NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Theresa Lowry Lehnen, RGN, GPN, RNP, PhD, National PRO of the IGPNEA, Clinical Nurse Specialist Practitioner and Associate Lecturer at Institute of Technology Carlow, and Assistant PRO, Irish Student Health Association
- 06th Aug 2021
Young sick woman with hands holding pressing her crotch lower abdomen. Medical or gynecological problems, healthcare concept. Young woman suffering from abdominal pain while sitting on sofa at home
An overview of the latest diagnostic guidelines and treatment approaches to one of the most common gastrointestinal conditions
Irritable bowel syndrome (IBS) is a common, chronic gastrointestinal (GI) disorder characterised by symptoms of abdominal pain and disturbances in bowel habits in the absence of known organic pathology. The condition affects between 5 and 10 per cent of healthy individuals at any one time and in most people runs a relapsing and remitting course. IBS is recognised as a multifactorial disorder, with GI dysmotility, inflammation, visceral hypersensitivity and altered intestinal microbiota contributing to symptomatology.1 Symptoms of IBS include loose, frequent stools, constipation, bloating, and abdominal pain and cramps. Patients may notice symptoms following the intake of specific foods or that symptoms, such as stool consistency or pain location, change over time. Patients may also present with headache, lethargy, nausea, bladder symptoms or faecal incontinence.1,2,9
The condition typically occurs before the age of 45 years and is more common in people aged 20-to-30 years.5 IBS appears to become less common with age and does not affect life expectancy or lead to other serious diseases. IBS affects both men and women, but the condition occurs more frequently in women. Women tend to have more frequent and severe IBS symptoms during menses and menopausal women have fewer symptoms than women who are still menstruating.10 Women more commonly report symptoms of abdominal pain and constipation, while men more commonly report diarrhoea. Men, however, are much less likely than women to report signs of IBS.2,4
The causes and pathophysiology of IBS are complex and remain poorly understood. Theories include combinations of gut-brain axis problems, gut motility disorders, pain sensitivity, infections including small intestinal bacterial overgrowth, neurotransmitters, genetic factors, and food sensitivity. Onset may be triggered by an intestinal infection or stressful life event. It is thought that a number of factors may contribute to development of the disorder.
Psychiatric comorbidities are present in approximately 50 per cent of IBS patients and include depressive symptoms, anxiety and eating disorders
Genetic predisposition and environmental interactions, such as familial susceptibility and psychosocial stressors, have been implicated in the multifactorial pathogenesis of IBS.1 Diet and stress have been proposed as contributing factors to this heterogeneous disorder. Because stress has been identified as a mechanism in the development of IBS, the major components of the stress response system, the autonomic nervous system (ANS) and the hypothalamic-pituitary-adrenal (HPA) axis, have been the subject of numerous investigations of IBS.1
