NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
A detailed overview of the presentation and management of gestational diabetes
Gestational diabetes mellitus (GDM) is a common pregnancy-related metabolic disorder characterised by glucose intolerance. It can occur at any stage of pregnancy, but is more common in the second and third trimesters. GDM poses risks to both the mother and foetus, necessitating early detection and effective management. Pregnant women with GDM are at risk of developing gestational hypertension, pre-eclampsia, premature birth, and delivery by Caesarean section. While GDM usually resolves following delivery, it can increase the risk of other complications, including cardiovascular disease, obesity, and impaired carbohydrate metabolism, leading to the development of type 2 diabetes (T2DM) in both the mother and infant.1
Risk factors include being overweight/obese, having polycystic ovary syndrome, long-term steroid use, advanced maternal age (40 years and over), glycosuria, previously given birth to a baby weighing 4.5kg or more, unexplained previous stillbirth, ethnicity, genetic polymorphisms, and a family history of insulin resistance and/or diabetes.9,10
The prevalence of GDM has been rising globally, mirroring increasing rates of obesity and diabetes. GDM affects approximately 14 per cent of pregnancies worldwide, accounting for an estimated 18 million births annually.3 Experts expect that this growing public health concern will increase in response to more people with hyperglycaemia, diabetes, obesity, advanced maternal age, and sedentary lifestyles.13 Recent advancements in research and clinical practice have enhanced understanding of GDM’s pathophysiology, diagnostic criteria, and management strategies.
Pathophysiology
GDM is a complex interplay of hormonal changes, insulin resistance, impaired insulin secretion, adipokine dysregulation, placental factors, oxidative stress, lipid metabolism disturbances, genetic predisposition, and epigenetic modifications.4
Hormonal changes: During pregnancy, the placenta produces hormones essential for foetal development, including human placental lactogen (hPL) and progesterone. While these hormones are vital, they can also induce insulin resistance in maternal tissues. Insulin resistance causes cells to become less responsive to the effects of insulin, leading to reduced glucose uptake and elevated blood glucose levels. This adaptive response ensures an adequate supply of glucose to the developing foetus, but it can contribute to the onset of GDM in susceptible women.4,5
Impaired insulin secretion: GDM is not solely characterised by insulin resistance; impaired insulin secretion from pancreatic beta cells also plays a role. The increased demand for insulin due to the hormonal changes of pregnancy can overwhelm the capacity of beta cells to secrete sufficient insulin. This results in a relative insulin deficiency, exacerbating the elevation of blood glucose levels. Genetic factors influencing beta cell function and insulin secretion contribute to the variability in GDM susceptibility among pregnant women.4
Adipokines and inflammatory factors: Adipokines play a role in glucose and lipid metabolism and can influence insulin sensitivity. In GDM, alterations in the profile of adipokines such as adiponectin and leptin have been observed. Additionally, increased levels of inflammatory markers, like C-reactive protein and tumour necrosis factor-alpha, have been associated with insulin resistance and impaired glucose tolerance.4,7
Placental factors: The placenta produces hormones that impact maternal glucose metabolism such as hPL and cortisol. These hormones antagonise the action of insulin, contributing to insulin resistance. The placenta also releases molecules called placental-derived factors that can interfere with insulin signalling pathways and exacerbate insulin resistance.4,8
