NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Theresa Lowry Lehnen, PhD, Clinical Nurse Specialist Practitioner and Associate Lecturer at Institute of Technology Carlow, and Member of the Irish Student Health Association (ISHA)
- 01st Oct 2020
Meningitis Vaccine
Worldwide, bacterial meningitis is among the top 10 causes of infection-related death and it is important for clinicians to remain up-to-date on this potentially fatal disease
Meningitis is an acute inflammation of the meninges, the protective membranes that surround the brain and spinal cord. It is caused by bacterial, viral and less often parasitic and fungal infections however, the bacterial form of meningitis is the most severe. Viral meningitis can make people feel very unwell, but is rarely life threatening, usually resolves on its own and seldom causes long-term complications. Bacterial meningitis however, is a serious illness, a medical emergency and a public health concern. Bacterial meningitis is an infectious disease associated with substantial mortality and a risk of permanent disability in survivors.
Mortality remains as high as 30 per cent in pneumococcal meningitis, 5-to-10 per cent in meningococcal meningitis and up to 50 per cent when untreated. Outcomes are improved by prompt recognition of symptoms and treatment with dexamethasone and intravenous antibiotics, which should be administered as soon as possible and preferably within the first hour.
Several types of bacteria can cause bacterial meningitis, including Streptococcus pneumoniae, Haemophilus influenza, Neisseria meningitides, Listeria monocytogenes, and Group B Streptococcus. The average incubation period is four days, but can range between two and 10 days. Early symptoms of meningitis include nausea and vomiting, fever, headache and a stiff neck, muscle pain, light sensitivity, confusion, cold hands or feet and mottled skin and in some cases, a rash that does not fade under pressure. These symptoms can appear in any order and only some may be present. Later symptoms can include seizures and coma. Infants are at higher risk of developing bacterial meningitis, and it spreads easily in areas with large gatherings of people such as schools and college campuses. Other factors that can increase the risk include an anatomical defect or trauma, such as a skull fracture or surgery, which could allow bacteria to enter the nervous system, an infection in the head or neck area, living in or traveling to high risk areas, a weak immune system, and working in laboratories and other settings where meningitis pathogens are present.
There were 89 cases of bacterial meningitis reported in Ireland in 2018. Vaccination is key to preventing meningitis and it is important to follow the recommended vaccination schedule. H. influenza is the main cause of bacterial meningitis in children under five years of age in countries that do not offer the Hib vaccine.
Meningococcal bacteria live at the back of the throat and in the nose. Nasopharyngeal carriage of meningococci is common. About 10 per cent of the population carry meningococci at any given time, however, not all are virulent strains. Most carriers remain well, but they can spread the bacteria to others through coughing, sneezing, sharing personal items such as utensils, cutlery, and toothbrushes or through kissing and close or prolonged personal contact. Humans are the only natural hosts for meningococci and the organism dies quickly outside the human host. Meningococcal disease can occur at any age, but the highest rate occurs in children under five years.
Group B streptococcus can pass from mothers to newborns during delivery. Meningococcal B disease is most common in children under one year of age and the next highest risk group are young people aged 15-19 years. The risk of infection in Ireland is highest in winter and early spring. Of those who get meningococcal disease (the combination of meningitis and septicaemia), one-in-20 will die and one-in-10 people who recover will have a major disability such as deafness, brain damage or loss of fingers, toes, hands, feet, arms, or legs.
Neisseria meningitidis, often referred to as meningococcus, is a Gram-negative bacterium that causes meningitis and other forms of meningococcal disease such as meningococcaemia, a life-threatening sepsis.
Vaccination
Before the introduction of the meningitis C (MenC) vaccine in 2000, groups B and C caused most cases of meningococcal disease in Ireland. Since the introduction of the MenC vaccine the number of cases of meningococcal disease due to group C bacteria has fallen dramatically and most cases are now caused by group B bacteria.
Meningococcal disease can occur at any age but the highest rate occurs in children under five years
All children in Ireland are offered MenB vaccine at two and four months of age with a booster dose given at 12 months. For babies born on or after 1 October 2016, the administration of MenC vaccine changed from four months, to six months to allow the administration of the MenB vaccine at two and four months for earlier protection against meningococcal B infection, which is the most common type of meningococcal infection in this age group. A further dose of MenC vaccine is given to babies at 13 months as a combined Hib/MenC vaccine.
In addition, all students entering first year of secondary school from September 2020 will be offered a booster dose of the Meningococcal ACWY (MenACWY) non-live vaccine. The MenACWY booster vaccine is given to protect teenagers up to and including early adulthood from life-threatening meningococcal group A, C, W, and Y infection.
