NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Ms Carmel Ann Galligan, Candidate Advanced Nurse Practitioner in Haematology
- 04th Dec 2023
To complete this module and earn free CPD points, go to www.doctorCPD.ie and answer the 10 true or false questions and complete the five MCQs based on this article.
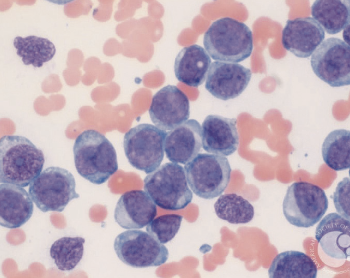
Acute myeloid leukaemia (AML) is an aggressive form of blood cancer that is derived from the over proliferation of ≥20 per cent of immature myeloid blood cells in the peripheral blood, bone marrow or extramedullary tissues. This uncontrolled growth of an immature clone of cells presents as AML. It is a life-threatening malignancy that mainly occurs abruptly in the adult and it may arise, de novo or secondary, from a preceding haematologic disorder, such as myelodysplastic syndrome or be treatment related.
With advances in the management and treatment guidelines, the recovery rates for AML have increased in recent decades to 15 per cent in patients older than 60 years and around 40 per cent in patients below 60 years of age. However, outcomes remain poor compared to many cancers, with high rates of relapse for most patients.
Haematopoiesis
Haematopoiesis is the process of production of blood cells and platelets which continues throughout life, replacing aged cells (which are removed from the circulation). In healthy adults, haemopoiesis is confined to the bone marrow.
Figure 1 shows the visual development from a haematopoietic stem cell (HSC) to what cell it is to become. Haematopoiesis is responsible for producing more than 500 billion blood cells every day – the lifespan of each white blood cell is approximately one-to-three days, red blood cells have a lifespan of 120 days, and platelets have a lifespan of seven-to-10 days.
AML is expressed by mutations of the genes involved in haematopoiesis. These mutations result in a clonal expansion of undifferentiated myeloid progenitor cells (blasts) in the peripheral blood and bone marrow, resulting in ineffective erythropoiesis and bone marrow failure. A differentiation block of these immature myeloid precursors blast cells makes AML blasts unable to complete a normal definite lifecycle. These blast cells are blocked from undergoing normal cell apoptosis and accumulate.
Figure 1: Haematopoiesis
Pathophysiology of AML
AML is defined by a clonal expansion of immature myeloid cells, blast cells, in the peripheral blood and bone marrow resulting in unproductive erythropoiesis and bone marrow failure. This over-production of immature cells overcrowds and inhibits the function of other healthy cells, leading to the symptoms of leukaemia. In AML, this over-proliferation occurs at the split and an accumulation of immature myeloid cells gather in the bone marrow and then pour out into the peripheral blood.
AML can result from genetic mutations, chromosomal translocations, and molecular level changes, and is a heterogeneous disease. Despite AML’s heterogeneous disease course, classification systems have divided it into favourable, intermediate, or adverse-risk groups based on cytogenetics.
Favourable risk AML categories include t(8;21), RUNX1, INV (16), and mutated NPM1+.
About 25-to-30 per cent of AML patients have Nucleophosmin 1 (NPM1+) mutations, which is the most common mutation found in AML and has a female predominance.
All have a favourable prognosis with a three-year overall survival (OS) rate of about 66 per cent in patients aged ≤60 years old, and 33 per cent in the over-60s age group.
AML with intermediate risk include NPM1+ with FLT3-ITD, t(9;11)/MLL:KMT2A, or cytogenetic and/or molecular abnormalities not classified as either favourable or adverse.
AML with adverse risk include t(6;9), t(11q23.3)/KMT2A rearranged, t(9;22)/BCR:ABL1), t(8;16)/KAT6A:CREBBP, INV(3)/Y(3.3), T(3q26.2v)/MECOM rearranged, -5, -7 depletion, complex karyotype, mutated ASXL1, BCOR, EZH2, RUNX1, SF3B1, SRSF2, STAG2, U2AF1, ZRSR2, and TP53 mutated.
This group of patients diagnosed with adverse risks have a poor prognosis and should be considered, if eligible, for haematopoietic stem cell transplant (HSCT).
Each leukaemia patient’s prognostic category is clinically assessed and altered to the individual, as mutations occur in numerous possible combinations and clonal evolution leads to clonal heterogeneity, even at diagnosis.
