NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
There are an estimated 50,000 people in Ireland living with Coeliac disease, which leads to chronic ill health and complications if untreated.
Coeliac disease is an autoimmune disorder triggered by gluten ingestion in genetically-predisposed individuals, resulting in mucosal inflammation and villous atrophy in the small intestine leading to malabsorption. It is a chronic disease and is not an allergy or food intolerance. Coeliac disease is one of the most common autoimmune conditions, with a prevalence of 0.5-to-1 per cent of the general population, with a female-to-male ratio ranging from 2:1 to 3:1.1,2 Prevalence estimates based on serologic screens indicate the disorder may be present in 1/150 in Europe, and 1/250 in some parts of the US. Current prevalence estimates in some regions including Ireland are as high as 1/100.4 There are an estimated 50,000 people in Ireland living with Coeliac disease, and a further 400,000 who are gluten intolerant. Many cases of Coeliac disease go undiagnosed.5,13
Onset of Coeliac disease can occur at any age, although symptoms are most likely to develop in early childhood after weaning with gluten, and the introduction of cereals into the diet in the first year of life. Coeliac disease can also occur in later adulthood, and is often diagnosed in people aged 40-to-60 years. Coeliac disease is higher in first-degree Coeliac disease relatives (10-to-20 per cent) and in other at-risk groups, particularly patients with Down syndrome, type 1 diabetes, or IgA deficiency.1,2 The condition is more common in people with type 1 diabetes and autoimmune thyroid disease. Between 4 and 9 per cent of people with type 1 diabetes also have Coeliac disease, compared with 1 per cent in the general population. People with autoimmune thyroid disease are at a higher risk (1-to-4 per cent) of having Coeliac disease compared with 1 per cent in the general population.12 Coeliac disease is a chronic condition, and currently, the only treatment consists of permanent exclusion of gluten from the diet.3
Aetiology and pathophysiology
Coeliac disease is a hereditary disorder caused by sensitivity to the gliadin fraction of gluten, a protein found in wheat. Similar proteins are present in rye and barley. In a genetically susceptible person, gluten-sensitive T-cells are activated when gluten-derived peptide epitopes are presented. The inflammatory response causes characteristic mucosal villous atrophy in the small intestine. This destruction, in turn, leads to the decreased functionality of the intestinal surface and malabsorption. The lack of nutrient absorption impacts directly on the digestive system, but also indirectly on all the systems of the body. This results in generally poor health, and is why Coeliac disease can have signs and symptoms arising from almost any body system, and not just the gastrointestinal system.4
Presentation
Coeliac disease is more commonly detected in infants and children younger than three years of age, and is characterised by diarrhoea, anorexia, pallor, abdominal distention, muscle wasting, and failure to thrive. Stools are often soft, bulky, clay-coloured, and offensive. Older children may present with anaemia, weight loss or failure to grow normally. Adults may present with diarrhoea, bloating, constipation and abdominal pain.3 Lassitude, weakness, and anorexia are common. Mild and intermittent diarrhoea is sometimes the presenting symptom and steatorrhoea ranging from mild to severe. Some patients have weight loss, although rarely enough to become underweight. Anaemia, glossitis, angular stomatitis, and aphthous ulcers are often seen in these patients. Manifestations of vitamin D and calcium deficiencies such as osteomalacia, osteopaenia, and osteoporosis are common. Both males and females may have reduced fertility and women may have amonorrhoea.3,4
About 10 per cent of patients with Coeliac disease develop dermatitis herpetiformis (DH), a skin condition caused by gluten intolerance. Dermatitis herpetiformis is an intensely pruritic papulovesicular rash that is distributed symmetrically over the extensor areas of the elbows, knees, buttocks, shoulders, and scalp. It usually responds to the exclusion of gluten from the diet, but can take a long time for a gluten-free diet to clear the rash. For individuals with dermatitis herpetiformis, a skin biopsy is usually sufficient for diagnosis of both DH and Coeliac disease. It is not necessary to perform an endoscopic biopsy, as the skin biopsy is definitive.14 Dapsone, a sulfone, is an oral antibacterial medication prescribed for DH, which is taken twice daily. Dapsone can cause side-effects such as headache and depression and may need to be prescribed for up to two years. The lowest effective dose should be prescribed.3,4,13
