NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Post-herpetic neuralgia: Diagnosis and management options
By
Prof Dominic A Hegarty
- 17th Dec 2023
Herpes zoster (HZ) is a relatively common disease; the estimated incidence of acute herpes infection in the European population varies from 1.2 to 5.2 per 1,000 people per year. There is a correlation between the incidence of the disease and age. People younger than 50 years have a low risk of developing HZ, which equals approximately 2 per cent. The incidence sharply rises in adults aged above 50 years; the risk makes up to at least 20 per cent and continues to increase further, reaching 35 per cent in people above 80 years.
The recent upswing in chickenpox infection and varicella-zoster virus (VZV) in the community has increased the risk of developing post-herpetic neuralgia (PHN). PHN is an extremely painful condition that can persist for many years, making life miserable for the unfortunate patient. Early recognition is very important and can offset chronicity. For those who are not so lucky, there are advanced options to help manage the pain.
Epidemiology
In the acute phase of inflammation, VZV reaches the sensory nervous system and remains latent in trigeminal or dorsal root ganglions (DRG) for a long period of time. Reactivation of VZV happens with advancing age, or immunosuppression can lead to the development of acute HZ. PHN occurs in a subset of the population suffering from an episode of acute HZ. Well-established risk factors for an acute HZ episode progressing to PHN include age, severe immunosuppression, the presence of a prodromal phase, severe pain during the zoster outbreak, allodynia, ophthalmic involvement, and diabetes mellitus.
A meta-analysis of the risk factors for the development of PHN, published in 2016, noted that approximately 13 per cent of patients ≥50 years of age with HZ would develop PHN. The association between increasing age and PHN is significant. According to some studies, at age 60, around 60 per cent of patients with HZ (shingles) develop PHN, and at age 70, this percentage rises to 75 per cent.
One month after the onset of HZ, 9-to-14.3 per cent of patients develop PHN, and at three months, this percentage becomes 5 per cent. At one year, 3 per cent of patients continue to have severe pain.
Family history has also been considered a risk factor for HZ. In a case-control study by Hicks et al, comprising 504 patients and 523 controls, it was observed that the blood relatives of patients were more likely to have HZ than the control group (39 per cent vs 11 per cent, p<.001). Moreover, this risk was more significant in patients with multiple blood relatives having HZ than those with a single blood relative having HZ. There is no sex predilection for PHN.
Covid-19 and PHN
In a retrospective cohort study of over two million people, it was highlighted that adults over 50 years of age who had mild Covid-19 were 15 per cent more likely to develop HZ within six months compared to those who had not been infected by coronavirus. The risk was 21 per cent greater in older people who were hospitalised with Covid-19 (Bhavsar et al. Open Forum Infectious Diseases).
Predictors
The predictors of PHN development include advanced age, acute pain, severe rash, prodromal pain, presence of the virus in peripheral blood, and adverse psychosocial factors. The associated pain with concomitant allodynia is traditionally attributed to the decrease in the activation threshold of pain-associated neuron clusters. Recently, some researchers have shown that TRVP1 receptor activation may also be implicated. This receptor may be a promising target for future analgesic drug development.
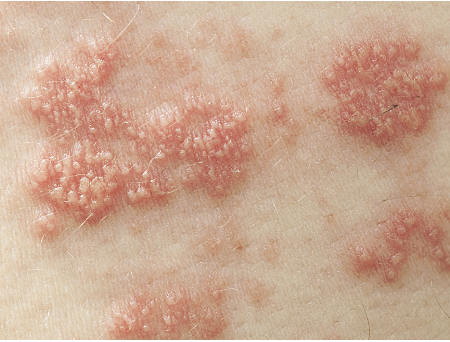
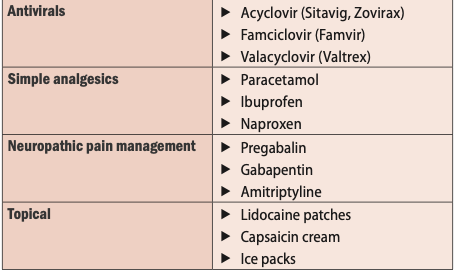
Figure 1: Herpes zoster acute blister formation Table 1: Suggested agents to consider in the early management plan
Pathophysiology
The exact physiology that separates a self-limited HZ outbreak from PHN is not fully understood. Histological examinations of relevant peripheral and central nervous tissue from sufferers of PHN reveal myelin and axon deficiency and atrophy of the dorsal horn in certain instances.
