







A comprehensive overview of the most prevalent STIs in Ireland, and current screening, diagnosis and treatment approaches.
Sexually transmitted infections (STIs) are a major public health concern and an increasing cause of ill-health globally. STIs are spread through intimate sexual contact, including unprotected vaginal, anal, and oral sex with an infected partner. Even protected sex can be a risk for contracting some sexually transmitted infections. STIs usually affect the genitals, anus, or mouth, but can also affect other areas of the body. Many STIs have no signs and symptoms and if left untreated have the potential to cause significant morbidity in women and men, including infertility, ectopic pregnancy, and other medical conditions, which is why STI screening is so important.
Some sexual activities pose higher risks than others, including unprotected sex with casual partners, multiple partners, or a partner who has taken risks – had unprotected sex with casual partners or with a partner who has injected drugs. Men who have unprotected anal sex with other men (MSM) are also at higher risk.
HSE public STI screening services are free in Ireland and are usually based in hospitals and special community clinic settings. Some GP practices and family planning services provide STI testing services for a fee. GPs and general practice nurses have an important role to play in both preventative and treatment services. Student health centres in third-level institutions provide an ideal opportunity to target at-risk populations for the promotion of safe sexual practices and STI screening and consultations in colleges are often free or subsidised. Well Woman Clinics and the Irish Family Planning Association (IFPA), both provide STI screening for men and women. Gay Men’s Health Service (GMHS) promotes sexual health among gay, bisexual and MSM, through counselling and STI clinical services. A community-based multidisciplinary project team of medical and support staff provide free STI clinical services to MSM and trans people.
The HSE’s Sexual Health and Crisis Pregnancy Programme (SHCPP) currently provides a free home STI testing service in partnership with online STI testing provider SH:24 to people over the age of 17 years, in 22 counties. Instructions are provided on how to complete the test kit, with support available from SH:24’s clinical team by phone or text message. Results are communicated through the SH:24 clinical team by text or phone and if follow-up testing or treatment is required this is provided for free by HSE public STI clinics. This home STI testing service is for individuals who do not have symptoms of an STI.
STI screening at a clinic takes approximately 30 minutes and involves a consultation, physical examination, urine and blood samples, and swabs. Full STI screening includes tests for chlamydia, gonorrhoea, syphilis, genital herpes, HIV, hepatitis B, and hepatitis C, and may include testing for trichomonas. Other non-sexually transmitted infections, such as candidiasis and bacterial vaginosis, are sometimes detected and can be easily treated.
Chlamydia trachomatis (CT, chlamydia) is the most commonly diagnosed bacterial STI in Ireland and most cases occur in young people under the age of 25. Often asymptomatic in both males and females, symptoms in males can include dysuria and a urethral discharge; and in women, vaginal discharge, intermenstrual bleeding, and post coital bleeding. Infection can lead to epididymitis in males and pelvic inflammatory disease (PID) in females. PID is associated with an increased risk of tubal factor infertility, ectopic pregnancy and chronic pelvic pain. Diagnosis can be made on first-void urine in males and vulvovaginal or endocervical swab (less sensitive) in females. Vulvovaginal swabs can be provider- or self-taken. In MSM, as well as first-void urine, pharyngeal and rectal sites should also be tested. Chlamydia is a notifiable disease.
Gonorrhoea (Neisseria gonorrhoeae) is the second most common bacterial STI in Ireland and is found most frequently in young people under the age of 25 and in MSM. Infection may involve the genitals, mouth, or rectum. Infected men may experience pain or burning with urination, discharge from the penis, testicular pain, and epididymitis. Symptoms in women can include vaginal discharge, intermenstrual bleeding, post coital bleeding, and PID. Rectal infection can lead to proctitis. Diagnosis can be made on first-void urine in males and vulvovaginal or endocervical swab in females. In MSM, pharyngeal and rectal sites should also be tested. Gonorrhoea is a notifiable disease.
The Nucleic Acid Amplification Test (NAATs)/PCR is the gold standard for chlamydia and gonorrhoea testing. The type of test may vary at different laboratories.