Untreated Coeliac disease leads to chronic ill health and complications. Complications which may or may not be present at diagnosis include osteoporosis, ulcerative jejunitis, malignancy-intestinal lymphoma, functional hyposplenism, vitamin D deficiency, and iron deficiency.11
Serological testing for Coeliac disease should be offered to people with persistent unexplained abdominal or gastrointestinal symptoms; faltering growth; prolonged fatigue; unexpected weight loss; severe or persistent mouth ulcers; unexplained iron, vitamin B12 or folate deficiency; type 1 diabetes at diagnosis; autoimmune thyroid disease at diagnosis; irritable bowel syndrome in adults; and first-degree relatives of people with Coeliac disease.11
Diagnosis
A diagnosis of Coeliac disease is suspected clinically, based on history and laboratory abnormalities suggestive of malabsorption. Family incidence is an indicator and Coeliac disease should also be strongly considered in patients with iron deficiency without obvious gastrointestinal bleeding. A confirmed diagnosis depends on serologic markers and a small-bowel biopsy. Anti-tissue transglutaminase antibody (tTG) and anti-endomysial antibody (EMA) have sensitivity and specificity 90 per cent. These antibodies decrease in titre in patients on a gluten-free diet and are useful in monitoring dietary adherence.4 Diagnostic serologic testing is done with patients following a gluten-containing diet. To obtain a reliable result the patient must have been consuming gluten for more than one meal a day for six weeks. It is important to advise the patient not to start a gluten-free diet until diagnosis is confirmed by a specialist, even if the results of a serological test are positive.11
Coeliac disease is strongly associated with variations of the human leukocyte antigen (HLA) DQ gene. Research has shown that the HLA DQ2 and HLA DQ8 variants are almost always present in people with Coeliac disease of white, Northern European background. Although less clear, these variants probably play a similar role in other ethnic groups. Testing for the HLA DQ2 and HLA DQ8 variants alone cannot be used to diagnose Coeliac disease, as these genes are present in a large proportion of the population, including people who do not have coeliac disease. In the UK, NICE recommends to only consider using HLA DQ2 (DQ2.2 and DQ2.5) and HLA DQ8 testing in diagnosis of Coeliac disease in specialist settings; eg, children who are not having a biopsy or people who have already limited gluten from the diet and choose not to have a gluten challenge.6,11
Serological tests to investigate suspected Coeliac disease in young people and adults should test for total immunoglobulin A (IgA) and IgA tissue transglutaminase (tTG) as the first choice; IgA endomysial antibodies (EMA) if IgA tTG is weakly positive and consider using IgG EMA, IgG deamidated gliadin peptide (DGP) or IgG tTG if IgA is deficient. Serological tests to investigate suspected Coeliac disease in children should test for total IgA and IgA tTG as the first choice, and consider using IgG EMA, IgG DGP or IgG tTG if IgA is deficient.11
If either serological test is negative, Coeliac disease is unlikely. However, it is possible to have a negative test and still have Coeliac disease; for example, patients already on a gluten-free diet and therefore the antibodies are negative. A minority of Coeliac patients may have IgA deficiency and the screening test results can be misleading so, the total serum IgA should be checked to detect IgA deficiency.3,8
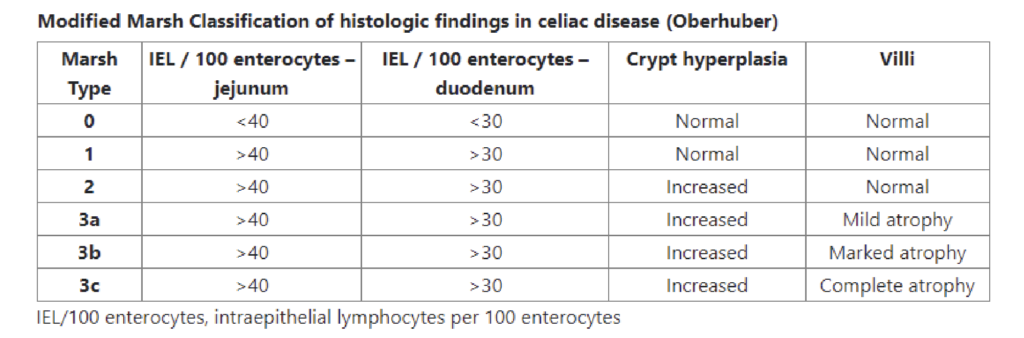
Table 1: Classification of histologic findings in celiac disease. Available at: https://celiac.org/about-celiac-disease/screening -and-diagnosis/diagnosis/
If either serological test is positive, the patient should have a diagnostic small-bowel biopsy. The gold standard for the diagnosis of Coeliac disease is a duodenal mucosal biopsy which shows villous atrophy.4 Biopsy remains essential for the diagnosis of adult Coeliac disease and cannot be replaced by serology alone. Exceptions are patients with coagulation disorders and pregnant women, in whom biopsy may not be feasible or should be postponed until postpartum.8
In Coeliac disease, the damage to the lining of the intestine is classified according to the Marsh classification scale:7
Marsh 0: lining of the intestine is normal and unlikely that the person has coeliac disease.
Marsh 1: Increased number of lymphocytes seen, but there are normal villi.