One study compared the difference in epidermal axon densities between patients who suffered from PHN and those who had a self-limited occurrence of HZ. Those afflicted with PHN had, in most instances, far fewer axons in the relevant dermatomes than non-sufferers. Therefore, an anatomical derangement is likely at least partially responsible for the development of PHN. Some suggest that an unchecked inflammatory response at the neuronal level is the main culprit of the eventual development of PHN, specifically via the reduction of centrally-mediated inhibition of nociceptive input and the promotion of peripheral sensitisation via damaged nociceptors.
The DRG suffers the most damage during PHN. Firstly, the reactivated VZV in the DRG proliferates and destroys axons, causing demyelination and ion channel dysfunction. The damaged sensory nerves can generate abnormal electrical impulses that are transmitted to the spinal cord, transmitting pain and pain hypersensitivity. A significant number of inflammatory cells are shown to be invading into the DRG of patients with PHN. Then, the inflammatory mediators that follow promote increased pain pathway activity and cause central sensitisation.
Diagnosis
The diagnosis of PHN is relatively straightforward and not one of exclusion. An episode of HZ is a prerequisite for PHN. Therefore, a history of rash with blisters in a dermatomal pattern would be expected. Rarely the characteristic rash will not be found. Persistent (more than or equal to three months) lancinating/burning pain, allodynia, paraesthesia, pruritus, dysesthesia, and/or hyperalgesia at or near the area of the rash is characteristic of PHN.
HZ can reactivate sub-clinically with no rash. This condition is called zoster sine herpete and is more complicated. It affects the central nervous system at multiple levels and causes cranial neuropathies, myelitis, polyneuritis or aseptic meningitis.
Physical examination of a patient with PHN may reveal the following:
Evidence of cutaneous scarring on an area of previous HZ.
Altered sensation in the affected areas, either hypersensitivity or hypoesthesia.
Pain is produced by non-noxious stimuli, such as a light touch, known as allodynia.
Autonomic dysfunction, such as excessive sweating over the involved area.
Investigations
PHN is almost universally diagnosed based on the history and physical examination. However, laboratory tests and some targeted imaging may provide a degree of utility. These are of greater value in atypical presentations of PHN, such as zoster sine herpete or HZ of the larynx. Serological testing for VZV IgG and IgM titres is possible, although the sensitivity and specificity are less than ideal. A four-fold rise has been used to diagnose subclinical HZ (zoster sine herpete). However, this rising titre may or may not be secondary to viral exposure or reactivation. Comparatively, immunofluorescence of vesicle scrapings detects VZV antigens in a highly specific and sensitive manner. Similarly, PCR is exquisitely sensitive for the detection of VZV DNA.
Results of cerebrospinal fluid (CSF) analysis are abnormal in 61 per cent of patients. Pleocytosis, elevated protein, and VZV DNA are usually seen. Viral culture or immunofluorescent staining helps distinguish herpes simplex from HZ.
Small-scale studies suggest that MRI may hold promise for diagnosing challenging PHN cases and differentiating between PHN and HZ. A study by Haanpaa et al reported that MRI revealed lesions attributable to HZ in the cervical cord and the brain stem in nine patients (56 per cent). At three months after the onset of HZ, PHN developed in five patients (56 per cent) who had an abnormal MRI. On MRI, seven patients with no HZ lesions did not develop residual pain.
Management options
Three fundamental treatment approaches may be considered for post-herpetic neuralgia.
1) Prevention
This focuses on identifying populations at risk for contracting HZ and administering a vaccine. At present, there are two licenced HZ vaccines in Ireland (MIMS May 2023) – Shingrix and Zostavax. Vaccination should be considered in those over 50 years and in those in the higher-risk groups. It is not necessary to determine whether patients have a history of varicella or zoster prior to vaccination because weaning antibodies in those previously exposed may lead to negative results despite past infection. A large (n =38,000) double-blind study published in the NEJM in 2005 showed that vaccination in the elderly reduced the incidence of HZ by 51 per cent and PHN by 66 per cent. Moreover, even among those who developed PHN, the burden of illness was reduced by approximately 61 per cent. It must be noted that the immune-boosting effect of the vaccination is not long-lasting, and interval re-vaccination is necessary to maintain its efficacy. Unfortunately, these vaccines are not part of the HSE’s national immunisation programme so patients need to discuss this option with their GP and self-fund the vaccine.