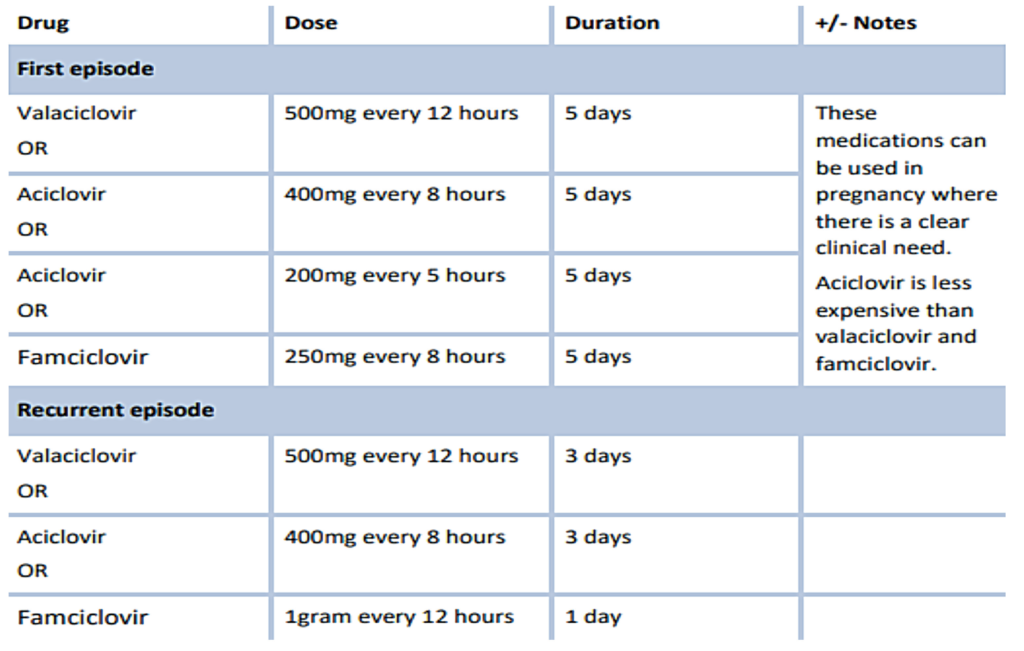
Genital herpes is a viral infection caused by the herpes simplex virus (HSV). There are two types: HSV-1 and HSV-2. Type 2 is most commonly associated with genital infection. Type 1 has also been found to cause genital infection, but is more commonly associated with oral herpes (cold sores). Genital herpes is common in Ireland and is mostly diagnosed in young women. The diagnosis can be made clinically, but should be confirmed with a HSV NAAT swab of the lesions to determine if HSV-1 or HSV- 2. Genital herpes is a notifiable disease.
Hepatitis B is a viral infection that infects the liver and is a major cause of serious liver disease, including cirrhosis and liver cancer. It affects millions of people worldwide. Hepatitis B is vaccine preventable.
Hepatitis C is a viral infection that can cause long-term liver disease such as liver cirrhosis and liver cancer. There is currently no vaccination against hepatitis C. Most cases of hepatitis C are found in people who inject drugs, however, the number of cases of sexually-transmitted hepatitis C diagnosed in MSM in Ireland has increased. Many cases have been in MSM who are also infected with HIV. Hepatitis C virus (HCV) testing should be considered part of routine sexual health screening for MSM; people living with HIV; commercial sex workers, and people who inject drugs (PWID). Partners should also be considered for HCV testing.
Trichomoniasis (TV) is an STI caused by a protozoan parasite – Trichomonas vaginalis. Most cases are found in women, and although it can affect both men and women, infection in men is uncommon. TV can infect the vagina and cervix in women and the urethra and underneath the foreskin in men. In women it usually presents with a vaginal discharge, which may be offensive with an associated vulvitis/vaginitis. Men usually present as sexual contacts of women with infection and may present with symptoms of urethritis, including dysuria and urethral discharge. TV is a notifiable disease.
Syphilis is an STI caused by a bacterium called Treponema pallidum. There were 611 cases reported in Ireland in 2020. The highest rate (2020) in males and females was in the 30-34-year age group, 75.6 per 100,000 population and 6.9 per 100,000 population, respectively. Most new cases of syphilis are among MSM. While the number of STI notifications decreased in Ireland in 2020, most likely due to the impact of the Covid-19 pandemic, early infectious syphilis (EIS) is on the increase, with a 43 per cent increase (498 cases) reported by HPSC in 2021 between 01/01/2021 and 21/08/2021, compared to the same time-period in 2020 (349 cases).
