







Pat Kelly examines a recent report from the US on physician suicide and highlights the work of Ireland’s Practitioner Health Matters Programme to provide wellbeing support to doctors.
The recent publication of the Medscape Physician Suicide Report provided some startling statistics on the mental health of doctors, including that physicians have suicidal thoughts at just below twice the rate of the general population, at 7.2 per cent compared to 4 per cent.
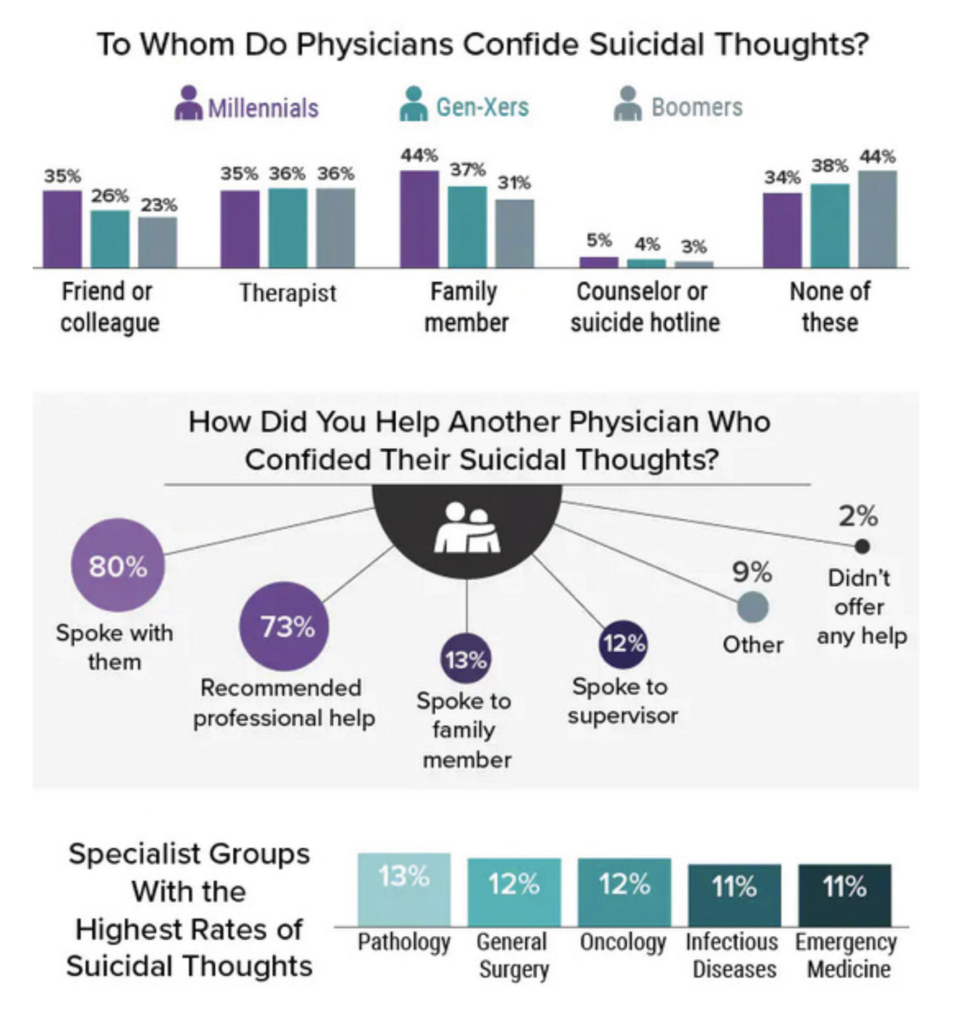
The researchers surveyed more than 13,000 physicians across 29 specialties in the US. The scope of the questions ranged from depression, to suicidal ideation, to coping strategies and how they support distressed colleagues. Among the top-line statistics, it was found that some 21 per cent of doctors reported having depression. Of these, 24 per cent had diagnosed depression, and 64 per cent had ‘colloquial’ depression. Whilst the overall number of doctors who reported suicidal ideation dropped to 9 per cent (from 22 per cent in 2020), one-in-10 physicians still said they had thought about or attempted suicide, and there was a rise in the number of women physicians who said they contemplated taking their own life. Over a period of years, the percentage of doctors who had attempted but not completed suicide remained steady, at 1 per cent.
The specialties of pathology (13 per cent), and general surgery and oncology (12 per cent) were the specialist groups with the highest rates of suicidal ideation. Further, 44 per cent said they had not confided in anybody regarding these thoughts (see Figure 1).