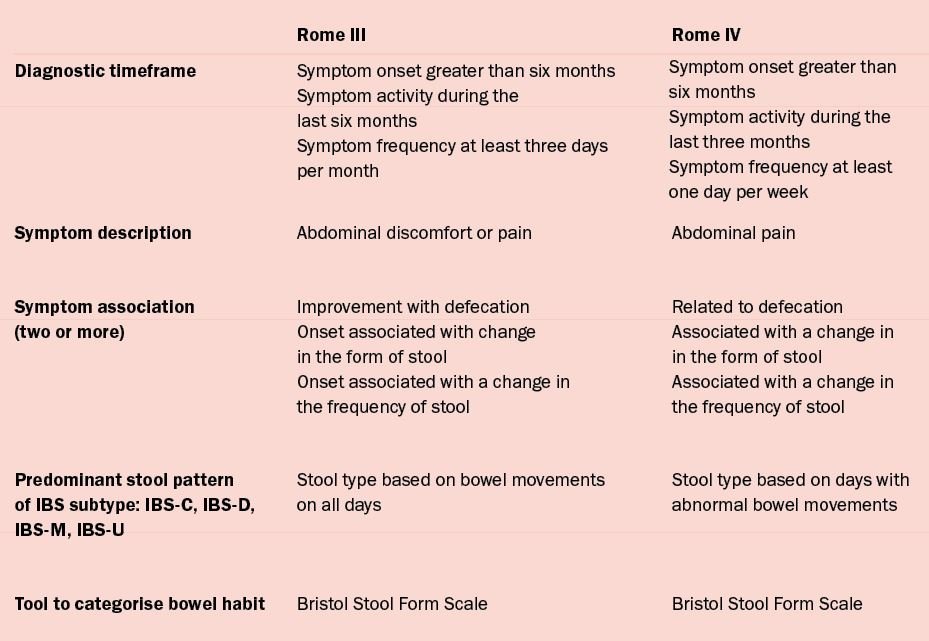
Table 1: Rome criteria1 for IBS classification
IBS is commonly associated with other functional, somatoform and mental disorders. In over 20 per cent of cases, there is an overlap of IBS with functional GI disorders of the upper GI system, particularly functional dyspepsia and gastro-oesophageal reflux disease (GORD), and of the lower GI system, such as diarrhoea, incontinence, pelvic floor dyssynergia, and constipation. Psychiatric comorbidities are present in approximately 50 per cent of IBS patients and include depressive symptoms, anxiety and eating disorders.10
A strong association between GI infections and the development of IBS has been established. Around one in nine patients exposed to infectious enteritis may develop IBS, at a rate four times higher than non-exposed individuals. The greatest risk is associated with protozoal and bacterial infections, with viral infections having a lower risk of development of IBS. The severity of acute gastroenteritis increases the risk of developing IBS, but symptoms usually decrease over time.10 In IBS, the epithelial barrier, gut microbiota, food antigens, and bile acids give rise to abnormal responses in the main regulators of sensorial and motor functions, such as the hypothalamus-pituitary-adrenal axis, the immune system, the brain-gut axis and the enteric nervous system.10
Classification criteria and diagnosis
IBS has been categorised as a functional bowel disorder, ie, it is not associated with any structural or biochemical abnormalities in the GI tract. No specific laboratory or imaging tests can diagnose IBS. The Rome criteria (See Table 1) are used to diagnose IBS when the presence of organic disease such as inflammatory bowel disease (IBD), colon cancer, and Coeliac disease have been excluded.1,2
IBS has been categorised as a functional bowel disorder, ie, it is not associated with any structural or biochemical abnormalities in the GI tract
The Rome III classification diagnostic criteria served as the symptom-based, diagnostic criteria for IBS since their release in 2006 and subtyped IBS patients based on predominant stool pattern: Constipation (IBS-C), diarrhoea (IBS-D), mixed (IBS-M) or unsubtyped (IBS-U). Rome III classified the disorder by symptom onset greater than six months and recurrence of at least three days per month during the last three months. Diagnostic criteria required abdominal discomfort or pain to be associated with two or more of the following: Improvement with defecation, onset associated with change in the form of stool, or onset associated with a change in the frequency of stool.
In early 2016 the Rome Foundation released Rome IV, an updated classification system for conceptualising and diagnosing functional GI disorders.1 The Rome IV definition of IBS maintains symptom chronicity greater than six months and current activity present within the prior three months, however, symptom frequency has been changed to at least one day per week from at least three days per month. Pain related to bowel movements is required, rather than just improving with bowel movements, because, in some cases, pain can worsen after bowel movements. The ‘onset’ of abdominal pain has been eliminated from the association of pain with changes in stool.