Unlike other STIs, such as chlamydia, gonorrhoea, and genital herpes simplex, cases of syphilis tend be in older age groups. The proportion of syphilis cases each year are highest in those aged 25-29 and 30-34 years, while for chlamydia the proportion of cases each year is highest in those aged 20-24 years. This trend continued in 2021, with 18 per cent of syphilis cases notified from 01/01/2021 to 21/08/2021 in those aged 25-29 years, 26 per cent of cases were aged 30-34 years, and 15 per cent of cases were aged 35-39 years, compared to 8 per cent of cases who were aged 20-24 years. Presenting symptoms of a syphilis infection depend on the phase of the infection at evaluation. Symptoms can be broken down by primary, secondary, latent, and tertiary phases. Early recognition and treatment of syphilis is critical to preventing avoidable morbidity for those infected and onward transmission to others. Safer sex practices and regular testing among at-risk groups, such as HIV-positive MSM and those with multiple partners, are key to prevention.
The screening test for syphilis is T. pallidum EIA (enzyme immunoassay), which checks for antibodies to T. pallidum. In individuals with syphilis, this test remains positive regardless of treatment or risk of reinfection. Syphilis is a notifiable disease.
Human immunodeficiency virus (HIV) is a virus that attacks the human immune system and weakens its ability to fight infection and disease. Over 6,000 people are estimated to be living with HIV in Ireland and approximately 15 per cent of people with HIV in Ireland are unaware they have the condition, because they have either not been tested or developed HIV since their last test. Approximately half of new cases of HIV in Ireland are among MSM, the other half being mostly heterosexual men and women, and PWID. HIV is diagnosed with a blood test and HIV testing is available in many healthcare settings including STI clinics, GPs, and student health clinics. Many NGOs offer HIV testing in Ireland, including rapid HIV testing in community venues; HIV self-test kits are also now available on the Irish market, both commercially and free-of-charge through https://selftest.hivireland.ie/. HIV is a notifiable disease.
HIV prevention: PrEP and PEP/PEPSE
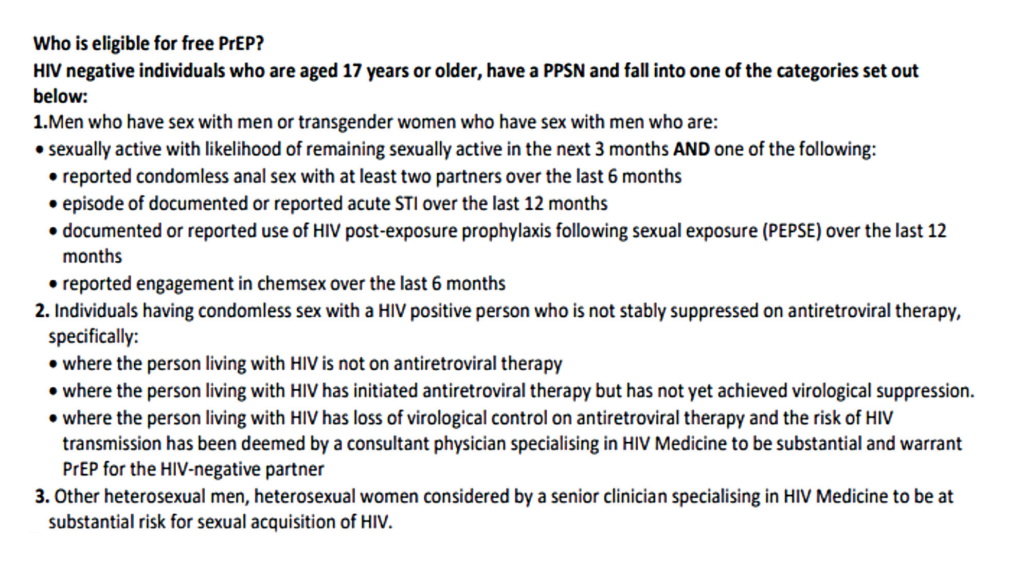
Pre-exposure prophylaxis (PrEP) is the use of oral antiretroviral therapy in HIV-negative people to reduce the risk of HIV infection. PrEP is taken by HIV-negative people prophylactically before having sex (pre-exposure) and after sex to prevent HIV. The window period for HIV is 45 days. PrEP is available free-of-charge through the HSE to people who meet the clinical eligibility criteria and who are deemed to be at substantial risk of acquiring HIV.
Post-exposure prophylaxis (PEP) is short-term antiretroviral treatment to reduce the likelihood of HIV infection after potential exposure, either occupationally or through sexual intercourse. PEP may prevent infection with HIV developing. A full course of PEP (two or three antiretroviral HIV drugs) is for 28 days (four weeks). The medication must be started within 72 hours of possible exposure to HIV infection to be effective. The term PEPSE is sometimes used and stands for PEP after Sexual Exposure.
