NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Theresa Lowry-Lehnen, CNS, GPN, RNP, PhD, National PRO of the IGPNEA
- 25th May 2021
Male doctors and patients, sexual problems are discussing the symptoms and treatment methods.
Prostate cancer is one of the most common, but also most successfully treated cancers in men
Prostate cancer is the second most frequent cancer diagnosed in men and the fifth leading cause of death globally. Excluding non-melanoma skin cancer, prostate cancer is the leading cause of cancer in men internationally. In 2018, 1,276,106 new cases of prostate cancer were registered worldwide, representing 7.1 per cent of all cancers in men and 358,989 deaths representing 3.8 per cent of all male cancer deaths. Approximately 3,890 men are diagnosed with prostate cancer each year in Ireland, indicating that one-in-seven men in Ireland will be diagnosed with prostate cancer during their lifetime (Irish Cancer Society 2021, and National Cancer Registry Ireland (NCRI)).
It accounts for 30 per cent of all newly-diagnosed cancers in Irish males and 11 per cent of all invasive cancers in Ireland (NCRI). Prostate cancer incidence rates are highly variable worldwide, which is likely to be attributed to different prostate-specific antigen (PSA) testing rates. In Europe, prostate cancer is the most frequently diagnosed cancer among men, accounting for 24 per cent of all new cancers in 2018, with around 450,000 new prostate cancer cases detected in 2018.
Risk factors
The most common risk factor for prostate cancer is increasing age. While one-in-350 men under the age of 50 years will be diagnosed with prostate cancer, the incidence rate increases to one in every 52 men for those aged 50-to-59 years. Prostate cancer most commonly affects men over the age of 50 and almost two in every three prostate cancers are diagnosed in men over the age of 65 years. In Ireland, the majority of cases are detected in men aged 65-to-84 years, with 37 per cent of cases detected in men under 65 years of age.
Genetic factors play a role. Family history is associated with an increased risk and men with a father or brother diagnosed with prostate cancer at age 50 years have an approximately two-fold increased risk of prostate cancer. Risk is higher in males with a relative who developed prostate cancer at a younger age and in males who have more than one relative with the disease. Two breast cancer genes, BRCA1 and BRCA2, have been linked to prostate cancer. Like women, men can have mutations in the BRCA1 and BRCA2 genes. Men carrying mutations in BRCA2 genes have an increased risk of developing prostate cancer, and mutations in either gene can significantly reduce survival. Studies have also revealed an association between hereditary susceptibility to prostate cancer and sequence variations in the RNASEL gene (ribonuclease L), which plays a role in maintaining immunity against viral infections.
A common RNASEL variant involves a mutation resulting in decreased activity of the encoded ribonuclease L protein, reducing the immune defence against viruses. Men who inherit this mutation have a significantly increased risk of developing prostate cancer. It is estimated that about 20 per cent of patients with prostate cancer report a family history, which may develop not only because of shared genes, but also for a similar pattern of exposure to certain environmental carcinogens and common lifestyle habits. Afro-Caribbean men have the highest incidence of prostate cancer of any group (231.9 per 100,000) while Asian men have the lowest risk.
Obesity and physical inactivity have been associated with higher-grade prostate cancers and studies have shown increased risk associated with various dietary intakes, including high levels of high-saturated fats and red meats, and reduced intake of fish, fruit, and vegetables. Research is ongoing into the links between diet and prostate cancer and there is some evidence that a diet high in calcium is also linked to an increased risk of developing prostate cancer.
Although there are no studies that can sufficiently demonstrate the direct correlation between diet and nutrition with risk or prevention of prostate cancer development, many preclinical studies that looked at links between certain eating behaviours and cancer suggest there may be a connection.
Symptoms
When the prostate gland becomes cancerous, it can put pressure on the urethra, causing dysuria, a burning sensation and frequency of micturition. It can also cause hesitancy, a weak and intermittent flow, nocturia, haematuria and impotence or sexual dysfunction. Other symptoms include swollen lymph nodes in the groin and pain in the pelvis, hips, back, or ribs. More advanced stages of the disease may present with urinary retention and back pain, as the axis skeleton is the most common site of bony metastatic disease. Prostate cancer should not be confused with benign prostate hyperplasia (BPH), which has similar symptoms and often occurs in older men.