2) Early recognition
Early recognition and treatment of an acute HZ infection may reduce the chance of developing PHN. The benefit of rapid treatment has been shown to be very useful. If a combination of agents can be commenced with 72 hours of first symptoms, this will lower the chance of compilations.
3) PHN management
In the situation where PHN develops, the symptom management of PHN is best considered using multimodal medication regimens and interventional procedures. The evidence regarding the efficacy of these methods is mixed, but rapidly evolving and certain approaches appear to be more successful than others.
Complete resolution of the symptoms is rare. A 2014 study concluded that less than half of patients with PHN achieve significant symptom reduction. The age of the patient population increases the side-effect risk profiles of interventions. Relevant studies comparing treatments and their outcomes are often suboptimally designed.
There is no one superior treatment regimen; however, expert consensus suggests that multimodal therapy is likely the best approach.
Lastly, many of the advocated approaches treat chronic neuropathic pain in general and are not specific to PHN.
a) Traditional non-invasive treatments include oral and topical medications. The American Academy of Neurology (AAN), Special Interest Group on Neuropathic Pain (NeuPSIG), and European Federation of Neurological Societies (EFNS) all recommend an oral tricyclic antidepressant (TCA), pregabalin, and the lidocaine 5 per cent patch as first-line therapies. The anticholinergic, antihistaminergic, and alpha receptor-blocking side-effects of TCAs must be considered, as the elderly are more susceptible. As a result, it is commonplace to initially prescribe and titrate a gabapentinoid, keeping in mind that patients with reduced renal function should be started at a lower dose and up-titrated more slowly.
b) The use of opioids to combat PHN is controversial because of the changing landscape regarding what constitutes appropriate use, and also renewed governmental interest in their administration given the epidemic of abuse, addiction, and mortality. The above three medical societies recommend opioids as either first- or second-line treatments, which underscores the pain-reducing capability of this medication class.
c) Lidocaine patches
Multiple studies have confirmed the short- and long-term efficacy of the lidocaine 5 per cent patch. This patch also has the additional benefit of a small side-effect profile that is mostly limited to application site reactions. Application is required for 12 hours at a time and should be used over a prolonged period (four-to-eight weeks initially).
d) Capsaicin
Capsaicin preparations in the patch and cream formulations are also available, but are not as well-studied as the lidocaine patch. The leading cause of discontinuing capsaicin treatment is pain and irritation at the application site, suffered by almost all users in proportion to the capsaicin concentration. The cream has a low concentration of capsaicin, requiring multiple applications to achieve a therapeutic effect throughout the day. Conversely, the capsaicin patch is available in an 8 per cent formulation, delivering a therapeutic dose in just one application. The higher concentration patch should only be provided by those trained in the application and monitoring of outcome. Nevertheless, encouraging case reports and other literature suggest the intervention warrants consideration and further study.
e) Non-TCA antidepressants and NMDA antagonists
There is limited evidence to support their usefulness. For example, larger studies involving serotonin-norepinephrine reuptake inhibitors (SNRIs) and selective serotonin reuptake inhibitors (SSRIs) have not shown better outcomes than TCAs, and both classes possess a concerning side-effect profile, though typically less severe than TCAs.
The use of ketamine infusions and related studies for treating a wide range of ailments, from neuropathic pain to depression, has also resulted in renewed interest in the role of NMDA antagonism in treating PHN. There are anecdotal reports that ketamine may prove beneficial, and a few small studies support this finding, but long-term data and large-scale studies are non-existent.
Lidocaine infusions have also been considered. One double-blind study in 1999 showed that an intravenous lidocaine infusion provided clinically significant short-term pain reduction in patients with PHN. In general, small studies and case reports have established that novel therapies may be useful in certain PHN sufferers when combined with other adjuncts. The pathophysiology of PHN is complex, and sometimes an individualised non-traditional approach may prove beneficial for a particular patient.
f) Invasive therapies
Often when an individual presents to a chronic pain clinic they will have tried a number of agents, so interventional options need to be considered. If the pain persists in a specific dermatomal or nerve distribution, then a simple effective option is to use a peripheral nerve block or pulsed denervation of the DRG.