U=U ‘undetectable’ equals ‘un-transmittable’
HIV can be treated effectively with antiretroviral medications, which stops HIV reproducing in the body. When taken properly, HIV treatment reduces the chance of a person living with HIV passing it on to someone else. When a person living with HIV is on treatment and the viral load in the body is ‘undetectable’, HIV cannot be transmitted to sexual partners. This is known as ‘undetectable’ equals ‘un-transmittable’ (U=U).
Window period
The window period can vary for different STIs, and is the time that elapses between encountering an STI, and when a false-negative result may occur. Sexual partners may have a false-negative test result in this time. Sexual partner(s) of someone with a confirmed STI in this window period should be tested and treated empirically and follow-up testing should be arranged.
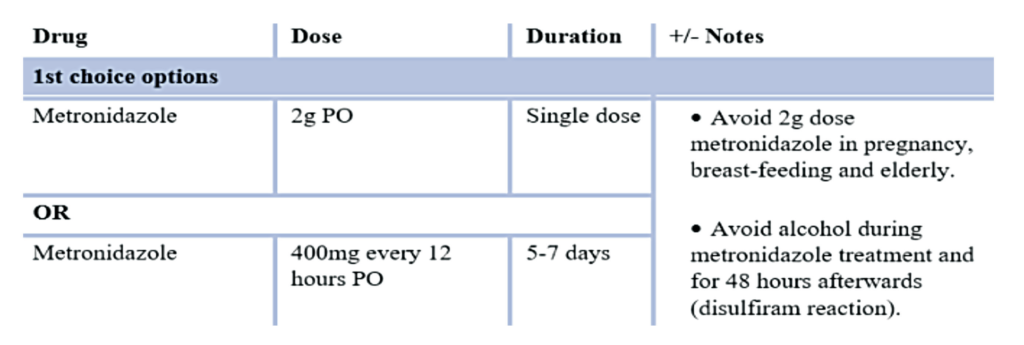
TABLE 2: Treatment of trichomoniasis (HSE guidance)
Partner notification
Partner notification is the process of providing advice, testing, and treatment to sexual contacts of an individual diagnosed with an STI. Testing and treatment of sexual partners is important to prevent reinfection and onward transmission. Partner notification is an important part of the management and control of STIs and a look-back period of three-to-six months should be considered. Patients who have been diagnosed with an STI should be encouraged to inform their sexual partners of the need for testing. For complex cases, referral to a GUM clinic should be considered.
STI screening. What happens at an STI clinic?
The clinician will start the consultation by taking a sexual health history with the patient and asking questions about the person’s symptoms, sexual and past-history, risks, and general health. If female, risk of pregnancy will be discussed (see Table 2). Personal sexual health questions are only asked for the purposes of assessing the patients’ health and to guide the provider to take the appropriate tests, depending on what risks the person has been exposed to. A physical examination will then be carried out and the type of tests depend on the patient’s symptoms. If a patient prefers a female or male provider this should be mentioned at registration and the request will be provided where possible. A chaperone can be provided if necessary and sometimes the patient may bring their own.
Males: The skin and testicles are examined for any rashes, lumps, bumps, and discharge. A swab may be taken from the penis, anus and/or throat, if required. A urine sample will be taken, and males need to hold their urine for at least two hours before testing. Blood tests will be taken for HIV, hepatitis B, and syphilis as well as any other infections the clinician considers necessary.
Females: The clinician will examine the skin and genitals for any rashes, lumps and bumps, and discharge. Vaginal swabs will be taken and sent for testing. Sometimes the vaginal swab may be taken by the patient themselves. Depending on the history, swabs may also be taken from the throat and anus. Blood tests will be taken for HIV, hepatitis B and syphilis as well as any other infections the clinician considers necessary.
Treatment
Bacterial vaginosis, vaginal candidiasis and trichomoniasis
Abnormal vaginal discharge can include STI and non-infectious causes. Three possible infections associated with abnormal vaginal discharge are bacterial vaginosis, vaginal candidiasis, and trichomoniasis.
Quick reference guide for vaginal discharge can be found at: www.antibioticprescribing.ie.