There are a few risk factors for AML, which include:
A diagnosis of myelodysplastic syndromes or other haematological disorders, which are likely to evolve in to AML.
Congenital disorders, such as Down’s syndrome and Bloom syndrome.
Environmental exposure to radiation, tobacco, benzene.
Previous exposure to chemotherapeutic agents.
Inherited predisposition – familial causes of genetic mutations should also be considered.
Older age.
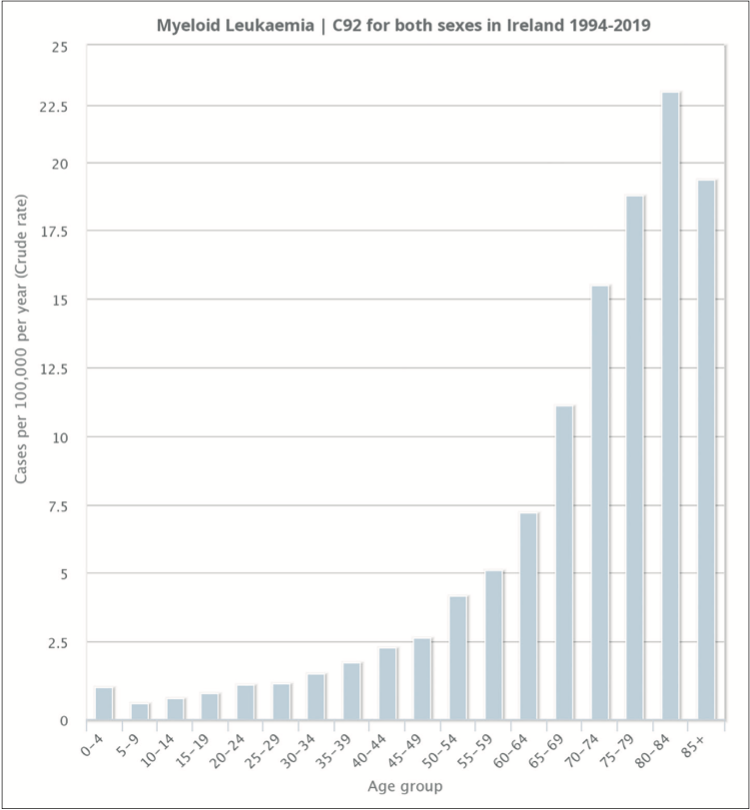
Figure 3: Incidence rate of AML per 100,000 of Irish population and age from 2004-2019
Epidemiology
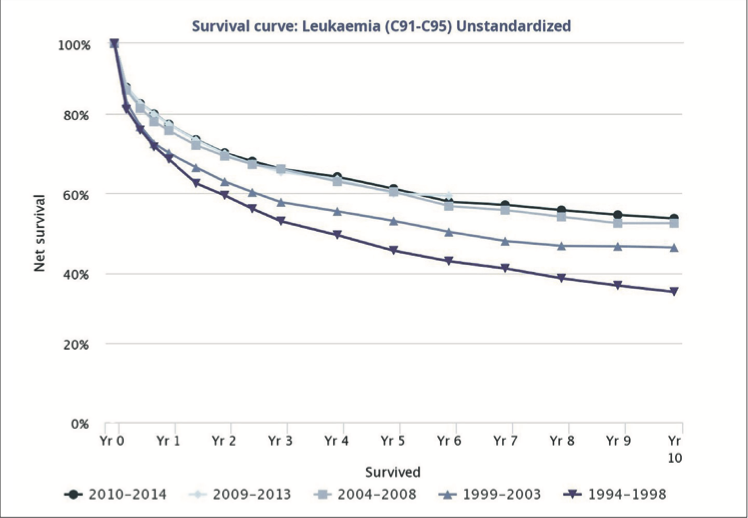
AML is the most common acute leukaemia in adults. It is generally a disease of older people and is uncommon before the age of 45. The average age of people when they are first diagnosed with AML is about 68. In the Republic of Ireland, on average, there are approximately 200 cases of AML per year. The latest incidence and survival data can be seen in graph form in Figure 3 and Figure 4.
Figure 4: Survival curve for all leukaemia diagnoses in Ireland from 1998-2010
AML accounts for <1 per cent of all cancers and 2 per cent of cancer deaths annually in Ireland.