There are few exceptions to immunising children with the MenB and MenC vaccines, however – a child who has had a severe allergic reaction or anaphylaxis to a previous dose or any part of the vaccine including tetanus should not get the vaccines.
Symptoms
Meningococcal disease may present with clinical features that are indistinguishable from those associated with other acute self-limiting systemic illnesses. Meningitis due to Neisseria meningitides can begin with flu‐like symptoms such as fever, muscle aches and vomiting, before meningitis becomes clinically apparent. Symptoms such as pallor, altered mental state or limb pain should raise suspicion of meningococcal disease. Rapid onset and progression of symptoms over a period of hours is typical and can help to distinguish it from viral meningitis. A patient presenting with meningitis and a non‐blanching petechial or purpuric rash strongly suggests meningococcal disease, although the rash may also be blanching, maculopapular or absent.
The rash can appear rapidly on any part of the body including the palms of the hands and soles of the feet. The rash may go unnoticed unless the acutely unwell patient with a systemic febrile illness is completely undressed so that a thorough search for a haemorrhagic rash can be undertaken. Meningitis due to Streptococcus pneumoniae should be suspected in patients with predisposing conditions, such as sinusitis, otitis media, mastoiditis, cerebrospinal fluid leak, cochlear implants, asplenia, human immunodeficiency virus (HIV) infection, or other immunosuppressive conditions. Meningococcal disease usually presents as meningitis or septicaemia, or a combination of the two. Septicaemia, with or without meningitis, can be particularly severe and is associated with a considerably greater mortality rate than meningococcal meningitis without bloodstream infection.
Diagnosis and treatment of bacterial meningitis
A presumptive diagnosis of bacterial meningitis is a medical emergency and immediate referral to hospital is required. Antibiotic therapy should not be delayed while initiating referral. GPs and advanced paramedics should have benzylpenicillin available when attending patients and administer it without delay to patients with a systemic febrile illness and a petechial or purpuric rash. Ceftriaxone or cefotaxime are suitable alternatives if necessary. For optimal benefit, benzylpenicillin should be given intravenously. However, if unable to access the intravenous route, it can be administered intramuscularly.
Benzylpenicillin should only be withheld if the individual has a proven history of penicillin anaphylaxis. Doses of benzylpenicillin used for suspected cases of meningococcal disease are: Adults or children aged 10 years or over: 1200mg; Children aged 1-9 years: 600mg and for children aged <1 year: 300mg. GPs or advanced paramedics are not expected to carry an alternative antibiotic to benzylpenicillin, however, if unavailable a third generation cephalosporin such as ceftriaxone 80mg/kg (up to 2g) IM or IV for all ages or cefotaxime 50mg/kg (up to 2g) IM or IV for all ages can be used and are acceptable for the empirical treatment of suspected meningococcal disease prior to transfer to hospital. GPs or advanced paramedics should telephone and inform the emergency department and clinician at the referral hospital of the patient’s expected arrival so that delays in treatment are minimal. Clinical notes accompanying the patient should inform the hospital clinician which antibiotics have been administered and their dose.
When invasive meningococcal disease is suspected the diagnosis must be confirmed as quickly as possible (again, antibiotic treatment should not be delayed while initiating or awaiting results of diagnostic tests). The following samples should be taken at the time of initiating treatment in all suspected cases: Blood cultures; throat/pharyngeal swab; samples from other sterile sites as clinically appropriate, eg, joint, pericardial, or pleural effusions, CSF. Blood should also be taken for a full blood count and PCR testing for meningococcal DNA. Serology may occasionally be beneficial and consultation with a microbiologist should be considered.
Lumbar puncture is recommended for all cases with clinical meningitis, but should be deferred until the patient is haemodynamically stable and there are no contraindications such as cerebral oedema or raised intracranial pressure. CSF obtained from a patient with meningococcal meningitis typically has a high neutrophil count, low glucose and high protein content. However, low or absent white cells do not exclude meningitis and initial CSF tests can be normal in up to 5 per cent of cases. In some instances, imaging such as a computed tomography (CT) scan will be recommended before the lumbar puncture, to help determine if it is safe to perform the lumbar puncture and if another condition may be contributing to the patient’s symptoms such as a brain haemorrhage or tumour.