Oxidative stress and lipid metabolism: Oxidative stress, characterised by an imbalance between reactive oxygen species production and antioxidant defences, has been implicated in GDM pathophysiology. Elevated levels of reactive oxygen species can impair insulin signalling pathways and contribute to insulin resistance. Disturbances in lipid metabolism, including increased levels of free fatty acids, can further exacerbate insulin resistance and impair glucose uptake by skeletal muscle and adipose tissue.4
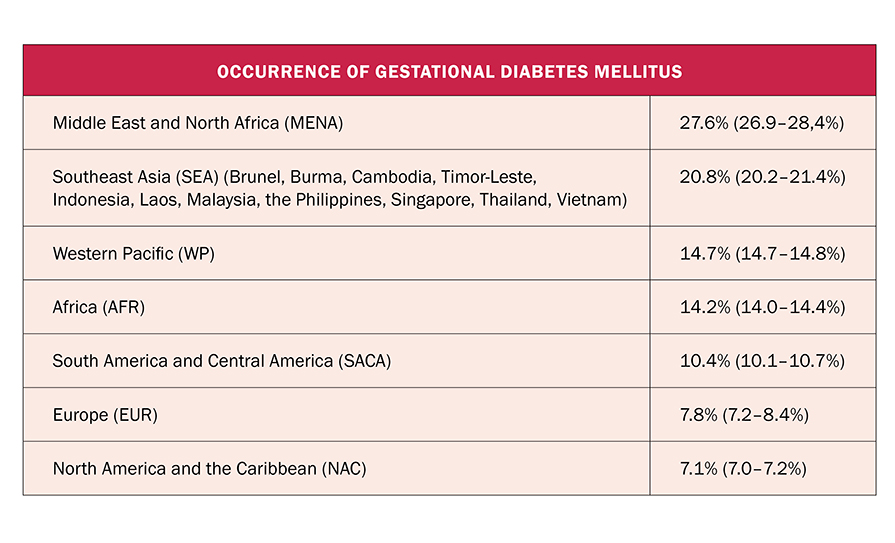
TABLE 1: Geographical distribution of GDM2
Genetic predisposition and epigenetic modifications: Genetic factors play a significant role in determining an individual’s susceptibility to GDM. Polymorphisms in genes involved in insulin signalling, beta cell function, and glucose metabolism can increase the risk of developing GDM. Changes in gene expression patterns without alterations to the underlying DNA sequence can influence GDM risk by modulating the expression of genes involved in insulin sensitivity and glucose metabolism.4,6
Reducing risk of development
The risk of developing GDM can be reduced by eating healthily, increasing moderate activity, and maintaining a healthy weight.9,10
Clinical presentation
GDM is often asymptomatic in nature. Understanding the potential signs and risk factors is important for early detection, timely diagnosis, and management. Unlike type 1 or T2DM, which can present with noticeable symptoms such as excessive thirst, frequent urination, and unexplained weight loss, GDM may not manifest obvious signs in the early stages. This highlights the significance of routine screening in pregnant women to ensure early detection and timely intervention. Women should be assessed for risk factors of GDM during their first antenatal appointment at around week eight-to-12 of pregnancy. Routine screening for GDM is usually carried out between week 24-to-28 of pregnancy. 9,10,15
Hyperglycaemia in pregnancy is associated with adverse maternal and prenatal outcomes. Symptoms of hyperglycaemia can include increased thirst, frequency of micturition, dry mouth, tiredness, blurred vision, genital itching, and candida. However, some of these symptoms are also common during pregnancy and are not necessarily a sign of GDM. Some women may experience subtle indications that warrant further investigation. These can include excessive hunger, excessive weight gain, recurrent infections, fatigue, lethargy, and polyhydramnios, resulting in larger-than-normal uterine size.9,10
Diagnosis
Diagnostic criteria for GDM primarily rely on glucose tolerance tests, with the oral glucose tolerance test (OGTT) being the gold standard. The standard 75g OGTT involves fasting blood glucose measurement followed by post-glucose load readings at one and two hours. If GDM is suspected at an earlier or later gestation than 24-to-28 weeks based on foetal macrosomia, polyhydramnios, or glycosuria, a 75g OGTT should be performed. If negative at an early gestation, the OGTT should be repeated between 24-to-28 weeks gestation.14,15
The potential of using haemoglobin A1c (HbA1c) as a diagnostic tool for GDM has been explored. HbA1c reflects average blood glucose levels over several weeks and is widely used in diagnosing diabetes. However, its utility in GDM diagnosis remains debated, as pregnancy-related changes in haemoglobin levels and potential variations in its accuracy during gestation can affect its reliability as a standalone diagnostic tool.12
Treatment
Pregnancy complicated by GDM is considered high risk; therefore, frequent hospital-based antenatal visits/remote monitoring are required. Women with diabetes in pregnancy should be cared for by a multidisciplinary team consisting of a consultant endocrinologist or a physician with an interest and experience in diabetes and pregnancy, a consultant obstetrician with experience in the management of diabetes in pregnancy, a dietician, and a diabetes midwife/nurse specialist. GDM may be the initial warning signs of intrinsic insulin resistance and beta cell dysfunction, and provides an opportunity for screening and possible prevention of diabetes and its long-term complications. Blood pressure, body weight, and urinalysis should be measured at each visit as the risk of hypertensive disorders increases when pregnancy is complicated by diabetes. If not already commenced, folic acid 5mg daily should be initiated and any teratogenic medication discontinued, where the specialist team, in consultation with the woman, deem it appropriate to do so.14
