NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
A review of the causes, symptoms, and treatment for this debilitating condition
Migraine is a complex neurological disorder. Although not life-threatening, migraine has been found to have a greater impact on quality-of-life than conditions such as heart disease and diabetes. With attacks lasting anything from a couple of hours to three days, it is easy to see why it can have such a debilitating effect on those living with the condition. The World Health Organisation (WHO) classifies migraine as the 12th leading cause of disability worldwide among women and the 19th overall.
Migraine affects 12-to-15 per cent of people worldwide (around one billion), with similar percentage figures reported (up to 500,000) for those living with the condition in Ireland.
Prior to puberty, boys experience migraine as often as girls. Once into adulthood, migraine becomes three times more common in women than in men. This is due in large part to the hormonal changes in women from puberty to menopause.
Approximately 92 per cent of Irish migraineurs report that attacks affect their performance at work, with 39 per cent of those being severely affected. Therefore, the unemployment rate for those with severe migraine is two-to-four times higher than the prevailing overall rate.
Migraine accounts for the loss of over half a million working days in Ireland each year, with 37 per cent of working Irish migraineurs missing more than five days per annum – the resultant cost to the economy is at least €250 million.
Causes
Whilst the precise cause of migraine is unknown, it is accepted that it relates to the abnormal functioning of nerve cells that affect the brain’s ability to process information such as pain, light, sounds, and other sensory stimulants.
As the condition is very individual, how each migraineur arrives at this point is then determined by a varied number of ‘trigger factors’, but generally once here, a pattern emerges, and an attack ensues. These factors can be physical, environmental, or genetic, and in most cases it will be a particular individual combination that will precipitate an attack. However, someone may experience all or only some of these during an attack.
It follows then, that identifying triggers is one of the keys to successful management of the condition.
Symptoms and types
The word ‘migraine’ derives from the Greek word ‘hemikrani’ (half-skull), which means ‘pain on one side of the head’. This accurately describes and differentiates migraine from other types of headaches, as typically it presents on one side of the head.
An attack may consist of some or all the following symptoms:
Migraine without aura (around 80 per cent of all attacks);
Moderate-to-severe pain, throbbing one-sided headache, aggravated by movement;
Nausea and/or vomiting;
Hypersensitivity to external stimuli (ie, noise, smells, light);
Stiffness in neck and shoulders;
Pale appearance.
Migraine with aura (in addition to above symptoms):
Aura – around 20 per cent experience visual disturbances prior to the headache lasting up to one hour (most commonly blind spots, f lashing light effect, or zig-zag patterns; may also include physical sensations such as unilateral pins and needles in fingers, arm and then face).
Blurred vision.
Confusion.
Slurred speech.
Loss of co-ordination.
Difference between episodic migraine and chronic migraine
Episodic migraine is defined as having 0-to-14 headache days per month compared to chronic migraine, which is defined as having 15 or more headache days per month.
Migraine accounts for the loss of over half a million working days in Ireland each year, with 37 per cent of working Irish migraineurs missing more than five days per annum
Other types
Basilar migraine
Usually affecting teenage girls, this is a rare form of migraine that presents additional symptoms such as loss of balance, fainting, difficulty speaking, and double vision. There can be loss of consciousness during an attack.
Hemiplegic migraine (sporadic or familial)
Usually beginning in childhood, this severe form of migraine causes temporary unilateral paralysis. May also feature an extended aura period that could last for weeks. Generally it is related to a strong family history of the condition. It is a rare form of migraine; diagnosis usually requires a full neurological exam, as the symptoms may be indicative of other underlying conditions.
Ophthalmoplegic migraine
In addition to headache, this very rare form of migraine shows additional symptoms such as dilation of the pupils. Inability to move the eye in any direction, as well as drooping of the eyelid occurs. It occurs primarily in young people and is caused by weakness in muscles which move the eye.
Abdominal migraine
Symptoms are usually nausea-and stomach-related rather than headache. Occurs predominantly in children, and usually evolves into typical migraine with age.
Triggers
A myriad of trigger factors, whilst in themselves not the cause of migraine, can build, bringing an individual to the point where a migraine attack is imminent.
Again, these can be different for everyone and, indeed, may differ for an individual each time, depending on their situation; trying to track down specifics can be difficult.
Environmental factors
Bright or f lickering lights (could be cinema, shop displays, or sunlight through trees whilst driving).
Certain types of lighting (f luorescent, strobe).
Strong smells (especially perfume, paint, etc).