Marsh 2: Increased number of lymphocytes, the depressions in the lining of the intestine are deeper than normal, but normal villi length.
Marsh 3: The villi are becoming flattened.
Marsh 4: The villi are completely flattened.
Originally the Marsh scale ranged from 0 to 4, with type 3 indicating Coeliac disease. The scale has since been simplified to allow for more consistency and reproducibility between pathologists.14
There are situations when the diagnosis is not clear. Some patients experience symptoms despite no identified changes on the small bowel biopsy. There is also seronegative Coeliac disease where despite typical symptoms and significant villous atrophy of the duodenal biopsy, there is no serological evidence of the disease.3
Treatment and management
The main treatment of Coeliac disease is a lifelong, strict, gluten-free diet. These include wheat protein, gliadin, rye protein, secalin, and barley protein, hordein. The goal of treatment is to relieve symptoms, achieve mucosal healing, avoid complications of Coeliac disease , and have a good quality-of-life with a nutritionally-complete gluten-free diet.
This is best achieved when patients are motivated, receive expert information and are involved in their own care and treatment. Follow-up and annual review are necessary to ensure adequate response to treatment, prevention of complications, and maintenance of motivation to remain gluten free.8
As a gluten-free diet is the primary treatment option for people with Coeliac disease, it is important that a dietitian or healthcare professional with a specialist interest in Coeliac disease plays a significant role in the patient’s care and follow-up. Many of the common problems associated with the long-term management of Coeliac disease happen because of non-adherence to a gluten-free diet.11 Patient education is important and a healthcare professional with a specialist knowledge of Coeliac disease should explain to the patient, and their family members or carers the importance of a gluten-free diet, and provide detailed information to help the patient follow it.
This should include: information on which types of food contain gluten and suitable alternatives, including gluten-free substitutes, explanations of food labelling information sources about gluten-free diets, recipe ideas and cookbooks, how to manage social situations, eating out and travelling away from home, including travel abroad, avoiding cross-contamination with gluten in the home, minimising the risk of accidental gluten intake when eating out, and the role of national and local coeliac support groups.11
Many everyday foods are gluten free including meat, vegetables, cheese, potatoes and rice. Foods containing gluten include, bread, pasta, cereals, biscuits, crackers, cakes, pastries, pies, gravies and sauces. However, gluten free varieties of these and other products exist. It is important to check the labels on food, as many products, particularly processed food contain gluten additives. Gluten may also be found in non-food products such as some medications, postage stamps, and lipstick.13
Oats contain a protein called avenin which is like gluten, but most people with Coeliac disease can safely eat avenin. Before including oats in the diet, the Coeliac disease patient should talk to a dietician or clinician, and check the oats are pure with no possibility of contamination from other grains. Coeliac friendly versions of oats are widely available. Oats should be avoided until the gluten-free diet is working well. They can be re-introduced into the diet, when the patient is symptom free, but should be stopped if symptoms re-occur.13
Symptoms usually improve over the course of several weeks once a gluten-free diet is initiated. Patients who do not respond need further review, and also an assessment of compliance with the gluten free diet. Serology testing can assess compliance. Non-compliance can be unintentional, and an individual may be still ingesting gluten without realising it.3
Treatment and management involve assessing the impact of malabsorption on the body. Nutritional deficiencies are common in Coeliac disease and should be identified and treated. Full blood count, iron stores, folate, ferritin, vitamin B12, levels of vitamin D and other fat-soluble vitamins, and bone mineral density should be monitored.3 A DEXA scan may be required for those with bone thinning or osteoporosis. A gluten-free diet itself can also be associated with lower levels of certain micronutrients. Fibre, iron, calcium, vitamin D, vitamin B6, vitamin B12 and folate deficiencies have all been noted in people following a gluten-free diet. Gluten-free foods themselves have been shown to be lower in thiamine, riboflavin, niacin, folate, iron, and dietary fibre. This may primarily be because gluten-free foods tend not to be fortified, and be refined.
Coeliac patients should be encouraged to consume foods high in iron and folate to combat these deficiencies, and supplements should be considered if recommended intakes cannot be achieved through diet alone. Calcium and vitamin D deficiencies may also be present and supplements are necessary if intake is insufficient. Other nutritional deficiencies may include magnesium, zinc, niacin, and riboflavin. Most nutritional deficiencies will resolve due to mucosal healing and increased absorption, once a gluten-free diet is established.9
The key elements of managing coeliac disease through diet are to choose and eat foods that are gluten-free; consume a well-balanced diet; including good sources of calcium, iron, vitamin D and B vitamins; eat foods that are rich in fibre; always check foods and fluids in the coeliac society list of gluten-free foods, and check food labels. The emphasis of dietary management in Coeliac disease should focus on the nutritional quality of the diet, and not just simply ‘foods allowed or foods to avoid’.9
Prognosis, outlook, and support
Prognosis for individuals diagnosed early and who remain compliant with a gluten-free diet is good, however, a lifelong diet completely free of gluten can be costly and challenging. Strict compliance with a gluten-free diet is difficult, and relapses are common. Many patients continue to experience symptoms, often due to imperfect adherence to a gluten-free diet.