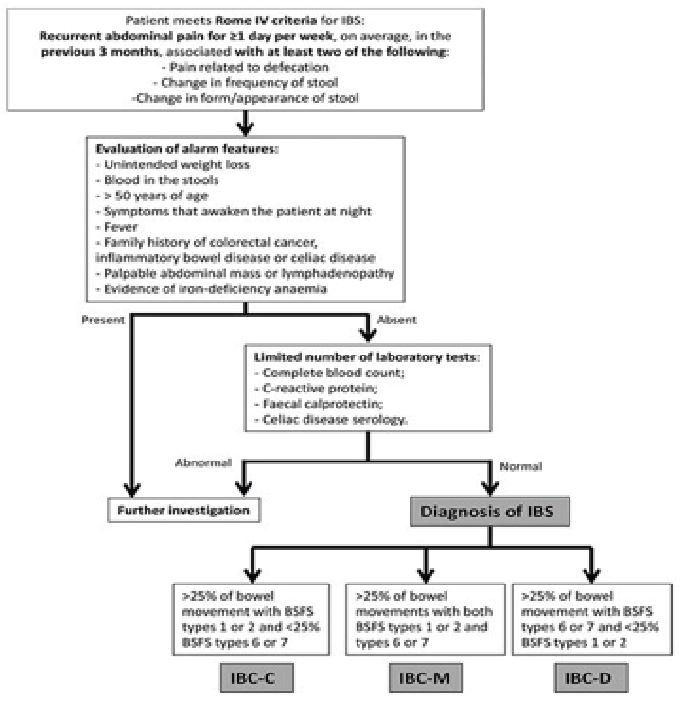
Figure 1: Algorithm for the diagnosis of IBS. BSFS, Bristol Stool Form Scale; IBS-C, IBS with predominant constipation; IBS-D, IBS with predominant diarrhoea; IBS-M, IBS with predominant irregular bowel habits (mixed C/D)10
Rome IV also updated the subtyping of IBS patients (IBS-C, IBS-D, IBS-M and IBS-U), in that stool type is based on days with abnormal bowel movements, as opposed to bowel movements on all days. The term ‘discomfort’ was eliminated from the criteria because it is non-specific and has different meanings in different languages. Rome IV retains the Bristol Stool Form Scale as a useful tool to categorise bowel habit.1,10 The Rome IV process also redefined IBS as a disorder of gut-brain interaction, in recognition of the complex interplay of biological, psychological, and social factors underpinning the condition.11
In the absence of any biomarker being available for IBS, the condition is diagnosed using a positive approach, based on the clinical history. To make an accurate diagnosis of IBS, it is generally recommended to incorporate Rome IV criteria along with the patient history including dietary questions, physical examination including abdominal and anorectal examination, laboratory tests such as full blood count, C-reactive protein or erythrocyte sedimentation rate (ESR), possible Coeliac disease serology, and when indicated a colonoscopy and/or upper GI endoscopy and other tests. An abdominal x-ray can be considered to rule out faecal loading if constipation is the predominant symptom. When Rome IV criteria are present and alarm features are absent, only a limited number of laboratory tests are recommended without the need to perform invasive investigations.10
Patients may have IBS-type symptoms for many years without presenting to medical care, often self-managing their symptoms without medical input, and some may never consult. Nevertheless, lower GI symptoms frequently prompt people to present to primary care, accounting for approximately one-in-12 of all consultations.11 Functional GI disorders, such as IBS, are by far the most common diagnosis, but symptoms can be difficult to assess and the possibility of colorectal cancer or IBD may create diagnostic uncertainty for clinicians, and anxiety for patients.11 GPs are usually the first point of contact and provide the diagnosis and medical care for most people with IBS.
Management guidelines encourage GPs to make a positive diagnosis of IBS, based on symptoms, in the absence of alarm symptoms or signs that warrant referral to exclude colorectal cancer or abnormalities on simple investigations. However, persistent abdominal bloating or distension in female patients should prompt consideration of CA-125 and pelvic ultrasound to exclude ovarian cancer.11 It is important to question patients about dietary and medication changes, life stressors and support networks, as part of the diagnostic assessment.