Diagnosis
Prostate cancers usually grow very slowly, and symptoms may not occur for some time. If the prostate is enlarged, a preliminary diagnosis can be made by rectal examination or transrectal ultrasound (TRUS). A PSA blood test is used to detect prostate tumours in their earliest stages in high-risk individuals. Although originally introduced as a tumour marker for the detection of cancer recurrence, PSA testing became widely adopted as a screening tool for prostate cancer. However, it is not prostate cancer-specific and other prostate conditions, such as BPH or prostatitis, can also affect PSA levels. If prostate cancer is suspected a biopsy is done to confirm the diagnosis. When detected early, prostate cancer is very treatable. A large majority of prostate cancers are diagnosed either before they have spread or when they have spread only locally. Survival rates in these cases are very high.
Staging
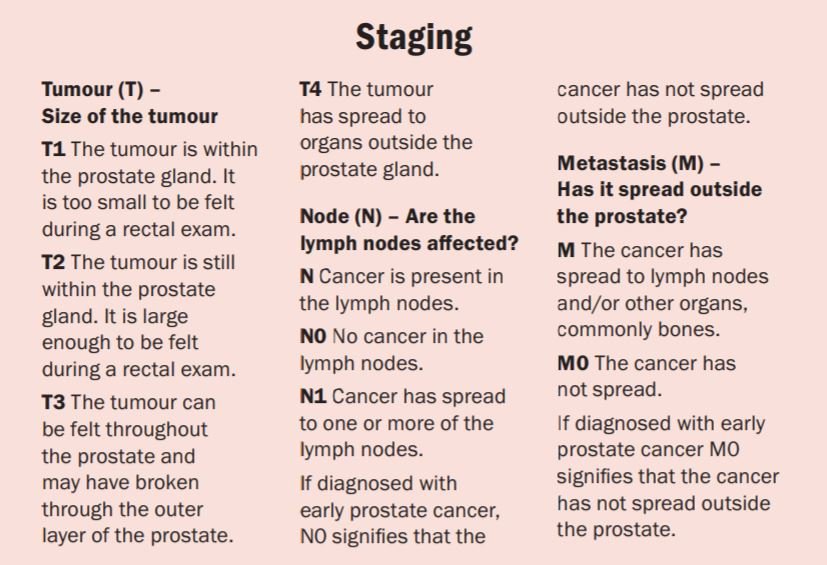
The TNM staging system refers to the size of the tumour (T), if the cancer has spread to the lymph nodes (N), and if the cancer has spread to other parts of the body – metastasis (M) (Figure 1)
Figure 1: TNM prostate cancer staging score
The Gleason Score
The Gleason Score is a grading system used to determine the aggressiveness of prostate cancer and can be used to choose appropriate treatment options. The Gleason Score ranges from 1-5 and describes how much the cancer looks like healthy or abnormal tissue. Most cancers score a grade 3 or higher. Since prostate tumours are often made up of cancerous cells that have different grades, two grades are assigned for each patient. A primary grade is given to describe the cells that make up the largest area of the tumour and a secondary grade is given to describe the cells of the next largest area. If the Gleason Score is written as 3+4=7, it means most of the tumour is grade 3 and the next largest section of the tumour is grade 4. If the cancer is almost entirely made up of cells with the same score, the grade for that area is counted twice to calculate the total Gleason Score.
Prostate cancer has one of the highest survival rates of any type of cancer: 92 per cent of all prostate cancers are found when they are in the early stage and almost 100 per cent of men who have local or regional prostate cancer will survive more than five years after diagnosis
Typical Gleason Scores range from 6-10. The higher the Gleason Score, the more likely that the cancer will grow and spread quickly. Scores of 6 or less describe cancer cells that look similar to normal cells and suggest that the cancer is likely to grow slowly. A score of 7 suggests an intermediate risk for aggressive cancer. Scoring a 7 means that the largest section of the tumour (primary score) scored a 3 or 4. Tumours with a primary score of 3 and a secondary score of 4 have a reasonably good outlook, whereas cancers with a primary Gleason Score of 4 and a secondary score of 3, are more likely to grow and spread. Scores of 8 or higher describe cancers that are likely to spread more rapidly, often referred to as high grade or poorly differentiated.
Treatment
Treatment options for patients with prostate cancer depend on the stage and grade of the cancer and include active surveillance, watchful waiting, hormone therapy, radical prostatectomy, external beam radiotherapy, and brachytherapy. Active surveillance involves a PSA blood test every three months and a digital rectal exam (DRE) every six months for the first year, followed by a PSA blood test every six months and a DRE at least once a year. Prostate biopsies and imaging tests may also be done every one-to-three years. Because prostate cancers usually progress slowly, a ‘watchful waiting’ approach rather than immediate treatment may be recommended.
This is especially true for patients who are elderly or in otherwise poor health. In patients with intermediate or high-risk localised prostate cancer with a real prospect of long-term disease control and those with locally-advanced disease, radical prostatectomy or radical radiotherapy should be offered.