People with Coeliac disease face a lifelong condition that can be emotionally and physically debilitating, and which left untreated can lead to a significant reduction in quality-of-life. While a large selection of gluten-free products are available in major supermarkets and food outlets with more supports available now than in the past, increased awareness of Coeliac disease as a worldwide health problem is necessary, to help patients cope with the illness and its treatment. Patient support and information is an integral part of the management of Coeliac disease. Clinicians play a lead role by providing ongoing assessment, management, support and education.
Future drug therapies are currently in development with the hope of reducing the burden of living with Coeliac disease, and improving long-term health outcomes. Clinical trials are in progress, but only a few have reached later clinical trial phases. Other scientific challenges include obtaining a better understanding of phenotypes and seronegative coeliac disease. There is ongoing work on developing possible non-dietary therapies that would enable people with Coeliac disease to tolerate gluten. One of the main focuses of the research in this area is immune modulators. Ongoing research and therapeutic strategies aimed at developing a vaccine and desensitising those with Coeliac disease to gliadin peptides, could provide a preventative and definitive cure for Coeliac disease. Identification of future cure and/or alternative treatments to a gluten-free diet brings hope for Coeliac disease patients, who are unavoidably burdened by dietary restrictions.
The Coeliac Society of Ireland https:// coeliac.ie/ is a registered charity that provides information and support to people diagnosed with Coeliac disease throughout Ireland. The Society is part of the European Association of Coeliac Societies (AOECS) involved in setting standards for gluten-free foods both within the European Union and internationally. The society empower the coeliac and gluten intolerant community by providing them with information, food lists, advice and practical solutions as they navigate a gluten-free lifestyle. They represent patient interests by advocating to government health agencies for improved resources and services, so that patients and their families can access the care they need.
THERESA LOWRY-LEHNEN, RGN, GPN, RNP, BSc, MSc, M. Ed, PhD, Clinical Nurse Specialist and Associate Lecturer, South East Technological University
References
Caio G, Volta U, Sapone A, Leffler DA, De Giorgio R, Catassi C, Fasano A. (2019). Coeliac disease: A comprehensive current review. BMC medicine, 17(1), 142. doi: 10.1186/s12916-019-1380-z
Fasano A, Catassi C. Coeliac disease. N Engl J Med. 2012; 367:2419–2426. doi: 10.1056/NEJMcp1113994
Posner E, Haseeb M. (2022). Coeliac disease. Stat Pearls Publishing. Available from: www.ncbi.nlm. nih.gov/books/NBK441900/
Ruiz A. (2021). Coeliac disease. MSD Manual Professional Version. Available at: www.msdmanuals.com/ professional/gastrointestinal-disorders/ malabsorption-syndromes/celiac-disease
Coeliac Society of Ireland. (2021). Getting diagnosed. Available online at: https://coeliac.ie/getting-diagnosed/
Coeliac UK (2022). Advice before testing and recommended tests. Available at: www.coeliac.org.uk/healthcare-professionals/diagnosis/recommended-tests/#:~:text=Testing%20for%20 the%20HLA%20DQ2,consider%20 using%20HLA%20DQ2%20(DQ2
Coeliac UK (2022). Classification of biopsy results. Available at: www. coeliac.org.uk/information-and-support/coeliac-disease/getting-diagnosed/blood-tests-and-biospy/
Ludvigsson J, Bai J, Biagi F, et al. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014; 63: 1210-1228
Coeliac Society of Ireland. (2021). Nutritional Deficiencies. Available online at: https://coeliac.ie/healthcare-professionals/nutritional-deficiencies/
Coeliac Society of Ireland. (2021). Healthcare professionals. Available at: https://coeliac.ie/ healthcare-professionals/
NICE (2015). Coeliac disease: recognition, assessment and management. NICE guideline. National Institute for Health and Care Excellence. Available at: https:// coeliac.ie/wp-content/uploads/2020/06/ coeliac-disease-recognition-assessment-and-management-1837325178565.pdf
Coeliac UK (2022). Conditions linked to coeliac disease. Available at: www. coeliac.org.uk/information-and-support/coeliac-disease/conditions-linked-to-coeliac-disease/
HSE (2021). Coeliac disease. Treatment. Health Service Executive. Available at: www2.hse.ie/conditions/ coeliac-disease/treatment/











Leave a Reply
You must be logged in to post a comment.