonia and of mycobacterial infection.³ Patients with a history of recurrent pneumonia and those with a previous mycobacterial infection should not routinely be started on ICS as the harms may well outweigh the benefits. These fundamental changes to the classification and initial treatment of patients with a high risk of future exacerbations reflect the findings of the ECLIPSE study. This study demonstrated that an eosinophil count, an indicator of underlying inflammation, was a better predictor of response to ICS therapy than was a high symptom burden.⁴
Management of patients with ongoing symptoms or exacerbations
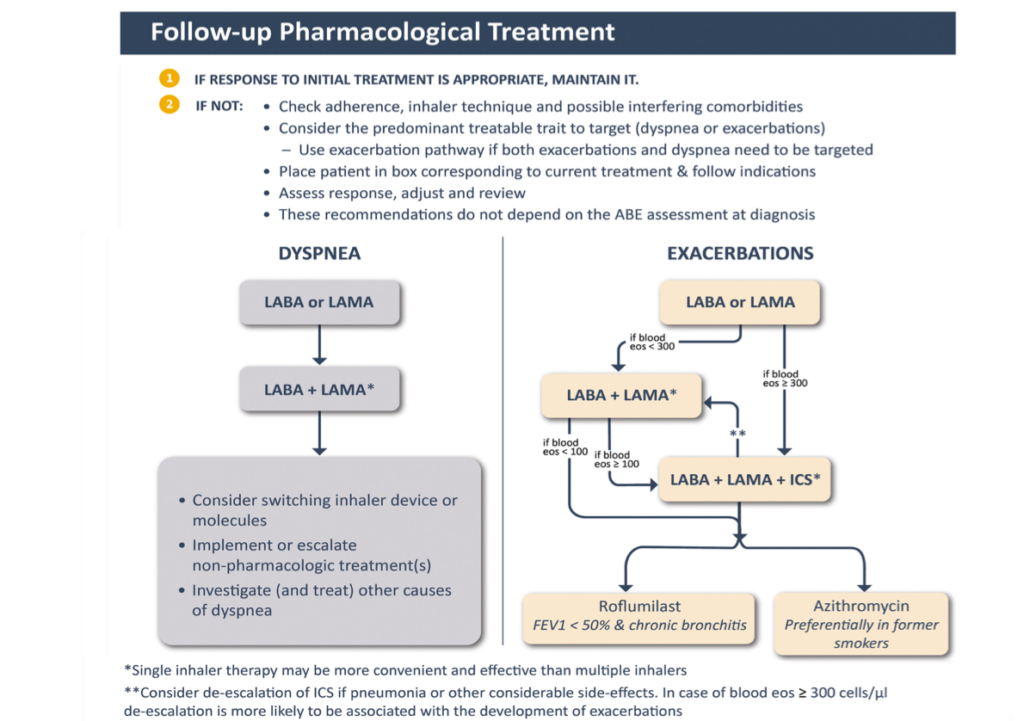
The rational approach to the use of ICS therapy based on evidence of an underlying inflammatory process greatly simplifies both the approach to initial treatment and the follow-up treatment decisions (Figure 3).¹ The first step for any patient with ongoing symptoms or repeated exacerbations is to review and optimise their current treatment regimen – check inhaler technique, check adherence to treatment, and consider whether any comorbid conditions are present or require review. Next steps depend on whether the patient has ongoing breathlessness or repeated exacerbations (treatable traits), regardless of their initial grouping (Figure 4). Patients with ongoing breathlessness who were receiving bronchodilator monotherapy can be escalated to combination LABA + LAMA therapy.¹ For those already on combination therapy, switching to an alternative device or molecule can be considered alongside a focus on treatment optimisation, ie, adherence and inhaler technique. Non-pharmacological management such as pulmonary rehabilitation, and investigation of alternative causes of breathlessness should also be explored. Patients with ongoing exacerbations can be escalated to triple therapy including an ICS if eosinophils are elevated >300 cells/µL if not contraindicated. Triple therapy with the addition of ICS can subsequently be offered for patients who experience a severe exacerbation (requiring hospitalisation) or who experience two moderate exacerbations within a year. If it is not clear which treatable trait (dyspnoea or exacerbations), is most predominate, it is recommended to follow the pathway for exacerbations.
