







Whilst the potential outcomes and complication rates are not insignificant with hypospadias repairs, the benefits of performing a repair appear to outweigh the risks.
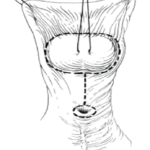
Hypospadias is the most common congenital malformation of the penis, affecting approximately 1/250 live male births, and consists of a triad of a proximally placed urethral meatus, hooded foreskin, and varying degrees of ventral chordee (bend) (Figure 1). The aetiology of this condition remains unclear and is likely to be multifactorial. In distal hypospadias, many hypotheses have been put forward implicating low birth weight, placental insufficiency, maternal age, endocrine disrupters, and even altitude.
Proximal hypospadias, however, appears to have a different developmental aetiology, with much research focused on the role of prenatal androgen exposure as a putative causative factor. Many of the studies exploring the role of antenatal testosterone are derived from rodent models. Whilst there are significant anatomical and endocrine differences between rodents and humans, extrapolation has led to the description of a masculinisation-programming window (MPW) at weeks eight-to-14 of gestational development in humans, during which androgen action is essential for urogenital development and testicular descent.
The European Association of Urology (EAU), the American Urological Association, and the British Association of Paediatric Urology all strongly endorse surgical management being initiated (if not completed) by a maximum of 18 months of age. With a black box warning still present on all anaesthetic agents below the age of 12 months except for morphine and dexmedetomidine, it would appear logical to utilise a window between 12 and 18 months. Operating after 18 months can lead to a more challenging patient in terms of the ability to recall events, mistrust, the placement of a catheter/stent in a sensate potentially toilet-trained patient, defiance, parental anxiety, schooling policies, and post-operative complications (O’Kelly F, manuscript in press). Put simply, younger children experience fewer complications. In some institutions within the Republic of Ireland, the average wait time to be seen in a paediatric urology clinic can be over two years, and surgical wait times well in excess of this. Post-Covid-19, some hospitals have also changed the designation of certain patient conditions such as hypospadias, with the result that they are now categorised as long-term, non-urgent.
One could certainly make the argument that certain types of distal hypospadias could comfortably be managed in early adult, where the patient becomes a stakeholder in the informed consent process. There have, however, been studies which have demonstrated that adults undergoing a delayed repair for distal hypospadias are more inhibited in seeking sexual contacts, and negatively appraise their genitals compared with controls. There are no studies describing men who have undergone a primary repair for proximal hypospadias as adults.
Surgical approach
In general, with postoperative management for more complicated repairs, one can employ urinary diversion with a soft, pliable urethral stent, which decreases rates of meatal stenosis and urethrocutaneous fistula development. Distal repairs can in theory be performed without diversion, however, about 2-to-5 per cent patients will have difficulties voiding post-operatively. The use of antibiotic prophylaxis is controversial and should be made on an ad hoc basis. Bladder spasms can place undue stress on urethroplasty and therefore oral oxybutynin liquid can help (this is currently difficult to source in Ireland). Regular Calpol and ibuprofen (no increased risk of bleeding) can be used for about 48 hours. There is no evidence that oral morphine improves recovery, and studies have repeated advised against its use.
There are several limitations in the current literature pertaining to their retrospective nature, small cohort sizes, variations in technique, poorly defined outcomes, lack of independent outcome assessment, and patient loss to follow-up. In a country the size of Ireland, all those performing these repairs should be reporting outcomes to a central repository. This has to date not been universally accepted.
Even in those boys who have undergone hypospadias repairs in a timely fashion within a well-established centre, the complication rate is high. There are currently no synthetic materials available globally for reconstruction of the ventral penis, and unlike the case of adult strictures, or traumatic injuries, boys with hypospadias have a paucity of tissue, and often the presence of dysgenetic bulbospongiosus muscle. The result is that coverage can be an issue.
Even in those boys who have undergone hypospadias repairs in a timely fashion within a well-established centre, the complication rate is high
Pfistermuller undertook a meta-analysis of 49 studies with 4,675 boys who had undergone a distal tubularised, incised plate repair and described a complication rate of 10.6 per cent (reoperation rate 4.5 per cent), with fistulae (5.7 per cent), and meatal stenosis (3.6 per cent). Outcomes improved with use of an additional layer of dartos coverage, but proximal and re-operative cases had a significantly higher complication rate. There are clear differences in outcomes between distal and proximal repairs.
Distal hypospadias complication rates: 17-to-24 per cent
- Urethrocutaneous fistula and glans dehiscence more common in the first year.
- Urethral stricture more common as late complication.
Proximal hypospadias complication rates: 25-to-70 per cent
- Urethrocutaneous fistula most common (3-to-55 per cent) > glans dehiscence and meatal stenosis.
- Urethral diverticula occur more frequently in setting of a Byars’ flap repair or onlay procedure vs a two-stage graft repair.