Symptoms and presentation of AML
Clinical presentation and symptoms of AML are dependent on the degree of bone marrow failure secondary to the amount of leukaemia invading the marrow space. Leukaemia originates in the bone marrow and then this over-proliferation leaks into the peripheral blood, which causes the presenting symptoms.
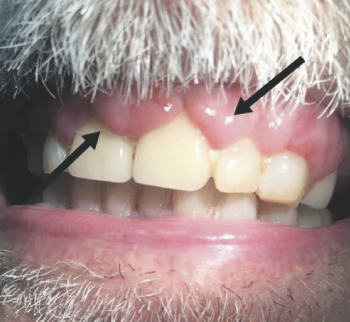
Figure 5: Gum infiltration of AML
As the bone marrow becomes progressively infiltrated with proliferating leukaemia, individuals present with symptoms and signs of bone marrow failure, such as fatigue, pallor, headache secondary to anaemia, and low haemoglobin. Multiple bruising and bleeding can be present secondary to thrombocytopaenia with or without being generally unwell, malaise or having a loss of appetite. Fever and bone pain are also associated with AML at diagnosis secondary to over-proliferation of blast cells, with infection common as white blood cell function is impaired.
Organ infiltration occurs in AML and can affect the gums (Figure 5), the skin (leukaemia cutis, Figure 6), and central nervous system (CNS). Where the CNS is affected, this may or may not present with an altered mental state. Leucocytosis is a high white cell count in an over-proliferation of blast cells circulating around the body, and can cause retinal haemorrhage, pulmonary infiltration, or neurologic symptoms from microinfarction and haemorrhage.
Figure 6: Skin infiltration of leukaemia cutis
Classification of AML
The original AML classification system was the French-American-British system which classified AML into eight subtypes, FAB M0 to M7 associated with morphology alone.
The World Health Organisation (WHO) (2016) revised its classification system to incorporate the advances in particular biomarkers associated in AML retrieved from investigations, such as gene expression analysis and next generation sequencing (NGS).
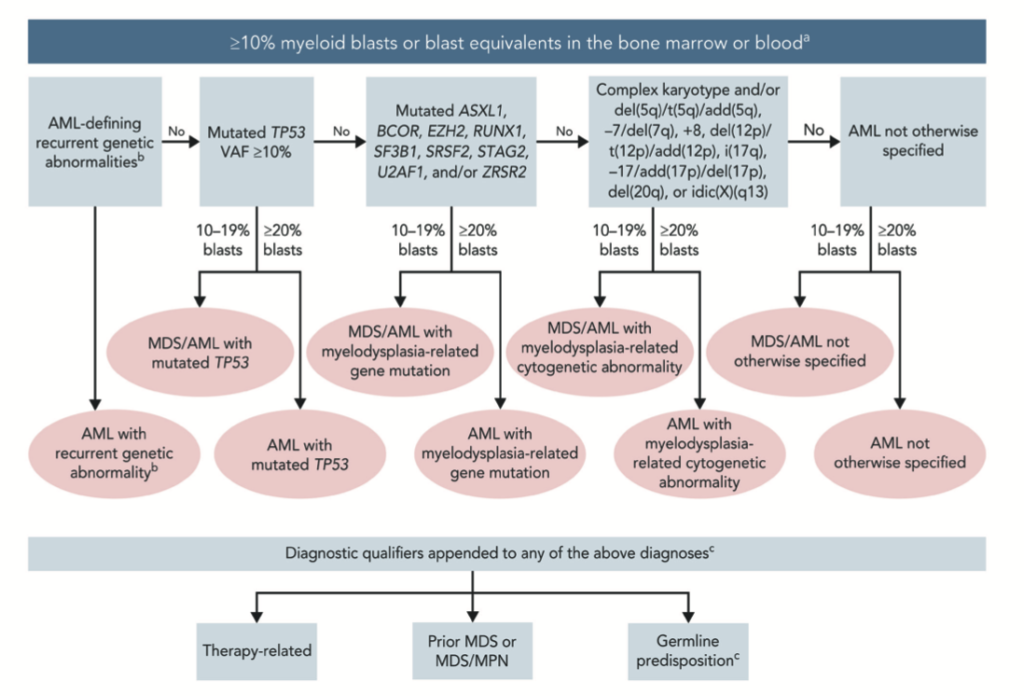
Through national and international publications, the understanding of the molecular pathogenesis of AML has led to an update in the classification of AML – the International Consensus Classification (ICC) of AML. This updated the prior revised fourth edition WHO classification of AML, and introduced changes in the blast thresholds and new genetic entities to define AML, further expanding the spectrum of classification identified by cytogenetic and mutational profiles (Figure 7).