Weather (variety of factors, ie, bright sun glare, muggy close days, humidity).
TV/computer screens and monitors.
Loud and persistent noise.
Travel areas of pressure change, ie, altitude.
Dietary triggers
Research indicates about 20 per cent of migraine attacks are brought on by dietary factors. Whilst people believe this to be the case, actual scientific evidence proving a link is virtually non-existent. In many cases, there may be other factors that precede consuming a ‘suspect’ food, which could contribute more to the onset of an attack, ie, lack of sleep, skipping meals.
The most cited link is foods which are high in the amino acids tyramine and/ or phenylethylamine, such as:
Cheese (fermented, aged or hard mouldy types).
Chocolate.
Alcohol (beer and red wine particularly).
Nitrites (common in processed meats).
Sulphites (ie, preservatives in dried fruit and red and white wine).
Additives (MSG).
Aspartame (diet drinks).
Caffeine (coffee, tea, etc; although caffeine can be used to prevent migraine, it is down to personal tolerance).
Hormonal triggers
Once females move into puberty and then adulthood, hormones play an increasing role in migraine prevalence. Oestrogen f luctuations due to menstruation or using oral contraceptive pills or HRT can sometimes trigger migraine. Conversely, migraine susceptibility can decrease during pregnancy when oestrogen levels are high.
In the main, migraine attacks lessen post-menopause (although can increase in the years preceding it). Identifying triggers can be the single most crucial step an individual can take in helping themselves to manage their condition. It may not be necessary to avoid situations completely, but instead build levels of awareness so that appropriate preventative steps and actions can be taken.
Treatment
The key to successful treatment is to establish correct diagnosis of migraine and eliminate other potential causes (tension or cluster headache in particular; see more at end of this article about non-migraine headaches). Some time spent with patients at an early stage reviewing their current medication regimen would prove hugely beneficial in identifying and/or preventing ‘medicine overuse headache’.
In acute treatments, the goal is to stop or at least alleviate the effects of an attack once it has begun.
Analgesics
Used to target area-specific pain and especially if taken as early as possible once an attack begins, analgesics can be a hugely effective pain killer.
Aspirin
Traditional first-line of defence, has anti-inf lammatory properties that can help alleviate many of the physical symptoms of migraine.
Paracetamol
As effective as aspirin, but without the anti-inf lammatory effects.
Combinations
Drugs that contain aspirin or paracetamol along with another agent such as codeine or caffeine; codeine and other opiates are best avoided due to addiction, side-effect risk, and risk over triggering ‘over-use headaches’.
NSAIDs
Generally used for more severe migraine attacks, evidence shows ibuprofen to be highly effective. Soluble forms may act quicker than tablet form for those where stomach issues are part of their migraine episode.
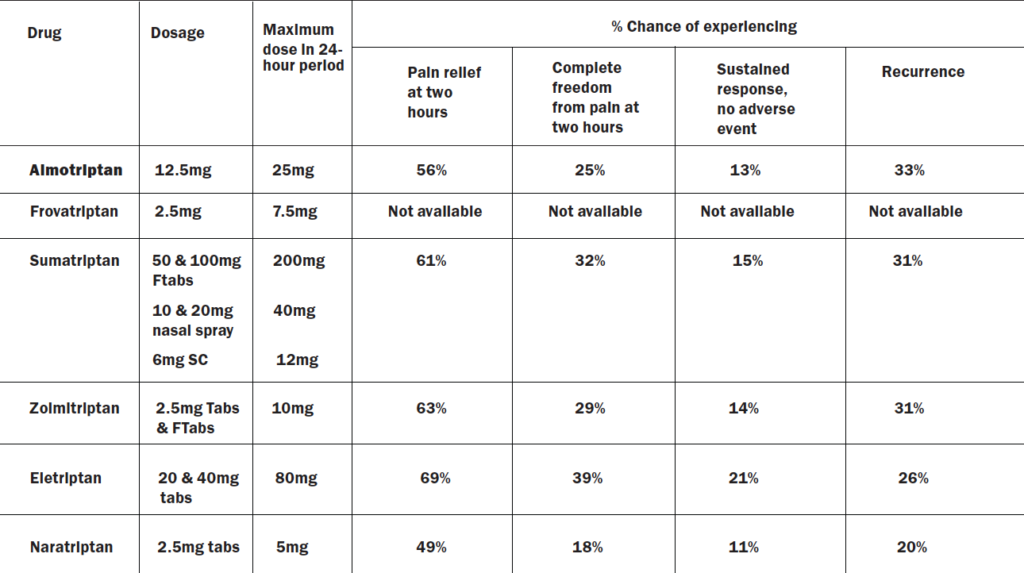
Triptans
Triptans are highly effective, reducing the symptoms or aborting the attack within 30-to-90 minutes in 70-to-80 per cent of patients. Triptans target those neural serotonin receptors specifically involved in migraine attacks and can be used in the treatment of migraine with or without aura. All of them are available in tablet form, with some brands also available as fast-melt tabs, nasal spray, or SC injection.