GDM can often be controlled with diet and exercise. The patient should be educated regarding diet, lifestyle modification, and diabetes management. Women should be encouraged, supported, and provided with appropriate information to make positive lifestyle changes such as cessation of smoking and alcohol consumption.
Treatment for GDM usually thus begins with non-pharmacologic management such as diet modifications, exercise, and glucose monitoring. Self-monitoring of blood glucose is suggested for all women with GDM. This includes women who are managed with diet alone, as well as those using diet and insulin therapy. For women receiving insulin therapy, self-monitoring of blood glucose should be performed seven times a day – pre meals, plus one hour post all meals, plus once before bed.
Making healthy food choices, including a wide variety of foods and correct portion sizes, is important.10,14,15 Monitoring carbohydrate intake remains the key strategy in achieving glycaemic control. A diet that includes carbohydrates from fruit, vegetables, wholegrains, legumes, and low-fat milk is encouraged for good health. Calorie intake and weight gain must be carefully monitored in patients with GDM. Working with a registered dietician, the patient can develop a dietary plan that incorporates their BMI. Just as no one-size diabetic diet exists, no set optimal calorie goal for those with GDM exists. Dietary plans should be adjusted based on blood glucose results, weight gain, appetite, dietary preferences, and activity level. Dietary goals should provide adequate calorie intake, promote maternal and foetal health, support appropriate weight gain, and ensure glycaemic targets are met. Dietary advice should be culturally appropriate.13
Physical activity has beneficial effects on insulin resistance, and regular physical activity is regarded as potentially advantageous to most people with diabetes. Exercising regularly helps keep glucose levels within normal targets to manage GDM. The amount of exercise recommended is 30 minutes of moderate-intensity aerobic exercise at least five days a week or a minimum of 150 minutes per week. Walking is a good exercise for pregnant women. Any pre-existing cardiovascular or musculoskeletal conditions should be evaluated before the patient engages in physical activity. Patients with pelvic joint laxity, short cervix conditions, or those at risk for premature delivery should seek advice from their medical provider and proceed with caution.10,13
Blood glucose should be maintained between 4-7mmol/L.14 One-to-two women in every 10 with GDM will require medication to control their blood glucose levels. If the patient’s glycaemic control is not adequate despite optimal adherence to diet and exercise, pharmacologic treatment is recommended. Insulin injections are the usual medication during pregnancy to help women control their blood glucose, as human insulin formulations do not cross the placenta. A clinical decision regarding insulin therapy should be based on gestational age, foetal size, and glycaemic control. Insulin given four times daily has been proven to improve glycaemic control and pregnancy outcomes. The flexibility of a basal bolus regime allows for easier adjustment of insulin doses. The most common complication associated with insulin therapy is hypoglycaemia, and patients prescribed insulin should be taught the signs and symptoms of hypoglycaemia and how to treat it. The glucagon injection should be prescribed, and its use explained to the woman and her family.14 Oral medication such as metformin can also be used to treat GDM.10-13