The initial belief was that majority of complications occur within the first year of surgery, however, it is now recognised that longer follow-up should be advocated as it universally yields higher complication rates. Adolescents and young adult patients must also be followed up through a transitional/adolescent urology clinic with both paediatric and adult expertise, due to the unique functional and sexual issues which arise following hypospadias repair in that age cohort. Complications do not end at puberty.
Parental and patient perception of outcomes may also differ from surgeons.
Issues that contribute to parental decisional regret:
- Development of complications;
- Parental hesitancy regarding potential surgery;
- Desire for circumcision.
Issues that decrease parental conflict about repair:
- Improved parental education;
- Understanding of hypospadias repair.
Patient-reported outcomes should play a role in the management of this condition, and there are a number of validated scales that are now in use which include, but are not limited to, the Hypospadias Objective Scoring Evaluation (HOSE) (unique in that a standard set of post-surgery pics are obtained and scored by independent panels consistent of parents, patients, and paediatric urologists), the Paediatric Penile Perception Score, the Genital Perception Score, and the Hypospadias Objective Penile Evaluation (HOPE) score. Each instrument incorporates similar components to varying degrees (meatus, presence of fistula, quality of urinary stream, penile length, skin appearance, general penile appearance).
The risk factors for hypospadias complications include a proximal meatus, re-operation, glans width <14mm, prior use of testosterone, and the lack of barrier flaps over the neourethra.
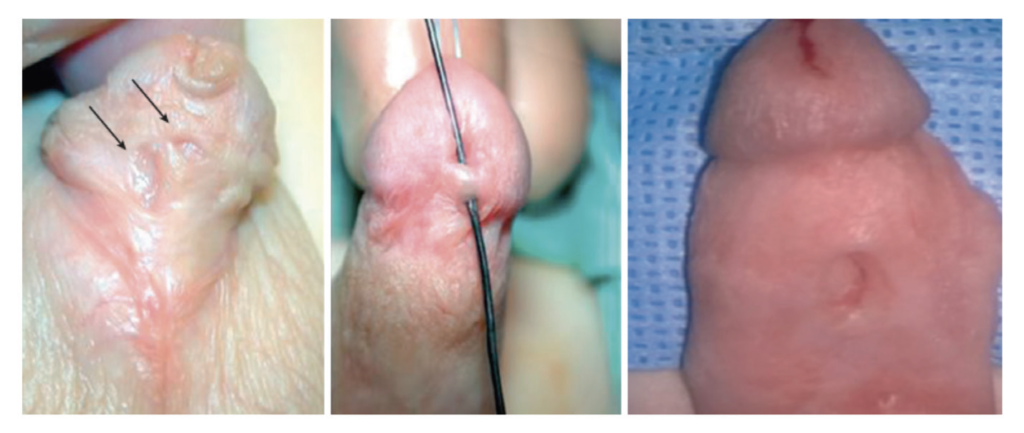
Urethrocutaneous fistula
These are most often at site of original urethral meatus or at coronal margin (Figure 2). Most are noticed within first two years after surgical repair (may be delayed until toilet training, when voiding more likely to be observed). The management of these depends on the number, size, location of fistulae, and presence of additional complications. One should assess for obstruction, excise the tract and close the opening, and use flap coverage over the defect. If the fistula appears unexpectedly at the coronal margin, one needs to consider distal narrowing or poor local tissue (consider revising urethroplasty). The recurrence of fistula is estimated at ~20 per cent of cases, and may be lessened if additional well-vascularised, non-epithelialised layers used.
Meatal stenosis
These are defined as a narrowed meatus with symptoms of stranguria (feeling of incomplete emptying), def lected stream, poor urof low, or urinary retention. They are more common in Afro-Caribbean populations. They can be repaired through meatal dilation +/- topical betamethasone cream, or a meatoplasty. When performing the initial repair, it is important to limit the incision to the urethral plate, create an oval opening, and to incorporate glans wings independent of the neourethra.
Neourethral strictures
This is defined by urethral narrowing that extends more proximally than the meatus; tends to form at the junction of the native and neourethra, along the path of the neourethra, or within the glans. Patients present with symptoms of diminished urine stream force, stranguria, urinary retention, and UTIs. It is thought that they arise out of improper urethroplasty technique, tissue ischaemia, trauma, or infection. The treatment for this can involve an endoscopic endourethral incision in lesions <1cm (not effective in tubularised f laps/ grafts; success rate 20 per cent at two years post incision even with clean intermittent catheterisation), or by using a local/buccal graft.