Treatment, complications and outcomes
The treatment and long-term outlook of meningitis differ considerably based upon whether it is caused by a virus or bacterium. However, this distinction may not be clear until the culture results are available, usually 48 to 72 hours after they are obtained. The length of antibiotic treatment depends upon the results of the bacterial cultures. If the cultures are negative and the patient has improved, antibiotics may be discontinued after 48 to 72 hours. If cultures are positive, the length of treatment depends upon the bacteria identified and extent of complications that occur. The treatment course may range from several days to several weeks. Worldwide, bacterial meningitis is among the top ten causes of infection-related death.
Although effective antimicrobial treatment is available and administered, fatality rates are still very high and 50 per cent of affected patients suffer long-term sequelae due to severe complications, such as hydrocephalus, cerebral oedema, cerebrovascular complications, and ventriculitis. Deafness, brain damage or loss of fingers, toes, hands, feet, arms, or legs are associated complications. Intracranial complications are associated with a worse outcome and are often the cause of long-term sequelae.
The occurrence of hydrocephalus in patients with acute bacterial meningitis is associated with worse outcomes. The fatality rate of these patients reaches up to 46 per cent, whereas the fatality rate of patients without hydrocephalus is around 17 per cent. Arterial cerebrovascular complications such as stroke and cerebral haemorrhage, occur in approximately 15-20 per cent of patients with bacterial meningitis. Vasculitis and/or vasospasms are the most likely cause of these complications. Septic thrombosis of cerebral veins and sinus occurs in about 10 per cent of patients with bacterial meningitis. Epileptic seizures are a common complication of bacterial meningitis.
In some cases they are the first presenting symptom, indicating impending herniation or the presence of an intraparenchymal abscess or cerebritis/encephalitis. Approximately 5 per cent of patients with acute bacterial meningitis experience seizures. Cerebritis and brain abscesses occur in approximately 1-to-5 per cent of patients with bacterial meningitis. On clinical examination the patients often presents a focal neurological deficit, such as partial paralysis or speech disorder, epileptic seizures or cephalgia, which is commonly one-sided. Abscesses can be the cause or the consequence of meningitis and are best detected by MRI or even MR spectroscopy.
Treatment for viral meningitis is mainly supportive. This includes rest, fluids or intravenous fluids if the patient is unable to drink, and medications to treat fever and/or headache. Most patients with viral meningitis recover with no long-term complications. Symptoms usually begin to improve within one week, although some will have fatigue, irritability, decreased concentration, muscle weakness and spasm, and difficulty with coordination for several weeks or more. Death is uncommon with viral meningitis.
Public health
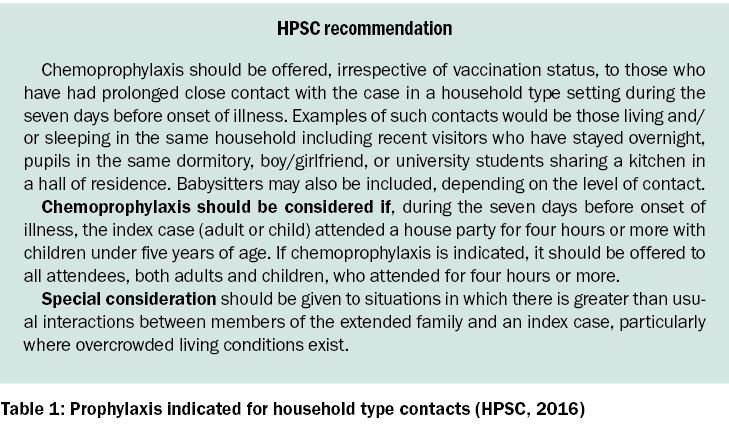
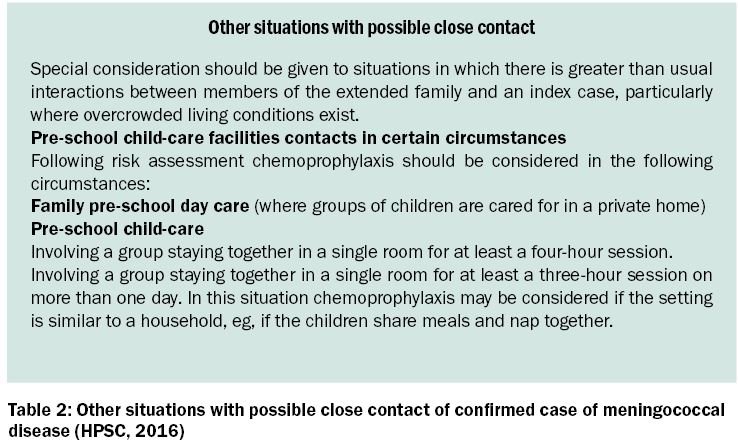
The public health response to meningococcal disease includes identification of close contacts, arranging appropriate chemoprophylaxis and provision of appropriate information. Chemoprophylaxis is indicated only for those in close contact with a case in the seven days preceding the onset of illness. It reduces the risk to other susceptible individuals in the network, protecting them from acquiring the meningococcal strain from the carrier and possibly invasive disease.