Monitoring of the foetus is an important part of managing GDM, and regular scans to monitor the baby’s growth are carried out. Monitoring can include ultrasound and doppler measurements to check the baby’s growth and health, and cardiotocography (CTG) to measure the baby’s heart rate. As pregnancy progresses, women should be advised to monitor foetal movement and report any concerns immediately to the healthcare team.10 For women diagnosed with GDM in the first trimester, undiagnosed pre-existing diabetes should be considered, and foetal surveillance should include a second trimester ultrasound to detect foetal anomalies, and third trimester ultrasounds to assess foetal wellbeing and growth.14
Delivery
Most women with controlled GDM can complete a full-term pregnancy and have a normal birth with no complications. However, delivery should take place in a hospital with full obstetric, anaesthetic, and neonatal intensive care facilities, and with an experienced paediatrician available for delivery. Continuous foetal monitoring throughout labour and delivery is advised. In GDM, delivery before 41 weeks is advisable. Induction of labour or a Caesarean section is recommended if labour does not start naturally by this time. Earlier delivery may be recommended if there are concerns about the mother or baby’s health, or if blood sugar levels have not been well controlled.9
If there is a risk of preterm labour between 24-to-34 weeks gestation, a course of antenatal corticosteroids should be administered to accelerate foetal lung maturity. Antenatal steroids adversely affect maternal glycaemic control, and this should be anticipated. Intensive insulin therapy and frequent glucose monitoring are required to prevent hyperglycaemia. Hospitalisation is necessary for metabolic supervision during steroid administration. In the presence of obstetric or diabetes complications, elective delivery should be considered at 38 weeks gestation. An elective Caesarean section is best performed at 39 rather than 38 weeks gestation in the absence of obstetric or diabetes complications to reduce neonatal respiratory morbidity. Following delivery, insulin requirements decline rapidly and prevention of maternal hypoglycaemia is important.14
Where feasible, mothers with diabetes should be offered an opportunity for skin-to-skin contact with their babies immediately after delivery. Breastfeeding within one hour of birth should also be encouraged. Routine blood glucose measurement in the well baby at term during the first two-to-three hours after birth should be avoided, however, where there is clinical concern, blood sampling should be performed. Screening for hypoglycaemia should generally be performed prior to the second feed (approximately four-to-six hours) in the well baby at term.14
Health education, health promotion, and follow-up discussions should take place at the six-week postnatal appointment if not already discussed in the immediate postpartum period. Women with a diagnosis of GDM have a 35-to-50 per cent chance of recurrence in future pregnancies, and this should be discussed in the postnatal period. Postnatal education should also incorporate advice on diet, physical activity, weight reduction/healthy weight maintenance, and other lifestyle interventions such as smoking cessation if applicable. The increased risk of developing T2DM in the future should be emphasised. Women with identified post-natal glucose intolerance or confirmed diabetes should be advised to seek pre-conceptual counselling for any future pregnancies, and methods of contraception agreeable with the woman and her partner should be discussed and prescribed as appropriate.14,15
Outlook
The prognosis for GDM is evolving in response to advancements in research, technology, and clinical practice. With a focus on personalised medicine, intergenerational health, and preventive strategies, the future holds the promise of improved outcomes for both mothers and their offspring.16 Advancements in precision medicine are likely to influence the prognosis for GDM. Personalised risk assessment based on genetic markers, metabolic profiles, and other factors can enable tailored interventions. This may include early identification of high-risk individuals, individualised dietary and exercise recommendations, and targeted pharmacological interventions.