Medscape points out that globally, physicians have a lower mortality rate from conditions such as heart disease and cancer, for example, than the general population. This is attributed to a medical professional’s greater awareness of symptoms, adherence to a healthy lifestyle, and access to early diagnosis and treatment. However, it is also recognised that doctors have a higher risk of dying by suicide compared with the general population.
The figures on physicians’ death by suicide are difficult to quantify due to coding and reporting inaccuracies; however, the authors note that a generally accepted estimate is that 300-to-400 physicians are lost every year to suicide in the US. This roughly equates to losing one doctor each day who has taken their own life, or between one small and one large medical school class lost to suicide each year.
Skewed statistics
Writing in Medscape in July 2022, Dr Louise B Andrew states: “A reasonable assumption is that under-reporting of suicide as the cause of death by sympathetic colleagues certifying death may well skew these statistics. Most probably, the real incidence of physician suicide is somewhat higher than the prevailing estimate.” She goes on to note that most common means of suicide by physicians in the US are lethal medication overdoses and firearms.
Most probably, the real incidence of physician suicide is somewhat higher than the prevailing estimate
In the Irish context, burnout among Irish doctors was among the most prominent topics at the IHCA Annual Conference held in Dublin earlier this month (see IHCA conference coverage pages 8 and 10).
Dr Íde Delargy, Medical Director, Practitioner Health Matters Programme (PHMP), told delegates that “the most common presentation to the [PHMP] service that we would see is one that would be termed burnout”.
“That presents in a way that the doctor is unable to sleep, is ruminating excessively, is feeling overwhelmed, stress, unable to cope,” Dr Delargy told the conference.
Speaking before the meeting, new IHCA President Prof Robert Landers said that “studies undertaken by colleagues have quantified that almost eight in every 10 consultants are screening positive for burnout”.
In 2019, the IHCA Annual Conference heard research showing that a doctor is twice as likely to die by suicide than a member of the general population. The finding was based on research by the RCPI in which the authors stated that staff shortages, inability to take annual and sick leave, and inadequate replacement cover during leave are contributing factors to this unacceptable rate of suicide. Worsening working conditions in Ireland’s acute hospital system was a significant contributing factor, leading to unsustainable levels of stress and burnout among the profession.
Nobody could reasonably argue that the Covid-19 pandemic has not worsened the problem of burnout considerably. This is also more difficult to quantify, but as with other knock-on effects of lockdowns, social isolation and increased pressure on the general population and doctors themselves, the ramifications will emerge in the years to come. Prof Daniel Shapiro, Professor of Medical Humanism at Penn State University in the US, pointed to simple screenings in the university’s College of Medicine, which indicated a rate of 10 per cent of major depression among physicians. “Now, we are seeing a 30-to-33 per cent depression rate,” he wrote in Medscape. “When patients go on ventilators, it’s often true that they don’t come off them. So physicians are witnessing terrible tragedy, which is a painful way to practice.”
Also the Medscape Physician Burnout and Depression Report 2022 provides data for the ongoing decline in physicians’ emotional and psychological wellbeing. The progression to burnout is insidious, touching almost all specialties – in the previous year’s report, 42 per cent of doctors reported being burned-out; this rose to 47 in this year’s report. Stark figures for the specialty of emergency medicine show that the rate of burnout is 60 per cent this year, compared to 43 per cent in 2021.
Other specialties in which burnout is rampant include critical care at 51 per cent; rheumatology at 50 per cent; infectious disease at 49 per cent; and urology at 49 per cent. Every year, an excess of bureaucratic tasks tops the list for the causes of burnout.
Practitioner Health Matters Programme
In Ireland, the PHMP provides anonymous, non-judgmental assessment, treatment and support for doctors, dentists and pharmacists who may be experiencing difficulties with mental health or substance misuse problems. The PHMP discretely accepts self-referrals from health professionals in difficulty and provides answers to questions and practical advice.
The PHMP Annual Report 2021 showed that there were 106 new presentations to the programme in 2021, an increase from 78 in 2020.

Speaking to the Medical Independent (MI), Dr Delargy expanded on the difficulties that doctors in Ireland may face in terms of their mental wellbeing, as well as the stigma around the topic and continuing unrealistic expectations placed on doctors. “One of the problems is that we don’t have accurate statistics [in Ireland],” said Dr Delargy. “The last survey that was done was conducted by Dr Blánaid Hayes [approximately 10 years ago] and that is the most recent study we have in terms of burnout and depression among doctors, and even that did not scan the whole of the medical profession. So we are running on estimates, we are running on studies like the Medscape report or ones done in the UK, so that is the first thing to understand in terms of having accurate figures.”