Alternative diagnoses that should be considered when patients present with IBS symptomatology include Coeliac disease, microscopic colitis (MC), IBD including Crohn’s disease and ulcerative colitis, bile acid malabsorption, colorectal cancer, and dyssynergic defecation.3 Once a diagnosis of IBS has been made, the GP should endeavour to follow-up with the patient within the next two months to ensure symptoms are not getting progressively worse, which may be indicative of a more sinister underlying disease process.11
BSG guidelines on the management of IBS (July, 2021)
The newly published (July, 2021) British Society of Gastroenterology (BSG) guidelines on the management of IBS (available at https://gut.bmj.com/content/70/7/1214) state: “This more restrictive nature of the Rome IV criteria calls into question whether they should be used to diagnose IBS in clinical practice, and a more pragmatic definition of the symptoms that constitute IBS may be preferred.
The National Institute for Health and Care Excellence (NICE) guideline for the management of IBS in primary care recommends a broader, more pragmatic, definition of IBS, focusing on abdominal pain or discomfort associated with altered stool frequency or stool form for at least 6 months, in the absence of alarm symptoms or signs, and acknowledging that coexistent bloating, lethargy, nausea, backache or bladder symptoms are common.”11
Furthermore, the 2021 BSG guidelines with regard to the diagnosis of IBS in primary care state: “The Rome diagnostic criteria are based on specific symptoms of a defined duration and frequency, which have been derived predominantly from secondary care patients and are rarely used in primary care. Their applicability to clinical practice has been challenged as unnecessarily restrictive and only a minority of people diagnosed with IBS in primary care fullfill them. “This restrictive diagnostic approach to IBS may be unhelpful and overly complicated in this setting, where fundamentals of clinical management are common across all these functional gastrointestinal disorders.
Applying rigid criteria potentially leaves many patients with troublesome impactful symptoms without a clear diagnosis, increasing uncertainty and leading to issues with providing appropriate advice and management options. The NICE guideline definition of IBS is therefore preferable.”11
The new BSG 2021 guidelines also point out: “The fall in prevalence in IBS that results from the changes made in moving from the Rome III to Rome IV criteria is noteworthy, reflecting the more restrictive nature of the latter. This has important clinical implications because, although as intended, the criteria are now more specific for diagnosing IBS, up to 50 per cent of patients who believe they have IBS will no longer meet criteria for the condition. Instead, they will be diagnosed as having another functional bowel disorder, such as functional diarrhoea, functional constipation or functional abdominal bloating or distension.
“Moreover, there may be an impact on treatment trials in IBS, and the interpretation of results, because patient populations recruited using the Rome IV criteria will differ from those recruited using Rome III, and may have more severe symptoms and higher degrees of psychological comorbidity Moving from Rome III to Rome IV IBS may therefore reduce the likelihood of novel pharmacological therapies demonstrating efficacy in future randomised controlled trials (RCTs), due to the spectrum of symptom severity, or may mean that trials need to be considerably larger, and therefore more expensive to conduct, to show a beneficial effect.”
Other novel approaches include drugs that act on cannabinoid receptors, which are expressed in the GI tract and may also modulate pain expression
Treatment
There is no known permanent ‘cure’ for IBS. Treatment is focused on symptom control, in order to improve quality-of-life. There is no definitive treatment for the management of the condition and a combination of lifestyle and dietary advice and use of pharmacological therapies is often required. Pharmacological management including laxatives, antidiarrhoeals and certain antispasmodics is centred on treatments that alleviate symptoms of IBS, but which are not specifically authorised for IBS itself. Education and reassurance is an important aspect of patient care and treatment, explaining the natural history of the disease and providing reassurance that it is a benign condition.