Pulsed radiofrequency (PRF) is a minimally-invasive technique that applies pulsed current (300-500kHz) to the target nerve. The current is delivered in a pulse of 20ms (45V voltage) followed by a silent period of 480ms to avoid heat lesions. Recent studies have confirmed the beneficial effects of PRF against post-operative pain, peripheral neuropathic pain, and PHN. The thoracic nerves (T1-12) are the most commonly affected by PHN, with an incidence of up to 50 per cent of cases. Studies have shown that treating both the DRG and intercoastal nerve with PRF is effective in the management of thoracic PHN. Targeting the DRG has shown to have a better outcome in pain intensity and other quality-of-life domains (SF-36).
Other invasive therapies including botulinum toxin injections, sympathetic blockade with local anaesthetics, and epidural/intrathecal injections have a limited side-effect profile. However, more studies need to be conducted to evaluate their efficacy. The other invasive therapies mentioned carry the potential for significant peri-procedural risk and/or side-effects.
g) Future therapy options
Neuromodulation offers the possibility of long-term drug-free pain therapy in a wide range of neuropathic pain conditions. The development of the DRG stimulator to treat focal dermatomal neuropathic pain conditions is theoretically promising for PHN. Traditional spinal cord stimulation programming options can now target the painful area with greater accuracy. We need to extend studies to consider the role of technology to advance our options.
Long-term enhancement of healthcare team outcomes
Considering that PHN is difficult to treat and outcomes are variable, prevention is of paramount importance. Therefore, primary care physicians and geriatricians are tasked with administering vaccinations to at-risk populations. The ever-growing ageing population means that demands on this service will continue to increase. Inclusion of the shingles vaccines on the national immunisation programme by the Department of Health needs to be considered as a priority if we are to protect our venerable senior citizens. When preventative measures fail or are never instituted, experts in the field of pain management who have experience with the condition and multimodal treatment techniques should be consulted. Interventional pain management can offer solutions. An interprofessional approach to managing patients with PHN is the best way forward.
References
Isagulyan E, Tkachenko V, Asriyants S, et al. The effectiveness of various types of electrical stimulation of the spinal cord for chronic pain in patients with post-herpetic neuralgia: A literature review. Pain Res Manag. 2023 Mar 24;2023:6015680
Huang X, Ma Y, Wang W, et al. Efficacy and safety of pulsed radiofrequency modulation of thoracic dorsal root ganglion or intercostal nerve on post-herpetic neuralgia in aged patients: A retrospective study. BMC Neurol. 2021 Jun 24;21(1):233
Forstenpointner J, Rice ASC, Finnerup NB, Baron R. Up-date on clinical management of post-herpetic neuralgia and mechanism-based treatment: New options in therapy. J Infect Dis. 2018 Sep 22;218(suppl_2):S120-S126
Lu WH, Lin CW, Wang CY, et al. Epidemiology and long-term disease burden of herpes zoster and postherpetic neuralgia in Taiwan: A population-based, propensity score-matched cohort study. BMC Public Health. 2018 Mar 20;18(1):369
Gabutti G, Valente N, Kuhdari P, et al. Prevention of herpes zoster and its complications: From the clinic to the real-life experience with the vaccine. J Med Microbiol. 2016 Dec;65(12):1363-1369
Zorzoli E, Pica F, Masetti G, et al. Herpes zoster in frail elderly patients: Prevalence, impact, management, and preventive strategies. Aging Clin Exp Res. 2018 Jul;30(7):693-702
Schutzer-Weissmann J, Farquhar-Smith P. Post-herpetic neuralgia – a review of current management and future directions. Expert Opin Pharmacother. 2017 Nov;18(16):1739-1750
Delaney A, Colvin LA, Fallon MT, et al. Postherpetic neuralgia: From preclinical models to the clinic. Neurotherapeutics. 2009 Oct;6(4):630-7