Dr Delargy acknowledged that the PHMP is seeing only a small representation of the problem amongst the profession. “We are well aware that there are a lot more people who are struggling out there who have not presented to us,” Dr Delargy told MI. “This is something we always get across about the PHMP – it’s not the kind of a programme that we want to be out there shouting about, because by its nature, it’s discrete, confidential, calm, and it’s in the background.
“But we do want every doctor, dentist and pharmacist to know that we exist,” she continued. “In fact, only recently I had somebody present to me and when I asked him how he found out about us, he said ‘you gave a talk about three years ago and I logged it in my head, and now I realise that I need your help’. That’s music to my ears, because we need every doctor to know that the PHMP exists, for if and when the time comes that they are struggling.”
Physicians’ quotes on burnout and depression
“I barely spend enough time with most patients, just running from one to the next, and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.”
“Where’s the relationship with patients that used to make this worthwhile? Everyone is in a foul mood.”
“Home is just as busy and chaotic as work; I can never relax.”
“I’m always tired, I have trouble concentrating, no time for children, more arguments with my hubby.”
“I’m grumpy and unpleasant to be around, I don’t care about anyone anymore, I don’t care about my hobbies anymore.”
“I get angry that my spouse doesn’t have a job that will adequately financially support us if I no longer want to work as a physician.”
“I’m unhappy and moody at home. I snap at my wife and kids when they mention it. Even my patients mention it.”
Source: Medscape Physician Suicide Report
Of the people who do approach the programme, some of them present with suicidal ideation. “We sometimes see people who are literally on the brink [of attempted suicide] and we give them the opportunity to talk about that,” she said. “My experience is that many of these people have what you might call a passive death wish. They have the view that ‘if a bus runs me over or if an accident happens, I’m okay with that’ because they are in such a negative place. We do occasionally see people who have a plan in place [to take their own life]. Of course, medics are in a better position to carry out that kind of plan – they know the how and where of how to do it, they have the access [to medications]… so if somebody is that unwell, they are more likely to do it, and we are of course aware of that as well.”
Tragically, there have been some suicides within the profession and there have also been suicides within the student ranks of the profession. “All suicides are a tragedy, but to see it happen to somebody so young who could perhaps have availed of support and help….
“When they come to us and have the opportunity to talk about what’s really bothering them, it can and does turn things around,” said Dr Delargy. “Thank God, so far on the programme, nobody has completed a suicide. However, we have seen some acutely unwell and highly distressed people attending the programme with suicidal ideation.”
‘Wrap-around’ support
Anybody who presents to the PHMP receives intensive “wrap-around” support, said Dr Delargy, and are linked with the programme on a daily basis in an effort to help them turn their lives around. “We are in a position to offer these services that these people might not otherwise get unless they are hospitalised. Most medics don’t want that – they don’t want to have to be admitted to hospital, so we have to offer them a service where the threshold for presentation is very low, so that they feel safe coming forward to a place where they can express their vulnerability safely. Reputational concern, reputational damage, and confidentiality are big [areas of concern for doctors]. They are concerned about who may find out if they go to a psychiatric service, for example; these are concerns for everybody, but I think this is felt more acutely by doctors,” she said.
“It makes for sad and difficult reading when you see these reports from Medscape, for example, and when you see that level of stress within their medical community, you have to ask if we are as bad as that in Ireland. There are signals to suggest that people are struggling and we should be under no illusions about that, because for every one person who comes forward to us, they say they know of X amount of people out there who are also struggling and haven’t come forward as yet. So we know these people are out there, just trying to muddle through.
“Our message is, you don’t need to struggle alone; there is help available, and that’s what we are all about.”
Dr Delargy also commented on the ‘superman/woman’ complex that still exists, whereby doctors are perceived by the general public – and sometimes themselves – as being immune to stress or illness, mental or physical. She was also asked if there was a particularly Irish trait of ‘soldiering on’ and ignoring emotional problems until they become acute. “I think we are seeing a little bit of a shift,” she told MI. “With the spread of social media amongst the younger generation, there are more opportunities and more acknowledgement that it’s okay to talk about your mental health. We see the younger cohort of medical people being able to articulate or discuss these issues – often, it starts in schools and builds-up from there,” she explained.