Hormone therapy is the primary treatment for metastatic prostate cancer, but is also used for patients with locally-advanced, non-metastatic disease. In patients with localised prostate cancer, the choice of treatment depends on whether the disease is low, intermediate, or high risk. Hormone therapy (androgen suppression or androgen deprivation therapy (ADT)) attacks androgens that stimulate the growth of prostate cancer. A form of hormone therapy involves LHRH analogs or LHRH agonists, such as buserelin, goserelin, leuprorelin acetate or triptorelin that chemically block the production of androgens. Side-effects of hormone therapy include reduced libido, sexual dysfunction, osteoporosis, gynaecomastia and hot flushes.
Brachytherapy is a form of radiation therapy used to treat prostate cancer. Prostate brachytherapy procedures vary based on the type. High-dose rate (HDR) brachytherapy is a temporary type of prostate brachytherapy that involves placing radioactive sources in the prostate gland and delivering a high dose of radiation over a few minutes before the sources are removed. Treatment may involve several sessions.
Low-dose rate (LDR) brachytherapy is permanent and involves placing radioactive seeds in the prostate gland permanently, where they slowly release radiation over several months. Brachytherapy may be the only treatment used for early-stage prostate cancer that is less likely to spread beyond the prostate. For larger prostate cancers or those that have a greater chance of spreading beyond the prostate, brachytherapy may be used along with other treatments, such as external beam radiation therapy (EBRT) or hormone therapy.
EBRT can be used to try to cure earlier stage cancers, or to help relieve symptoms, such as bone pain if the cancer has spread to a specific area of bone. Surgery is usually only carried out if the cancer has not spread from the prostate. A radical prostatectomy may be considered if examination of the pelvic lymph nodes reveals that they are not cancerous. Surgical risks can include impotence and urinary incontinence. TURP can be used to relieve symptoms, but does not remove all of the cancer. TURP is often used in men who cannot have a radical prostatectomy because of advanced age or illness or in men who have a non-cancerous enlargement of the prostate. In men who are unable to have traditional surgery, cryosurgery may also be used.
If the cancer has spread from the prostate, radiation therapy may be used. Bi lateral orchidectomy should be offered to all patients with metastatic prostate cancer as an alternative to continuous LHRH agonist treatment. If surgery or hormone therapy fails, chemotherapy may be used. While chemotherapy can slow the growth of the tumour, it is not very effective in treating prostate cancer.
Prognosis and outlook
The outlook for prostate cancer is generally good because, unlike many other types of cancer, it usually progresses very slowly. If treated early, prostate cancer can often be cured. The survival rate is over 90 per cent and many men die with prostate cancer, rather than as a result of having it. Prostate cancer has one of the highest survival rates of any type of cancer: 92 per cent of all prostate cancers are found when they are in the early stages and almost 100 per cent of men who have local or regional prostate cancer will survive more than five years after diagnosis.
For most with local or regional prostate cancer, the relative 10-year survival rate is 98 per cent and the relative 15-year survival rate is 96 per cent. Once prostate cancer has spread beyond the prostate, however, survival rates fall and about 7 per cent have more advanced prostate cancer at the time of diagnosis. For men with prostate cancer that has spread to other parts of the body, the five-year survival rate is 30 per cent.
In summary
Prostate cancer presents a number of challenges for primary care clinicians. Many men with prostate cancer are asymptomatic until the tumour has progressed and common symptoms have significant crossover with benign conditions affecting the prostate. PSA-based testing of prostate cancer is very common but remains controversial. The value of screening remains uncertain because the PSA test does not distinguish between benign and malignant disease and there has been no proof that early treatment leads to increased cure rates. DRE alone is insufficient for screening as its positive predictive value is only 11-to-26 per cent.
Current diagnostic tests have limitations in terms of significant false positive and false negative rates, however, research is ongoing into improved methods for diagnosing prostate cancer. Understanding the underlying causes of prostate cancer, including genetics and pathogenesis, has improved substantially in recent years. Nanotechnology has shown initial success in prostate cancer disease diagnosis, imaging and treatment.
A number of new tests and testing strategies are being trialled to improve the diagnosis of clinically significant prostate cancer and blood-based biomarkers for prostate cancer are also being extensively investigated. Because the value of PSA-based testing of prostate cancer remains unclear, more genetic testing–based detection strategies are needed to identify individuals at high risk of prostate cancer and novel drugs need to be evaluated to substantially improve the clinical care of patients with prostate cancer.
Continued clinical and translational research in prostate cancer is important and key to the future treatment and management of prostate cancer through leading improvements in prostate cancer imaging and diagnosis.












Leave a Reply
You must be logged in to post a comment.