The table below shows those triptans available in Ireland, along with information from trials regarding effectiveness over the course of an episode. In all cases, these are only for treatment where migraine has been diagnosed and not for the treatment of hemiplegic, basilar, or ophthalmoplegic migraine.
Currently all are prescription-only medicines (POM), apart from sumatriptan, which now has an option for sale over-the-counter (OTC) in the pharmacy for patients with the diagnosis of migraine who have been prescribed it in the past.
Preventative medication for migraine
Prophylactic medication may be considered if the patient has taken adequate lifestyle steps to prevent migraine, such as using a diary to determine triggers and avoidance of these triggers, but the migraine continues. It would be reasonable for a prescriber to consider prophylaxis for migraine if a patient must use analgesics for eight or more days of the month. Prophylactic medication should be tried for four-to-six months at a reasonable dose to determine if it is working effectively. Prophylactic medication has potential side-effects that can limit dose or use. Amitriptyline, topiramate, and f lunarizine are the three most prescribed migraine prophylactic drugs, with amitriptyline being the most prescribed. Other prophylactics such as sodium valproate, pregabalin, gabapentin and pizotifen are considered second-line (often only used if the first three are not tolerated or ineffective).
Amitriptyline
Amitriptyline is a traditional tricyclic antidepressant, but is not used much for depression due to side-effects such as drowsiness, constipation, dry mouth, vivid dreams or nightmares and risks in people with glaucoma. It is dangerous in overdose. A low dose may be effective in preventing migraine; the dose for migraine varies between 10mg to 150mg, but the lower the better and it should only be titrated up slowly. Use at six months at maximum tolerated dose before considering changing.
Topiramate
Topiramate is traditionally an epilepsy drug that is sometimes used in low-dose form to prevent migraine. It must be used with caution in those with liver or kidney problems and must be avoided in pregnancy. Possible side-effects include nausea, vomiting, constipation, diarrhoea, decreased appetite, drowsiness, and sleeping problems. Highest daily dose of 700mg, but for migraine, recommended dose is 25mg to 200mg twice daily. Starting dose is 25mg at night for two-to-eight weeks and increase gradually.
Propranolol
This is an old-style beta blocker traditionally used for angina and blood pressure, but is rarely used for these indications nowadays due to safer newer versions of beta blockers with less side-effects. However, in low doses, it is used for migraine prophylaxis in some people. It should be used in caution in people with asthma, COPD, some heart problems, and diabetes. Side-effects can include cold hands and feet, pins and needles, tiredness, and sleeping problems.
Flunarizine
Flunarizine can take months to see a significant reduction in symptoms. Patients should be regularly reviewed to assess their response to this preventative treatment and if a sustained attack-free period is established, interrupted flunarizine treatment should be considered.
If the patient is responding satisfactorily to f lunarizine and a maintenance treatment is needed, the same daily dose should be used, but this time interrupted by two successive drug-free days every week, ie, Saturday and Sunday. Even if the preventative maintenance treatment is successful and well-tolerated, it should be interrupted after six months and it should be re-initiated only if the patient relapses.
Treatment is started at 10mg daily (at night) for adult patients aged 18- to-64 years and at 5mg daily (at night) for elderly patients aged 65 years and older. It is good practice to start at 5mg for all patients before titrating up. Side-effects include increased weight, increased appetite, depression, insomnia, constipation, stomach discomfort, and nausea.
Gabapentin
Like topiramate, gabapentin is traditionally an epilepsy drug. It may be used if topiramate, f lunarizine, or propranolol are not effective or tolerated. However, in recent years, studies have indicated that gabapentin may not be as effective for preventing migraine as first thought. Side-effects can include dizziness, drowsiness, appetite increase, weight gain, and suicidal thoughts.
Sodium valproate is another epilepsy drug occasionally used for migraine prevention if other prevention options fail or are not tolerated. Other preventative medicines include pizotifen and pregabalin.