The future also holds promise for more sensitive and specific diagnostic tools for GDM. Biomarkers and advanced glucose monitoring technologies could enable earlier detection, allowing for timely interventions to prevent maternal and foetal complications. Strategies that focus on preventing GDM through lifestyle modifications and optimising maternal health prior to conception could further enhance outcomes.16
Telemedicine and remote monitoring technologies are likely to play a significant role in the future prognosis of GDM. Continuous glucose monitoring devices and smartphone applications can facilitate real-time data collection, enhancing patient engagement and healthcare provider collaboration. Telemedicine platforms can enable remote consultations, providing convenient access to healthcare services, especially for women in remote areas.16
While the outlook for GDM is promising, several challenges require attention. Standardising diagnostic criteria, establishing clear guidelines for postpartum monitoring, and addressing disparities in access to care are essential. Additionally, ensuring that interventions are culturally sensitive, accessible, and acceptable to diverse populations is important for equitable outcomes.
References
Modzelewski R, Stefanowicz-Rutkowska M, Matuszewski W, Bandurska-Stankiewicz E. Gestational diabetes mellitus – recent literature. Review. J Clin Med. 2022;11(19):5736
Wang H, Li N, Chivese T, et al. IDF Diabetes Atlas: Estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res Clin Pract. 2022;183:109050
International Diabetes Federation. IDF Diabetes Atlas. 8th ed IDF. Belgium. 2017
Plows J, Stanley J, Baker P, Reynolds C, Vickers M. The pathophysiology of gestational diabetes mellitus. Int J Mol Sci. 2018;19(11):3342
Skajaa G, Fuglsang J, Knorr S, et al. Changes in insulin sensitivity and insulin secretion during pregnancy and post-partum in women with gestational diabetes. BMJ Open Diabetes Res Care. 2020;8(2):e001728
Lowe W. Genetics and epigenetics: Implications for the life course of gestational diabetes. Int J Mol Sci. 2023;(24):6047
Gutaj P, Sibiak R, Jankowski M, Awdi, et al. The role of the adipokines in the most common gestational complications. Int J Mol Sci. 2020;21:9408
Olmos-Ortiz A, Flores-Espinosa P, Díaz L, et al. Immunoendocrine dysregulation during gestational diabetes mellitus: The central role of the placenta. Int J Mol Sci. 2021;22(15):8087
National Health Service. Gestational diabetes. National Health Service, UK. 2020. Available at: www.nhs.uk/conditions/gestational-diabetes/
Health Service Executive. Why diabetes develops in pregnancy: Gestational diabetes. 2023. Available at: www2.hse.ie/conditions/gestational-diabetes/
Quintanilla Rodriguez B, Mahdy H. Gestational diabetes. StatPearls Publishing. 2022. Available at: www.ncbi.nlm.nih.gov/books/NBK545196/
Arbiol-Roca E, Pérez-Hernández N, Aisa-Abdellaoui T, et al. The utility HBA1c test as a screening biomarker for detecting gestational diabetes mellitus. Clinical Biochemistry. 2021;90:58-61.
Brady V, Goering L. Gestational diabetes. American Nurse. 2022. Available at: www.myamericannurse.com/gestational-diabetes/
Health Service Executive. Guidelines for the management of pre-gestational and gestational diabetes mellitus from pre-conception to the postnatal period. 2010. Available at: www.hse.ie/eng/services/list/2/primarycare/east-coast-diabetes-service/management-of-type-2-diabetes/diabetes-and-pregnancy/guidelines-for-the-management-of-pre-gestational-and-gestational-diabetes-mellitus-from-pre-conception-to-the-postnatal-period.pdf
Irish College of General Practitioners. GP desktop guidelines for the management of pre-gestational and gestational diabetes mellitus from pre-conception to the postnatal period (Revised 2015). Adapted from: A practical guide to integrated type 1 diabetes care. 2015. Available at: www.icgp.ie
Chu L, Sugiyama T, Ma R. Recent updates and future perspectives on gestational diabetes mellitus: An important public health challenge. J Diabetes Investig. 2021;12(11):1944-1947
Theresa Lowry-Lehnen: RGN, PG Dip Coronary Care, RNP, BSc, MSc, PG Dip Ed (QTS), M Ed, PhD, Clinical Nurse Specialist and Associate Lecturer, South East Technological University












Leave a Reply
You must be logged in to post a comment.