Urethral diverticula
These bothersome, but not dangerous, complications were once more common from the widespread use of large inlay grafts. Patients might complain of a weak urinary stream, post-void dribbling, UTI, or haematuria (less common). However, the pathognomonic sign is ballooning of penile shaft during voiding/need to ‘milk’ residual urine from penile urethra. It is more common in boys undergoing preputial f lap repairs, two-stage repairs, and proximal repairs, and is thought to be related to a lack of spongiosal tissue in neourethra. Repairs involve excision of the diverticulum and closure over a catheter in two layers (Figure 3).

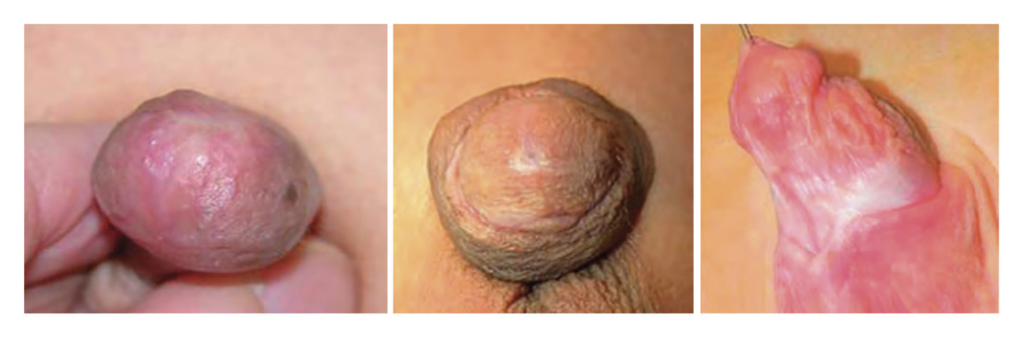
Balanitis xerotica obliterans
This autoimmune destructive condition, which is characterised as a chronic inflammatory dermatosis, is much more common in uncircumcised boys with phimosis and/or meatal stenosis, but can also present as a progressive urethral narrowing after hypospadias (Figure 4). The treatment for this is the use of topical steroids/systemic tacrolimus (if just meatus), but usually requires surgical excision. If this involves the urethra, it is important to excise all affected tissue and replace with buccal mucosa or inner prepuce.
(Recurrent) penile curvature
This presentation can have significant consequences for urinary and sexual function. This true incidence of this is unknown due to the limitations in research as described above, but is also a reason to advocate for hypospadias repair, as it does not spontaneously improve in conservatively-managed patients. This curvature may worsen as boys advance through puberty (potential differential growth of the dorsal and ventral portion of the corporal bodies). There are a number of approaches to repair this, which initially involve degloving of the penis and performing an artificial erection test. There are several methods published which claim to be able to correctly identify the degree of curvature over an ‘eyeball test’, with research having recently ventured into the realms of artificial intelligence (AI). Several procedures can be required to satisfactorily repair this, usually involving some degree of corporoplasty.
In a country like Ireland, it is incredulous that patients should be made wait for several years for all types of repair
EAU guidance
The EAU has updated a number of its general recommendations regarding the management of hypospadias (note that timing of repair remains unchanged):
- At birth, differentiate isolated hypospadias from disorders of sex development, which are mostly associated with cryptorchidism or micropenis.
- Counsel caregivers on functional indications for surgery, aesthetically feasible operative procedures (psychological, cosmetic indications), and possible complications.
- In children diagnosed with proximal hypospadias and a small-appearing penis, reduced glans circumference or reduced urethral plate, pre-operative hormonal androgen stimulation treatment is an option, but the body of evidence to accentuate its harms and benefits is inadequate.
- For distal hypospadias, offer Duplay-Thiersch urethroplasty, or tubularised incised plate urethroplasty. Use the onlay urethroplasty or two-stage procedures in more severe hypospadias. Correct significant (> 30 degrees) curvature of the penis.
- Ensure long-term follow-up to detect urethral stricture, voiding dysfunctions and recurrent penile curvature, ejaculation disorder, and to evaluate patient’s satisfaction.
- Use a validated objective scoring systems to assist in evaluating the functional and cosmetic outcomes.
In summary
Whilst the potential outcomes and complication rates are not insignificant with hypospadias repairs, the benefits of performing a repair (especially in proximal cases) appear to outweigh the risks. Informed consent is critical, and parents/ caregivers (and in some cases patients) need to understand that congenital phallic reconstruction is not a quick fix, and that several procedures may be required. It is important to be honest in terms of outcomes, and a second opinion should be offered in cases where there is some ambiguity as to the correct path. In a country like Ireland, it is incredulous that patients should be made wait for several years for all types of repair and if institutions cannot abide by international guidelines, then it is important for them to acknowledge this and seek outside help, rather than leave patients on waiting lists. One should not underestimate the psychological stress of a congenital genitourinary condition on families, creches, and schools. Finally, it is important to consider adopting an all-Ireland registry for these cases so that we better understand the aetiology, and outcomes for these vulnerable patients.








Leave a Reply
You must be logged in to post a comment.