Hicks LD, Cook-Norris RH, Mendoza N, et al. Family history as a risk factor for herpes zoster: A case-control study. Arch Dermatol. 2008 May;144(5):603-8
Helgason S, Petursson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a first episode of herpes zoster: Prospective study with long-term follow-up. BMJ. 2000 Sep 30;321(7264):794-6
Chen F, Chen F, Shang Z, et al. White matter microstructure degenerates in patients with post-herpetic neuralgia. Neurosci Lett. 2017 Aug 24;656:152-157
Watson CPN, Deck JH, Morshead C, et al. Post-herpetic neuralgia: Further post-mortem studies of cases with and without pain. Pain. 1991 Feb;44(2):105-117
Werner RN, Nikkels AF, Marinović B, et al. European consensus-based (S2k) guideline on the management of herpes zoster – guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 1: Diagnosis. J Eur Acad Dermatol Venereol. 2017 Jan;31(1):9-19
Koshy E, Mengting L, Kumar H, Jianbo W. Epidemiology, treatment and prevention of herpes zoster: A comprehensive review. Indian J Dermatol Venereol Leprol. 2018 May-Jun;84(3):251-262
Gilden D, Nagel MA, Mahalingam R, et al. Clinical and molecular aspects of varicella zoster virus infection. Future Neurol. 2009 Jan 01;4(1):103-117
Spiegel R, Miron D, Lumelsky D, Horovitz Y. Severe meningoencephalitis due to late reactivation of Varicella-Zoster virus in an immunocompetent child. J Child Neurol. 2010 Jan;25(1):87-90
Harbecke R, Oxman MN, Arnold BA, et al. Shingles prevention study group. A real-time PCR assay to identify and discriminate among wild-type and vaccine strains of varicella-zoster virus and herpes simplex virus in clinical specimens, and comparison with the clinical diagnoses. J Med Virol. 2009 Jul;81(7):1310-22
Haanpää M, Dastidar P, Weinberg A, et al. CSF and MRI findings in patients with acute herpes zoster. Neurology. 1998 Nov;51(5):1405-11
Lang PO, Ferahta N. Recommendations for treatment and prevention of herpes zoster and associated pain in aged adults. Rev Med Interne. 2016 Jan;37(1):35-42
Kim SR, Khan F, Ramirez-Fort MK, et al. Varicella zoster: An update on current treatment options and future perspectives. Expert Opin Pharmacother. 2014 Jan;15(1):61-71
Argoff CE. Review of current guidelines on the care of post-herpetic neuralgia. Postgrad Med. 2011 Sep;123(5):134-42
Raja SN, Haythornthwaite JA, Pappagallo M, et al. Opioids versus antidepressants in post-herpetic neuralgia: A randomised, placebo-controlled trial. Neurology. 2002 Oct 08;59(7):1015-21
Shrestha M, Chen A. Modalities in managing post-herpetic neuralgia. Korean J Pain. 2018 Oct;31(4):235-243
Baron R, Allegri M, Correa-Illanes G, et al. The 5 per cent lidocaine-medicated plaster: Its inclusion in international treatment guidelines for treating localised neuropathic pain, and clinical evidence supporting its use. Pain Ther. 2016 Dec;5(2):149-169
Derry S, Rice AS, Cole P, et al. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev. 2017 Jan 13;1(1):CD007393
Goncalves D, Rebelo V, Barbosa P, Gomes A. 8 per cent capsaicin patch in treatment of peripheral neuropathic pain. Pain Physician. 2020 Sep;23(5):E541-E548
Kim YH, Lee PB, Oh TK. Is magnesium sulfate effective for pain in chronic postherpetic neuralgia patients comparing with ketamine infusion therapy? J Clin Anesth. 2015 Jun;27(4):296-300
Baranowski AP, De Courcey J, Bonello E. A trial of intravenous lidocaine on the pain and allodynia of post-herpetic neuralgia. J Pain Symptom Manage. 1999 Jun;17(6):429-33
Apalla Z, Sotiriou E, Lallas A, et al. Botulinum toxin A in post-herpetic neuralgia: A parallel, randomised, double-blind, single-dose, placebo-controlled trial. Clin J Pain. 2013 Oct;29(10):857-64
Johnson RW, Rice AS. Clinical practice. Post-herpetic neuralgia. N Engl J Med. 2014 Oct 16;371(16):1526-33
Prof Dominic A Hegarty, Consultant in Pain Management and Neuromodulation and Clinical Director, Mater Private Hospital, Cork; Associate Professor of Pain Medicine, University College Cork; President, World Institute of Pain (WIP); and Clinical Director of Pain Relief Ireland – www.painreliefireland.ie












Leave a Reply
You must be logged in to post a comment.