Figure 7: Hierarchical classification of the International Consensus Classification (ICC) of AML
This is now the current classification system used in clinical practice in Ireland. The clinical value of genetic abnormalities for diagnosis and prognosis in AML is vital for the management of these patients. The presence of any familial inherited susceptibility to AML may also be clinically significant. The technological improvement in quantitative assessment of measurable residual disease (MRD) by polymerase chain reaction (PCR) is applicable to AML with: NPM1 mutations, Inversion 16 chromosome, t(8;21) translocation. PCR MRD has a sensitivity of 1/10,000 – 1/100,000. Therefore, highly-sensitive tests are required in monitoring these patients during and post-treatment. The ability to assess a therapeutic response to treatment and disease response has led to the improvement of treatment plans and evolution of novel therapeutic agents. They include FLT 3, IDH 1, IDH 2, and BCL 2 inhibitors, and development in the management in HSCT.
Diagnosis
Diagnosis of AML is a rapid process, which requires a comprehensive assessment of the patient. Multiple tests and procedures are required to yield a diagnosis. Initially, a full blood count with blood film is requested and reviewed by a haematologist, and a bone marrow aspirate and trephine biopsy, immunophenotyping by flow cytometry, and cytogenetic analysis is sent from the marrow sample.
A full patient history to include medical, social, and family history is completed by the haematology team in an acute hospital setting. A physical assessment is performed, and performance assessment and frailty assessment status (ECOG and clinical frailty scale). Other blood works include renal, liver, bone profiles, coagulation screen, magnesium, lactate dehydrogenase (LDH), uric acid, full virology screen, human chorionic gonadotropin (HCG) if applicable, and human leukocyte antigen (HLA) test if eligible for HSCT. Other tests can include chest x-ray, 12-lead electrocardiogram, echocardiography, CT scan, lumbar puncture if clinically indicated, and biobanking.
All the outlined tests and procedures are completed rapidly to establish a diagnosis and thereby create a treatment plan individually tailored to suit each patient. Fertility preservation for female oocyte cryopreservation and sperm cryopreservation will be discussed with each patient secondary to the aggressive disease state. In AML, fertility preservation is not always possible due to urgency to treat the patient, but is discussed, and where possible, undertaken at the patient’s request.
Treatment options
The latest European Society for Medical Oncology (ESMO) Clinical Practice Guidelines for diagnosis, treatment, and follow-up of AML in adult patients were published in 2020, and are available at: www.annalsofoncology.org/article/S0923-7534(20)36079-8/fulltext.
The standard therapy for AML patients eligible for intensive induction therapy has not changed significantly in the past 40 years: Induction therapy with combination chemotherapy, followed by consolidation therapy to maintain remission. Some eligible patients with intermediate/poor risk disease may also receive a stem cell transplant along with consolidation therapy.
When commencing AML treatment, the aim is to control and eradicate the disease and ideally place the patient in remission after the first cycle of intensive chemotherapy. While the treatment go-to options for AML have not changed dramatically for induction chemotherapy treatment; over the past five years, the introduction of new model targeted therapies has allowed for a more targeted and patient-specific treatment plan.
New agents include:
Midostaurin, a multi-targeted protein kinase inhibitor, received European Medicines Agency (EMA) approval in September 2017 for previously untreated AML with FLT3+ mutated.
Liposomal daunorubicin and cytarabine was approved by the EMA for newly-diagnosed t-AML or AML-MRC in August 2018.
Gemtuzumab ozogamicin received EMA approval for newly-diagnosed CD33+ AML in April 2018.
Gilteritinib was approved by the EMA in 2019 for relapsed or refractory AML with FLT3+ mutated (EMA, 2023).
Venetoclax was approved by the EMA in May 2021 for use in combination with a hypomethylating agent, and is indicated for the treatment of adult patients with newly-diagnosed AML who are ineligible for intensive chemotherapy (EMA, 2023).