Riboflavin (vitamin B2)
There has been some indication that vitamin B2 supplementation may help prevent migraine; however, this has not been proven.
Botox
Botox injections were introduced in recent years as a preventative treatment for chronic migraine. It is administered in 30-to-40 injection sites located across seven head and neck muscle groups. It is administered every 12 weeks, as its effect wears off after this period. It should be administered by doctors specialising in administering Botox for migraine, as it is more complicated than simply administering Botox to points on the skin, as is done for its anti-wrinkle effect on the likes of the forehead. Patients need two bouts of Botox injections to be able to determine it is working. While Botox use for migraine has varying degrees of success, it is shown to be successful (headaches cut in half) in 30-to-50 per cent of patients after two rounds of treatment and this may increase to a 70 per cent success rate in patients after five rounds of Botox. Botox reduces migraine by reducing neurotransmitter signalling in the brain. The patient may still be prescribed other preventative drugs for migraine even if receiving Botox treatment.
Table adapted for Irish market, source data from a meta-analysis of head-to-head trials, in C Asseburg, P Peura, T Oksanen, JA Turunen, T Purmonen and J Martikainen (2012). Cost-effectiveness of oral triptans for acute migraine: Mixed treatment comparison. No head-to-head info available for Frovatriptan
New migraine drugs
A new class of migraine preventative drugs called anti-calcitonin gene-related peptide (CGRPs) are monoclonal antibodies (MABs), which inhibit the action of the CGRP neurotransmitter, have come to market in the last three years.
The CGRP’s role in migraine includes:
Being released in the trigeminal nerve.
Increasing levels are seen during migraine attacks.
It dilates blood vessels.
It reduces mast cells (cells that control inf lammation during allergic reactions).
Causes an inf lammatory fluid in blood vessels.
For this reason, CGRP inhibitors are effective in reducing migraine.
The four CGRP inhibitors that have come to market in Europe and America are erenumab, fremanezumab, eptinezumab, and galcanezumab.
Erenumab, fremanezumab, and galcanezumab are all currently available in Ireland under the High-Tech Scheme (the manufacturer of eptinezumab has not looked for licencing in Ireland) for prophylaxis of chronic migraine in adults who have failed three or more prophylactic treatments.
A managed access protocol is in place for the three approved CGRP MABs, which outlines the criteria that must be satisfied in order for a patient to be recommended for reimbursement under the High-Tech Scheme .
Prescribing of these agents is confined to consultant neurologists who have agreed to the terms of the HSE-managed access protocol and have been approved by the HSE Medicines Management Programme. The approved clinician must submit an online application for individual reimbursement approval for each patient.
Galcanezumab and cluster headaches
On a separate very positive note for people living with cluster headaches, galcanezumab was granted US FDA approval in 2019 to treat episodic cluster headache. It was initially approved for migraine prevention by the FDA in 2018 and the FDA extended the licencing of galcanezumab to include treatment of episodic cluster headache after positive trial results. Studies showed that 71.4 per cent of patients had weekly cluster headache attacks cut in half with galcanezumab. It is the first new treatment to be approved for cluster headaches since triptans (and triptans were initially developed for migraine). While there is no licensing approval for galcanezumab in Europe and Ireland for cluster headaches yet, its success in American trials and subsequent FDA approval gives optimism that it will come to the market here to treat cluster headache in the coming years.
What is cluster headache?
Affecting around 1 per cent of people, this is a rare, but very severe, headache found six times more commonly in men and usually begins in the late 20s or early 30s. Typically, attacks begin in the middle of the night. The primary symptom is a severe stabbing pain affecting one side of the head. The side affected can vary between attacks, but only in very rare cases would it affect both sides of the head at the same time. The duration of an attack can be between 15 minutes and up to three hours. Attacks come in clusters (hence the name) and can occur several times a day over a period of weeks or even months after each cluster, though attacks can disappear for months or years.
A cluster attack can be distinguished from a migraine attack in that with cluster headache, the person is agitated during an attack or is unable to sit or lie at peace or find relief though sleep.
During an attack other symptoms may occur such as red or watery eyes, runny nose, nasal congestion, or facial sweating. In addition, a sufferer’s eyes may be affected, with constriction of the pupil or drooping or swelling of the eyelid. Cluster headache is described by some medics as ‘the most painful event that can happen a person’, which emphasises the severity of the condition.