Chemoprophylaxis should be given to all identified as close contacts as soon as possible preferably within 24 hours after notification of the index case. However, it can be given up to a month after onset of illness in the index case. Three antibiotics, rifampicin, ciprofloxacin and ceftriaxone are currently used in Ireland for chemoprophylaxis of meningococcal disease. Depending on the serogroup of the index case, vaccination with MenC or MenACWY vaccine may be recommended for close contacts.
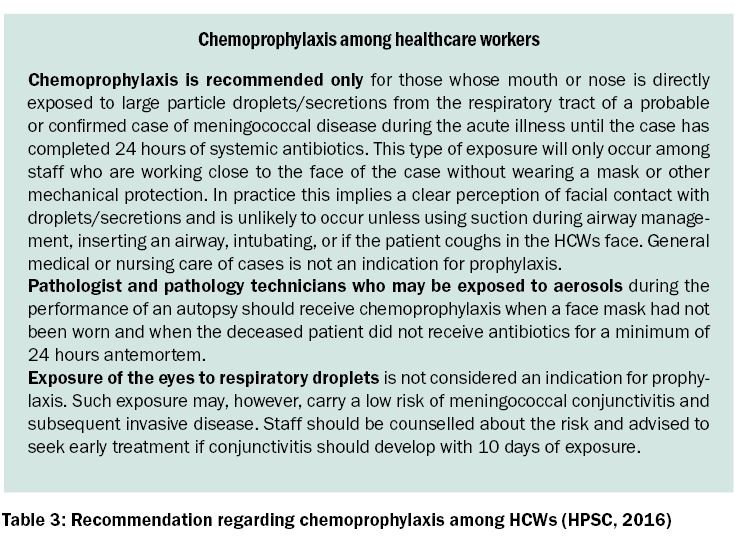
Healthcare workers in contact with cases of meningococcal disease are at increased relative risk of disease in the 10-day period following exposure. Outbreaks of meningitis may occur in the general community or in settings such as crèches, schools, and colleges. The public health actions for each of these settings may vary and will depend on the identification of epidemiological links between cases and identification that the same organism is associated with the outbreak cases. The objective of public health management of such outbreaks of invasive meningococcal disease is to interrupt transmission and prevent further cases. Once an outbreak is either suspected or recognised there is an immediate need to initiate a coordinated response. Following a case or outbreak of meningococcal disease, it is important for public health to disseminate information appropriately, as early detection, diagnosis, and treatment improves outcomes. Disseminating information to the community may require use of mass media, websites and community meetings and help lines.
Before the introduction of the meningitis C (MenC) vaccine in 2000, groups B and C caused most cases of meningococcal disease in Ireland
Vigilance for signs and symptoms among contacts is important especially in the immediate one-week high-risk period after the onset of symptoms in a confirmed case. Information disseminated should be sufficient to ensure public awareness of the situation while maintaining patient confidentiality. The family of a confirmed case should be informed that information will be distributed as appropriate. Leaflets or other printed material about meningococcal disease should be widely available and quickly distributed after reporting of a confirmed or clinical case.
Vaccination and patient education
Vaccination provides the best chance of protection against meningococcal disease. Opportunistic discussion in practice with patients helps reinforce the importance of vaccination programmes and adherence to the recommended schedules. Providing education to pregnant women and their partners about the importance of childhood immunisations programmes can help increase knowledge, vaccine uptake, and the timeliness of receipt of childhood vaccinations. Discussion involves debunking myths and addressing parental concerns about vaccine safety. Clinicians must continue to address the gaps in patient knowledge through detailed educational efforts and effective communication techniques.
It is imperative that practice nurses and doctors are up to date on research and immunisation guidelines, and are able to communicate effectively the benefits and importance of vaccination. Effective communication techniques providing evidence-based information and best practice advice can address misconceptions and gaps in patient knowledge, leading to informed choices, patient education, and improved outcomes.
References on request
For reliable and up-to-date information about HSE immunisation programmes visit HSE NIO: https://www.hse.ie/eng/health/immunisation/












Leave a Reply
You must be logged in to post a comment.