Management of patients without features of asthma
Patients with breathlessness as their major clinical feature and who do not have features of asthma will not benefit from ICS therapy and their treatment should focus on bronchodilation, SABA, LABA or LABA + LAMA depending on the impact of their breathlessness on their daily activities. Patients who are exacerbating can start on a SABA in addition to single agent bronchodilation with a LAMA or LABA. If breathlessness is still impacting on their activities of daily living, then dual long-acting bronchodilator therapy (LABA + LAMA) can be commenced. ICS (triple therapy) can be used in addition to dual bronchodilation if they continue to experience exacerbations. At each stage, medication optimisation should be undertaken, including checking the patient’s inhaler technique and their adherence to therapy. In addition, ongoing monitoring of patients should include reviewing for comorbidities (especially alternative causes of breathlessness) and whether pulmonary rehabilitation has been offered and attended, as well as treating tobacco dependency and offering appropriate vaccinations.
As we have seen from the ECLIPSE study,³ ongoing breathlessness is not a good indicator for response to ICS therapy and it was for this reason that the 2023 GOLD update elected to require elevated eosinophils as a marker of underlying inflammation as a pre-requisite for initiation of ICS therapy. Using triple therapy as an option for patients with ongoing breathlessness is concerning as it is unlikely to prove much benefit in relieving their breathlessness and may cause a delay in seeking alternative causes for their chronic breathlessness. This approach will mean that a proportion of patients will be escalated to triple therapy and receive an ICS which they will gain no clinical benefit from, and which may place them at increased risk for pneumonia.
Patients with an asthma component are likely to benefit from ICS and this should form a part of their initial treatment regimen.
Vaccinations
In addition to influenza, pneumococcal and Covid-19 vaccines, the US CDC recommends the Tdap vaccine (pertussis, tetanus, and diphtheria) for COPD patients who were not vaccinated in adolescence, as well as routine use of shingles vaccine in all COPD patients over 50 years.⁵
COPD exacerbations
The definition of COPD exacerbations has been revised to: “An exacerbation of COPD is defined as an event characterised by dyspnoea and/or cough and sputum that worsen over <14 days. Exacerbations of COPD are often associated with increased local and systemic inflammation caused by airway infection, pollution, or other insults to the lungs.”¹
Currently, exacerbations are classified after the event has occurred as:
Mild (treated with short-acting bronchodilators only, SABDs);
Moderate (treated with SABDs and oral corticosteroids ± antibiotics); or
Severe (patient requires hospitalisation or visits the emergency room). Severe exacerbations may also be associated with acute respiratory failure.¹
GOLD 2023 proposes the following changes based on a clinical approach based on the current best available evidence:¹
1. Complete a thorough clinical assessment for evidence of COPD and potential respiratory and non-respiratory concomitant diseases, including consideration of alternative causes for the patient’s symptoms and signs: Primarily pneumonia, heart failure, and pulmonary embolism.
2. Assess:
u Symptoms, severity of dyspnoea that can be determined by using a VAS, and documentation of the presence of cough.
u Signs (tachypnoea, tachycardia), sputum volume and colour, and respiratory distress (accessory muscle use).
3. Evaluate severity by using appropriate additional investigation such as pulse oximetry, laboratory assessment, CRP, arterial blood gases.
4. Establish the cause of the event (viral, bacterial, environment, etc).
Conclusions
Steroid stewardship, both OCS and ICS, remains relevant to avoid exposing patients to treatments that they will not benefit from, and which may in fact place them at risk for side-effects. Managing patients according to their treatable traits is one of the most significant changes to the GOLD 2023 guidelines. This allows healthcare professionals to provide a more holistic approach to COPD management as it recognises the trait which is most problematic for the patient and allows treatment to be individualised and more targeted. While a cure for COPD remains elusive and treatment is largely reactive to clinical presentation, there is much we can do to ensure patients receive treatments that relieve their most impactful daily symptoms, optimise their lung function, and reduce their risk for life-threatening exacerbations.
References
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report. Available at: https://goldcopd.org/2023-gold-report-2/. Accessed February 2023
HSE National Clinical Programme for COPD. About COPD. Available at: www.hse.ie/eng/about/who/cspd/ncps/copd/about/. Accessed February 2023
Banerji D, Mahler DA, Hanania NA. Efficacy and safety of LABA/LAMA fixed dose combinations approved in the US for the management of COPD. Expert Rev Respir Med 2016;10:767–80
Faner R, Tal-Singer R, Riley JH, et al. Lessons from ECLIPSE: A review of COPD biomarkers. Thorax 2014;69:666–72
Centers for Disease Control and Prevention. Post-Covid Conditions: Information for Healthcare Providers. 2022. Available at: www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html











Leave a Reply
You must be logged in to post a comment.