Whilst the cause is unknown, suspected trigger factors include alcohol, tobacco, irregular sleeping patterns, stress, and decreased blood oxygen levels. The most common treatment for cluster headache is the inhalation of pure oxygen and is only successful if the mask fits perfectly without leaking.
Barriers to patients accessing neurologists
Migraine Ireland has flagged issues with the HSE’s managed access protocol for CGRP inhibitors, including delays transferring patient records to the High-Tech Scheme to allow access to the CGRP inhibitors currently approved in Ireland.
A barrier to access for migraine patients is lack of access to neurologists in Ireland. Inadequate numbers of neurologists in Ireland has long been a problem. As far back as 20 years ago, the WHO commissioned an Atlas Country Profile Report (2001) on mental health resources and services, surveying 51 European countries. This report showed Ireland had the lowest number of neurologists per 100,000 population, at 0.38 neurologists per 100,000 in 2001. The report showed the average number of neurologists per 100,000 population out of 51 European countries was 5.82 per 100,000. Ireland was lower than former Eastern block countries like Albania that were, at the time, only starting to recover from years of oppressive regimes and economic hardship. Even Bosnia and Herzegovina, which were not long out of a bitter civil war and still had 500,000 displaced refugees, had a higher number of neurologists per 100,000 than Ireland.
While the number of neurologists per 100,000 population in Ireland has increased in the intervening 20 years, Ireland still has the lowest number of neurologists per 100,000 in Europe. There are currently 61 public neurologist posts in Ireland; compared to 320 in Finland, which has a similar population and socio-economic status. There also remains much geographic inequality as regards access to neurologists in Ireland.
There are currently specialist clinics for headache and migraine based at Beaumont Hospital, St Vincent’s University Hospital, Tallaght University Hospital (all in Dublin), and Cork University Hospital, which provide access to new treatments like CGRP inhibitors. Private hospitals also offer access to neurologists specialising in migraine.
Other new migraine drugs on the horizon
Gepants
Gepants are a new class of drug that are relatives of anti-CGRP drugs like erenumab and fremanezumab; they also block the CGRP receptor and are effective at relieving migraine.
Gepants are an oral medication. Side-effects include nausea, somnolence, and dry mouth.
They work quicker than anti-CGRP inhibitors like erenumab and fremanezumab.
Rimegepant, ubrogepant, and atogepant are examples of gepants.
In America, rimegepant received FDA approval in 2021 as both an acute and preventative treatment for migraine; ubrogepant got FDA approval as an acute treatment of migraine, while the FDA approved atogepant as a preventative treatment of episodic migraine in adults in September 2021 and is currently being considered by the FDA for expanded use.
Whilst the cause is unknown, suspected trigger factors include alcohol, tobacco, irregular sleeping patterns, stress, and decreased blood oxygen levels
In the UK, the National Institute for Health and Care Excellence (NICE) is currently appraising rimegepant for treatment and prevention of migraine. Other gepants are also in the pipeline.
Rimegepant received a marketing authorisation from the EMA valid throughout the EU on 25 April 2022, for both acute and preventative treatment.
Ditins
Lasmiditan is a new oral medication for the acute treatment of migraine attacks with or without aura and is the first of the ditin class. It was approved by the FDA in the US in 2019, but is not yet approved in Europe. It is not an anti-CGRP medication, but works by blocking the 5-HT 1F serotonin receptor, so is similar in its mechanism of action to triptans. However, triptans work by blocking the 5-HT 1B and 5-HT 1D receptors. Advantages of ditins over triptans are that there is decreased stimulation of the trigeminal system and unlike triptans, ditins do not cause vasoconstriction, so can be used instead of triptans when triptans are contraindicated due to cardiovascular issues.
Support
The Migraine Association of Ireland provides a range of useful supports for patients with migraines and clinicians treating migraine patients. Visit www.migraine.ie or call 1850 200 378. Additionally, further information about living with migraine can be found on www.speakyourmigraine.ie.
TIPS FOR PATIENTS TO MANAGE MIGRAINE
Keep a migraine diary – identify any potential triggers and make a note of how they affect you
Establish a daily routine – and stick to it as much as possible
Practice good sleep hygiene – go to sleep and wake up at a similar time daily
Limit screen time – take regular breaks from your phone, TV, or desktop during the day
Practice self-care – exercise, eat healthy meals regularly, and stay hydrated
If consuming alcohol do so in moderation
Reduce stress – try yoga, meditation or mindfulness
Stay in touch – maintain contact with friends, family, and support groups












Leave a Reply
You must be logged in to post a comment.