It is important to build up a good rapport with the patient, including them in the decision-making process and ensuring their voice and concerns are heard as well as validating their symptoms. Management of IBS involves an integrated approach and treatment options include establishment of an effective patient-provider relationship, education, reassurance, nutritional interventions, pharmacological and psychological therapy.2,5,9,10
Key skills, in relation to chronic disorders such as IBS in general practice, are for the GP/clinician to make a positive diagnosis, provide a simple explanation of the pathophysiology underlying the symptoms, clarify the patient’s main concerns and manage current symptoms in the wider context of the patient’s life. The clinician-patient relationship, continuity of care, empathy, including acknowledgement of the impact of symptoms on daily life, a shared understanding of IBS and shared decision-making can assist in providing appropriate education, signposting to reputable online information or peer support, reassurance, advice and management options.
There should be a realistic discussion concerning the limitations of all available treatments for IBS to manage expectations. It is important to stress that cure is unlikely, but substantial improvement in symptoms, social functioning and quality-of-life is achievable.11
Pharmacological therapy
The choice of pharmacological therapy depends on the nature and severity of IBS symptoms. Many drug treatment options for IBS are available over-the-counter (OTC). Antispasmodics are among the most frequently used OTC treatments for IBS and can be broadly divided into antimuscarinics and smooth muscle relaxants. Antimuscarinics, including dicycloverine, propantheline, otilonium bromide and hyoscine butylbromide, reduce intestinal motility, whereas alverine and mebeverine are direct-acting intestinal smooth muscle relaxants.11
Butylscopolamine, due to its ability to antagonise the binding of acetylcholine to the muscarinic receptor at the neuromuscular junction, leads to smooth muscle relaxation, however, due to antimuscarinic adverse effects such as constipation, it should not be used in patients with IBS-C.10 Mebeverine, a spasmolytic without atropine-like side-effects, has high efficacy for abdominal pain and reduction in daily defecation frequency, as well as an improvement in well-being, with good tolerability with minor complications.
Peppermint oil inhibits smooth muscle contraction through calcium channel blockade and has been proven to reduce IBS symptoms, being a safe and effective treatment. Antispasmodics are thought to improve symptoms of abdominal pain and have been shown to provide short-term relief of symptoms.5,10
Osmotic laxatives such as polyethylene glycol are often recommended to improve constipation for those with IBS-C, however, they have not been shown to improve abdominal pain or bloating. Stimulant laxatives may also be used. Lactulose is not recommended, as it increases gas production, causes bloating and can exacerbate symptoms.2 Patients who have not responded to laxatives from the different classes and who have constipation for at least 12 months can be treated with linaclotide, however, caution must be taken due to its predisposition to fluid and electrolyte imbalance. Linaclotide is contraindicated in GI obstruction inflammatory disease.5
Loperamide hydrochloride is the first-line choice of anti-motility drug for relief of diarrhoea due to its action on opioid receptors in the GI tract, and because it does not readily cross the blood brain barrier. It inhibits peristalsis, prolongs gut transit and reduces faecal volume. As constipation is an adverse effect, it should be used with caution for patients with IBS-M. Patients with IBS should be advised how to adjust their dose of laxative or anti-motility drug according to stool consistency with the aim of achieving a soft, well-formed stool.2,5
A low-dose tricyclic antidepressant (TCA), such as amitriptyline hydrochloride (unlicensed indication) can be used for abdominal pain or discomfort as a second-line option in patients who have not responded to antispasmodics, anti-motility medications or laxatives. They should be commenced at a low dose, eg, 10mg amitriptyline once a day and titrated slowly to a maximum of 30-50mg once a day.11 An SSRI may be considered in those who do not respond to a tricyclic antidepressant. As with tricyclic antidepressants, they can be initiated in primary or secondary care, but careful explanation as to the rationale for their use is required, and patients should be counselled about their side-effect profile.5,9,11
Non-pharmacological treatment
Psychological interventions can be offered to patients who have no relief of IBS symptoms after 12 months of drug treatments. There is good evidence that psychological treatments directed against IBS symptoms, especially cognitive behavioural therapy (CBT) and hypnotherapy, are helpful for many patients’ symptoms, but unfortunately these are not always readily accessible.5,11
Diet and lifestyle changes are important for effective self-management of IBS. First-line dietary advice should be offered to all patients with IBS. Patients should be encouraged to increase physical activity, with recommended guidelines of 30 minutes at least five days a week and advised to eat regularly without missing or leaving long gaps between meals. Dietary advice should also include limiting fresh fruit consumption to no more than three portions per day. The fibre intake of patients with IBS should be reviewed. If an increase in dietary fibre is required, soluble fibre, such as ispaghula husk, or foods high in soluble fibre, such as oats, are recommended. Intake of insoluble fibre such as bran and resistant starch should be discouraged as they may exacerbate symptoms.