“With the older cohort, it is still almost a taboo subject and it goes along with the context and the attitudinal challenges, even within the medical community. That challenges how medics look upon how people struggle with mental health, because there are big attitudinal difficulties there. So even amongst ourselves, there can sometimes be a ‘if you can’t stand the heat, get out of the kitchen’ type of thing and if you are not robust or resilient enough to meet the demand, you are somehow weaker than the next person,” she continued. “That is where people become distressed – they start comparing themselves and start to think ‘I’m not as good, as robust or strong as they are’.
“People often say things tend to happen in threes, and you will almost invariably see that come true within this highly resilient population – and these people are highly resilient and perfectionist – they get one setback, and they push through. Then they get a second setback. But it’s usually when the third thing occurs, either in their personal or professional lives, that’s when the resilience suffers. That’s a generalisation, but it reflects what I am seeing on a day-to-day basis. We all have limits, and recognising when you reach that limit is important, to not let it affect your mental or physical health to the point of no return… that’s where burnout happens and people can resort to self-medication and/or suicidal ideation. You have to recognise these things at an early stage, rather than waiting until you reach the burnout phase.
“With true burnout… it’s like an elastic band that has lost its elasticity. We say, don’t wait until that happens because at that point your career is on the line. When you get to that point, it’s a big struggle to get back on track. That’s the key message: Don’t wait until you get to that point,” said Dr Delargy.
Within the HSE, the workplace health and wellbeing unit (WHWU) provides a wide range of specialist and expert advice and support to healthcare staff and managers. The unit is tasked with ensuring that all healthcare workers, including doctors, are informed and encouraged to access services that support them at each stage of their working lives with the aim of promoting and maintaining the physical, mental, and psychosocial wellbeing of HSE employees.
The WHWU oversees the employee assistance programme (EAP), which is a work-based support service that serves HSE staff, including doctors. It provides confidential counselling and brief practical psychosocial support, depending on the need.
The service, which is free of charge to all HSE employees, is provided by trained and experienced counsellors who are professionally qualified and bound by the codes of conduct of the professional bodies to which they belong.
Barriers
But both nationally, as well as internationally, how can the situation be improved? The US report highlighted a number of barriers for physicians seeking help with their mental and emotional distress, not least for organisational reasons. Two of the more important barriers to seeking help were stigma and potential professional repercussions, with one of the survey respondents commenting: “I’m afraid that if I spoke to a therapist, I’d have to report receiving psychiatric treatment to credentialling or licensing boards.”
Approximately 40 per cent of survey respondents chose not to disclose their suicidal thoughts to anyone – including a family member or suicide hotline – regardless of their age. Only 10 per cent of men and 13 per cent of women said that a colleague had discussed their suicidal thoughts with them, reinforcing the well-known culture of silence among doctors with emotional and mental health difficulties.
Physicians, by and large, tend to resort to self-help strategies when in emotional distress. Some 68 per cent cited spending time with their families as a coping strategy, with only 10 per cent saying reducing working hours or transitioning to a part-time schedule was their way of coping with the professional stress.
Gaining traction
In the US, the issue of physician suicide has recently come under the spotlight following the death by suicide of emergency department physician Dr Lorna Breen. US Congress has passed the Dr Lorna Breen Health Care Provider Protection Act, which aims to reduce and prevent suicide, burnout, and mental and behavioral health problems among healthcare professionals. The Act will help to establish grants for training healthcare students, residents, or professionals in evidence-informed strategies to reduce and prevent suicide, burnout, mental health conditions, and substance use disorders.
This is in tandem with the establishment of the Dr Lorna Breen Heroes Foundation, which seeks to: Advise the healthcare industry to implement doctor wellbeing initiatives; build awareness of these issues to reduce stigma; and fund research and programmes that will reduce healthcare professional burnout and improve provider health.
Speaking to Time magazine, Dr Breen’s brother-in-law Mr Corey Feist – CEO of a physician group at the University of Virginia, US – highlighted the institutional barriers to physicians seeking help. “I think it’s important to clarify that burnout is not a mental health condition; it’s a workplace condition,” he commented.
“We don’t need more banners about healthcare heroes, and we don’t need more free meditation apps for them. We need real solutions that work for people like Lorna. She was the canary in the coalmine for us, and for many people. We don’t need to make our canaries stronger. We need to redesign the coalmine.”
Doctors in difficulty can contact the PHMP confidentially for support and advice by calling 085 760 1274 or by emailing confidential@practitionerhealth.ie.












Leave a Reply
You must be logged in to post a comment.