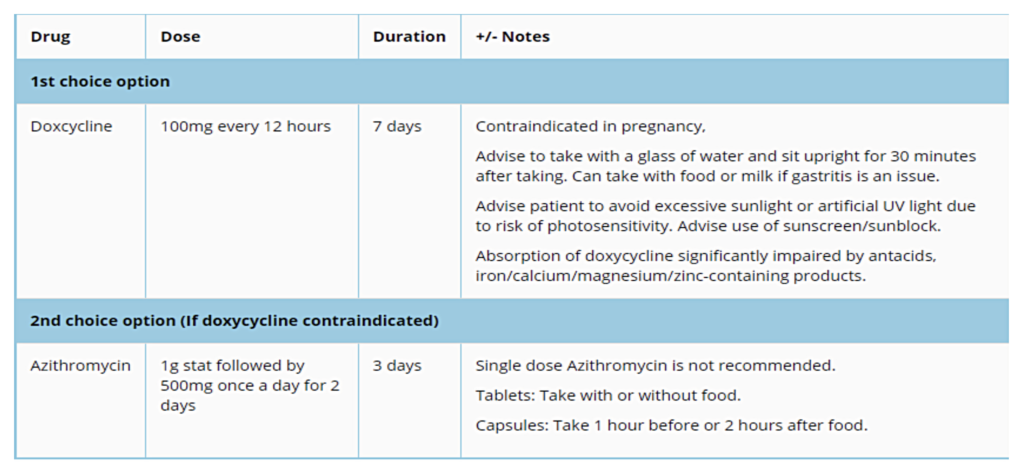
Treatment of chlamydia
Treatment of uncomplicated anogenital chlamydia: Azithromycin therapy should only be considered if doxycycline is contraindicated. Doxycycline is effective in treatment of C. trachomatis infections of urogenital, rectal, and oropharyngeal sites, whereas azithromycin is less efficacious than doxycycline in the treatment of pharyngeal and rectal chlamydia. Azithromycin therapy is also associated with macrolide resistance in Mycoplasma genitalium and high-level azithromycin resistance in gonorrhoea. If azithromycin therapy is indicated, single-dose azithromycin is not recommended and a three-day course is required. See Table 3.
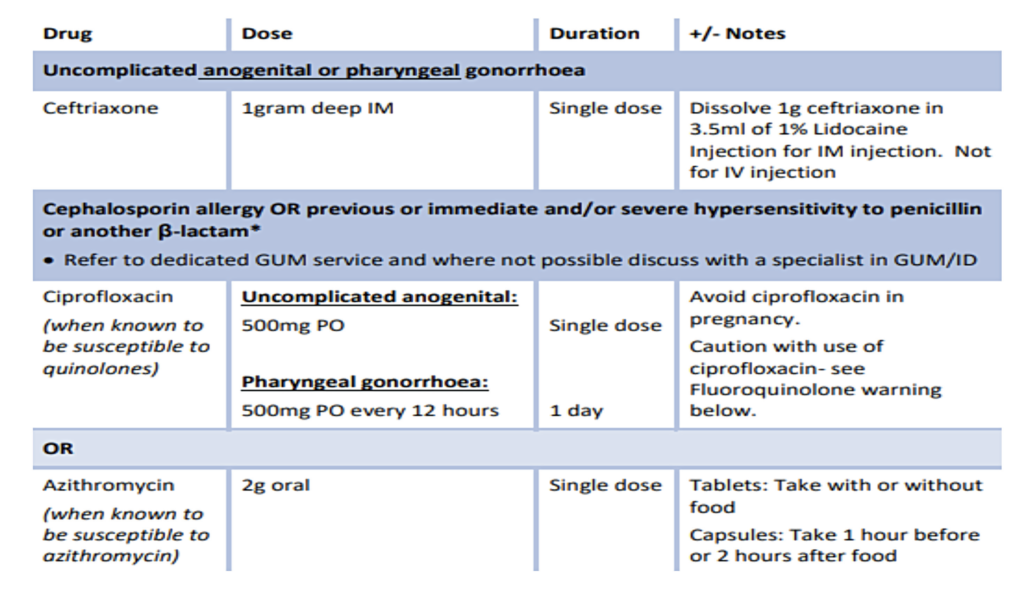
Treatment of gonorrhoea
Empiric treatment with oral cefixime is inappropriate. See Table 4.
Treatment hepatitis B
There are two main phases of hepatitis B: acute (short-term) and chronic (long-term). Approximately 90 per cent develop an acute version of hepatitis B. They can clear the virus naturally from their bodies within six months and usually develop immunity to hepatitis B for life. About 10 per cent of people do not clear HBV from their bodies naturally and go on to develop a long-term chronic infection. In some people the virus progresses quickly and can result in cirrhosis, cancer, liver failure, and even death.