Fluid intake, mainly water, should be increased to at least eight cups per day and the consumption of caffeine, alcohol and carbonated drinks reduced/avoided. Artificial sweetener sorbitol should be avoided in patients with diarrhoea. Where probiotics are being used, continue for at least four weeks while monitoring the effect.5,9,11
A growing focus of clinical research has been to improve IBS symptomatology through dietary modifications.6 Over 80 per cent of individuals with IBS report food-related symptoms, especially to fermentable carbohydrates and fats.11 Food ingestion can contribute to the generation of symptoms through stimulation of chemoreceptors, mechanoreceptors, by osmotic actions, altered secretion, activation of motor reflexes, and colonic fermentation. Dietary intolerance in IBS patients has been attributed to gluten, wheat, lactose, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) as well as fructose malabsorption. FODMAPs are short chain carbohydrates found in a variety of fruits, vegetables, dairy products, artificial sweeteners, and wheat that are poorly absorbed in the small intestine and subsequently fermented by bacteria in the distal small and proximal large intestine.11 This is a normal phenomenon, common to everyone.
The resultant production of gas potentially results in bloating and flatulence. Although FODMAPs can produce certain digestive discomfort in some people, they do not cause intestinal inflammation and can also help avoid it, because they produce beneficial alterations in the intestinal flora that contribute to maintaining the good health of the colon. FODMAPs are not the cause of IBS nor other functional GI disorders, but rather a person develops symptoms when the underlying bowel response is exaggerated or abnormal.7 A low FODMAP diet is recommended as a second-line diet for IBS, under the guidance of a trained dietitian.11 Exclusion diets have been used in patients with IBS, for instance with wheat and dairy, although conflicting results have been reported.1 Food elimination diets based on IgG antibodies are not recommended in patients with IBS.11
Parallel to the focus on dietary modifications are efforts to alter the intestinal microbiota. Undigested food is used by intestinal microbes (GI microbiota) upon entering the intestine, and microbiota play a major role in GI processes and overall health.8 The faecal microbiome of patients with IBS may differ significantly from that of healthy individuals. The theory that this might, in part, be involved in pathophysiology has led to interest in whether probiotics can be used to alter the microbiome.11
Numerous studies have investigated the utility of probiotics in IBS, in efforts to manipulate the intestinal microbiota and improve symptomatology.8 Although there are some inconsistencies in different studies, there is sufficient evidence to suggest their efficacy in reducing IBS symptoms, such as bloating, abdominal pain and flatulence.10
New therapies
Novel drugs that have been tested successfully in chronic idiopathic constipation, including elobixibat and mizagliflozin, a sodium-glucose cotransporter-1 inhibitor, are likely to undergo testing in IBS-C.11 Plecanatide, a peptide guanylate cyclase C receptor agonist is a promising therapeutic option and an efficacious second-line drug for IBS-C in secondary care. In a phase 3 clinical trial it led to a significant reduction of IBS symptoms, however, diarrhoea is a common side-effect. Although the drug is licensed for IBS with constipation in the US, it is not yet available for this indication in many countries.10,11 Tenapanor, an inhibitor of the GI sodium/hydrogen exchanger NHE3 and an efficacious second-line drug for IBS with constipation in secondary care, is another novel agent.