The HSE National Cancer Control Programme (NCCP) develops national systemic anti-cancer therapy (SACT) regimens to support safe, evidence-based and cost-effective cancer treatment for all Irish cancer patients. These regimens include specific indications for specific drugs and the list for leukaemia is available here: www.hse.ie/eng/services/list/5/cancer/profinfo/chemoprotocols/leukemia-bmt/protocols%20leukaemia.html.
Chemotherapy
Age, frailty, co-morbidity, genetics, and patient requests and wants are involved in the individual AML treatment plan.
Initial patient assessment determines whether a patient is eligible for intensive induction chemotherapy or not. Patients are classified into intensive (fit patients, usually younger) or non-intensive (unfit patients or older) chemotherapy regimens to control the disease burden.
The aim of induction is to achieve complete remission (ie, bone marrow blasts <5 per cent; absence of circulating blasts; absence of extramedullary disease; absolute neutrophil count ≥1,000/microlitre; platelet count ≥100,000/microliter); and reduce the risk of relapse.
Younger patients (<60 years of age) who are fit and able to tolerate intensive therapy should undergo induction therapy with standard dose-intense chemotherapy regimens.
Older patients can also be considered for intensive therapy if deemed suitable (eg, based on performance status, cytogenetic/molecular profile, and comorbidities).
The standard induction chemotherapy regimen is based on a backbone comprising infusional cytarabine followed by an anthracycline (eg, daunorubicin or idarubicin). A complete remission rate in this induction is about 70 per cent with this regimen. Again, see the aforementioned HSE NCCP protocols for more information.
At this stage, all cytogenetic and/or molecular abnormalities are available to classify using the ICC system, and a decision for chemotherapy alone versus HSCT if required. After induction therapy when a complete remission is achieved, due to the aggressive nature of leukaemia, consolidation treatment is undertaken always with a second cycle of a cytarabine-based regimen or proceeding to HSCT if warranted after second induction.
Non-intensive treatment or treating the unfit patient in clinical practice
Azacitidine is used as a single oral agent, giving complete response rates of about 30 per cent with a four-month response rate with a median OS rate of less than one year. Azacitidine is well tolerated in this cohort of patients.
Since 2021, considerable advances in treating this patient group have occured, with the addition of the BCL2 inhibitor venetoclax, which has improved clinical response to 66.4 per cent in comparison to azacitidine single agent of 28.3 per cent response rate. It has also shown a greater median OS rate of 14.7 months compared to 9.6 months with single agent azacitidine; therefore, this data provides promising evidence to establish a new standard-of-care for older or unfit patients with AML.
Approximately 10-to-20 per cent of younger and 50 per cent of older AML patients do not achieve complete remission after at least two courses of intensive induction therapy, and 50-to-70 per cent of patients who obtain complete remission will relapse.
The prognosis of primary refractory and relapsed AML patients remains poor and treatment is challenging. A primary consideration in the therapeutic approach of refractory or relapsed AML patients should be their suitability for intensive chemotherapy and alloHCT (ESMO). Mutation analysis for FLT3 should be repeated in relapsed patients, as gilteritinib is approved in the relapse setting of FLT3-ITD- and FLT3-TKD-mutated patients.
Emerging options
The further successful development of treatment and management of AML lies with ongoing clinical trials. In Ireland, two clinical trials are open for newly-diagnosed AML patients.
HOVON 150 is a phase 3, multicentre, double-blind, randomised, placebo-controlled study of ivosidenib vs placebo (IDH1) or enasidenib vs placebo (IDH2) (AG-120 or AG-221) in combination with induction therapy and consolidation therapy followed by maintenance therapy in patients with newly-diagnosed AML or myelodysplastic syndrome with excess blasts-2 with an IDH-1 or IDH-2 mutation eligible for intensive chemotherapy (St James’s Hospital (SJH), Dublin, 2023).
HOVON 156 is a phase 3, multicentre, open label, randomised study of gilteritinib versus midostaurin in combination with induction and consolidation therapy followed by one-year maintenance in patients with newly-diagnosed AML or myelodysplastic syndromes with excess blasts-2 (MDS-EB2) with FLT3 mutations eligible for intensive chemotherapy (SJH, 2023).
Conclusion
In this CPD module, you have gained an insight and understanding of AML, its pathology, symptoms, diagnosis, treatments, and current clinical practice guidelines in an Irish setting.















Leave a Reply
You must be logged in to post a comment.