Treatment is available for hepatitis B. Chronic hepatitis B infection is usually treated with alpha/pegylated interferon to help prevent further liver damage, however, not everyone can take interferon due to serious side-effects. Treatment usually lasts a number of months during which time the patient will be carefully monitored. If alpha/pegylated interferon is not suitable, antiviral medications, such as tenofovir or entecavir, will be tried instead.
Hepatitis B is a vaccine-preventable illness. PEP emergency treatment is also available within 72 hours for anyone who has been exposed to hepatitis B. PEP can prevent HBV establishing itself in the blood stream. It is available in most emergency departments and sexual health clinics.
Treatment of hepatitis C
Hepatitis C is now treated using direct-acting antiviral (DAA) medication. Two pangenotypic regimens are available on the Irish market – sofosbuvir/velpatasvir (Epclusa) and glecaprevir/pibrentasvir (Maviret). Treatment is extremely effective and consists of an eight-to-12-week course of oral tablets, although some people may need a 24-week course. Treatment is free under the National Hepatitis C Treatment Programme and cure rates exceed 95 per cent.
Treatment of syphilis
Parenteral penicillin is first-line treatment for syphilis and the dose, duration, and route (IV versus IM) is determined by the clinical circumstances. Oral doxycycline is the second-line option – the dose and duration are determined by the clinical circumstances. Decisions around treatment should be made by a clinician with expertise and experience in managing syphilis. Patients with newly-diagnosed syphilis should be referred to a GUM clinic for further management and treatment.
Treatment of HIV
There is no cure for HIV, but the current treatment options (HAART, highly active anti-retroviral therapy), mean people with HIV can live a normal lifespan. There are more than 30 antiretroviral medications in six drug classes. Each class of drug attacks HIV in a different way. Most people start HIV treatment on two drugs from the nucleoside/nucleotide reverse transcriptase inhibitors class combined with either one integrase inhibitor, one non-nucleoside reverse transcriptase inhibitor, or one protease inhibitor – hence the name, ‘triple therapy’.
It is important that people infected with HIV adhere to the treatment schedule, as HIV can become resistant to the medication if it is not taken properly. People living with HIV who have an undetectable viral load and take their HIV medications properly, will not pass on HIV to sexual partners.
Current situation and outlook
More than one million STIs occur worldwide every day. The economic and social cost of STIs places a large strain on healthcare systems. Adolescents, young adults, and MSM are disproportionately affected by STIs, and at high-risk due to behavioural, biological, social, and cultural factors.
The timeliness of treatment for STIs can have consequences for the individual and increase the likelihood of infecting others. Given the high burden of STIs and the risk of medical complications associated with these infections, screening, accurate diagnosis, and timely and appropriate treatment are critical. The testing and treatment of sexual partners is important in preventing the spread of STIs, decreasing the rate of reinfection, and preventing medical complications of asymptomatic infections.
Aside from the pandemic-related infectious disease drop, the continuing rise in STIs annually in Ireland is a worrying trend. The key message from the HSE HPSC is for people to get tested regularly and reduce their risks through using condoms for vaginal, oral and anal sex, and being mindful of other risks. People should get tested for STIs if they have symptoms of an STI, change their sexual partner, have multiple or overlapping partners, or their partner has an STI.
Stigma causes many people to avoid seeking STI-related services because of negative experiences such as discrimination, indifference, and overt hostility in healthcare settings. In addition to effective public health infrastructures and the technologies needed for diagnosis and treatment, global STI prevention and control efforts require renewed commitment to systematic programmatic approaches to prevent or reduce STI-related stigma.
The HSE has a number of dedicated programmes and strategies to improving sexual health activities and services. Sexual health is an essential component of overall health. Effective STI prevention and control emerges from a holistic, sexual health perspective involving many levels of society and a variety of approaches. An integrated approach is required that involves taking action throughout the entire population and at all levels of the prevention and care continua. Further advancement in technology, specifically the development of rapid, sensitive and specific point-of-care testing, will provide additional tools for STI diagnosis and control. These actions can lead to better prevention, screening, and treatment.
TTheresa Lowry-Lehnen, RGN, GPN, RNP, BSc, MSc, M. Ed, PhD, Clinical Nurse Specialist and Associate Lecturer, South East Technological University (SETU).











Leave a Reply
You must be logged in to post a comment.