It increases intestinal fluid volume and transit, leading to an improvement of constipation, bloating and pain. Again, diarrhoea is a frequent side-effect and although the drug is licensed for IBS with constipation in the US, it is also not yet available for this indication in many countries.10,11 Tegaserod, a 5-Hydroxytryptamine 4 receptor agonist, is also an efficacious second-line drug for IBS with constipation in secondary care, but is unavailable outside the US and diarrhoea is a common side-effect.11 Colesevelam, a bile acid sequestrant, has been evaluated in patients with IBS-D.
Clinical trials demonstrated that colesevelam increases the delivery of bile acids to stools, improving stool consistency, and increases hepatic bile acid synthesis, avoiding steatorrhoea in IBS-D patients.10 The highly selective 5-HT4 agonist minesapride has been studied in two phase 2 dose-ranging RCTs in patients with IBS-C. A dose of 40mg once a day was superior to placebo, in terms of improvements in number of bowel movements per week, abdominal pain and global symptoms. The drug was well-tolerated, with diarrhoea the most common side effect, and there were no cardiovascular adverse events.11
Other novel approaches include drugs that act on cannabinoid receptors, which are expressed in the GI tract and may also modulate pain expression.11 Although faecal microbiota transplantation (FMT) was thought to be a potential therapeutic option, current evidence suggests there is no improvement in global IBS symptoms after FMT.10
Efforts in identifying the different pathophysiological mechanisms involved in symptom generation have allowed the development of new symptom-based and target edtherapies. New insights and ongoing research into trials of novel treatments, including pharmacological, dietary and behavioural therapies, device-based treatments and FMT will hopefully bring a better quality-of-life to patients with IBS, as they contribute to a new understanding of this common syndrome.
References
Weaver K, Melkus G, Henderson A. (2017). Irritable bowel syndrome: A review. American Journal of Nursing: June 2017 – Volume 117 – Issue 6 – p 48-55 doi: 10.1097/01.NAJ.0000520253.57459.01. www.ncbi.nlm.nih.gov/pmc/articles/PMC5453305/
Callachand N. (2020). Irritable bowel syndrome in focus. Medical Independent. Published August 6 2020. Available at: www.medicalindependent.ie/irritable-bowel-syndrome-ibs-in-focus/
Lacy B, Mearin F, Chang L, Chey W, Lembo A, Simren M, Spiller R. (2016). Bowel disorders. Gastroenterology. 2016; 150:1393–1407. doi: 10.1053/j.gastro.2016.02.031
Healthline (2021). Everything you want to know about IBS. Available at: www.healthline.com/health/irritable-bowel-syndrome
BNF British National Formulary (2020). Edition 80. September 2020 – March 2021. British Medical Association/Royal Pharmaceutical Society, London
Chey W. (2016). Food: The main course to wellness and illness in patients with irritable bowel syndrome. American Journal of Gastroenterology. 2016;111:366-371. doi: 10.1038/ajg.2016.12
Mullin G, Shepherd S, Chander R, Ireton-Jones C, Matarese L. (2014). Irritable bowel syndrome: Contemporary nutrition management strategies. Journal of Parenteral and Enteral Nutrition. 2014;38:781–799. doi: 10.1177/0148607114545329
Barbara G, Feinle-Bisset C, Ghoshal U, Santos J, Vanner S, Vergnolle N, Quigley E. (2016). The intestinal microenvironment and functional gastrointestinal disorders. Gastroenterology. 2016;150:1305–1318. doi: 10.1053/j.gastro.2016.02.028
NHS (2021). Irritable Bowel Syndrome. National Health Service, UK. Available at: www.nhs.uk/conditions/irritable-bowel-syndrome-ibs/
Ferreira A, Garrido M, Castro-Poças F. (2020). Irritable Bowel Syndrome: News from an Old Disorder. GE Port J Gastroenterol 2020; 27:255–268
BSG (2021). British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. British Medical Journal. Volume 70, Issue 7. Available at: https://gut.bmj.com/content/70/7/1214












Leave a Reply
You must be logged in to post a comment.