NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Michelle, a 46-year-old female, underwent biopsy of a lesion in her left sided chest musculature in August 2022. Unfortunately, the lesion revealed a recurrence of breast cancer, which was first diagnosed in 2019. This new diagnosis was classified as oestrogen receptor positive and human epidermal growth factor receptor 2 (HER2) positive. The proposed oncology management was for surgical excision of the localised lesion, followed by aggressive treatment with chemotherapy, in turn followed by radiation and hormone therapy.
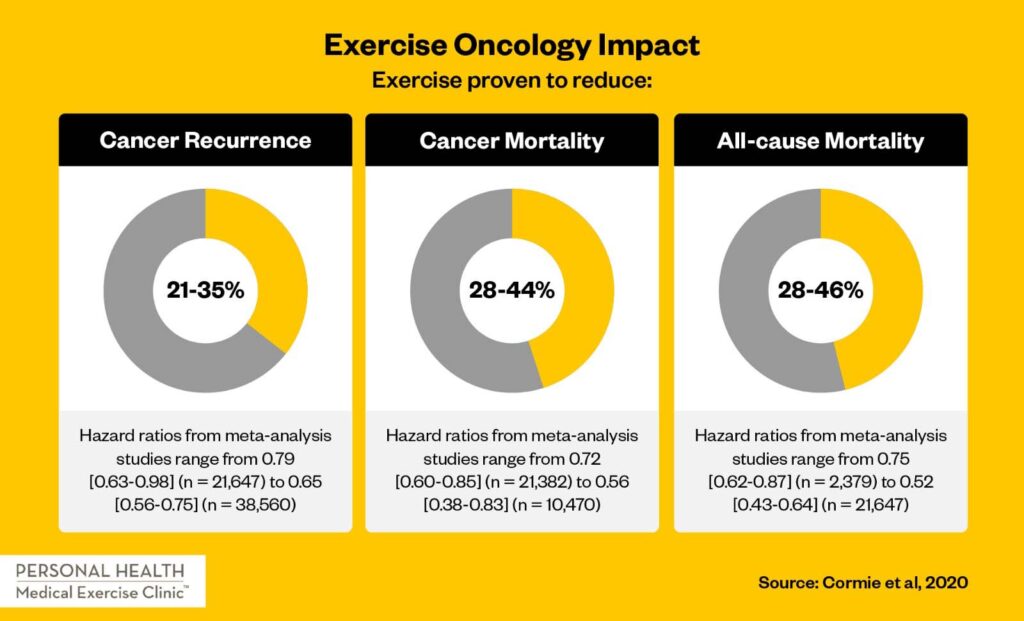
Michelle had her surgery in September 2022. This was followed by a 12-week programme of ACT chemotherapy (adriamycin, cyclophosphamide, taxol), a course of tamoxifen, and then radiation therapy. Michelle was referred for an exercise oncology programme by her surgeon in the pre surgical phase (which only lasted two weeks). The referral was primarily made in a bid to further reduce the percentage risk of cancer recurrence. Similarly, the intention was to mitigate some impactful side-effects throughout her oncology treatment plan.
Exercise testing
Given Michelle’s general exercise literacy and compliance, her familiarity with cancer treatment protocols/procedure, and great determination in the face of adversity, she chose to complete exercise testing only four days prior to her surgery date. On initial assessment, Michelle was screened via the American College of Sports Medicine (ACSM) risk stratification algorithm to gauge her suitability for maximal exercise testing. Her recent physical activity history was extensive, including a regularly used gym membership for small group classes supervised with a personal trainer, a daily walk with her dog, jogging at least twice per week (3-to-5km per jog) and being generally active as opposed to sedentary. She was formally exercising for more than 2.5 hours per week at varying levels of intensity including 50-to-60 minutes per week of vigorous activity. With no cardiology history and no current medications, she fulfilled the inclusion criteria for maximal exercise testing.
Assessment was performed in a clinical setting and included cardiorespiratory testing via gas analysis, body composition testing via bio-electrical impedance, isometric strength testing across relevant muscle groups and joints, mobility/flexibility assessment and neuromotor testing (an umbrella term for agility, power, co-ordination, and dynamic balance) via force plates.
Cardiorespiratory
Michelle’s cardiorespiratory function was assessed with a ‘Vo2max’ test via gas analysis. This test analyses the efficiency of the heart and lungs in transporting oxygen to peripheral tissues while under stress. The test was performed on a treadmill using the Bruce protocol, with oxygen saturation levels and heart rate monitored throughout. Blood pressure was taken pre- and post-exercise testing. The Borg scale of exertion was used to subjectively monitor Michelle’s exertion levels and appropriateness to continue or cease the maximal exertion testing.
Strength
Isometric strength testing was performed across relevant muscle groups and joints, alongside hand-grip dynamometry and a modified press-up test. Michelle’s previous cancer diagnosis and treatment had resulted in some self-reported weakness in left shoulder strength and range of motion. Bilateral shoulder rotation (internal and external), abduction, flexion, and extension were all identified as key measurements to ascertain the degree of shoulder dysfunction. Lower limb strength tests included bilateral hip flexion, knee extension, and ankle dorsiflexion.
Body composition
Body composition testing was performed via bio-electrical impedance. Key areas identified for assessment were bone mass, segmental lean muscle mass, body fat percentage, visceral fat, and basal metabolic rate (cardiorespiratory testing also provided a score in this area). Prior to exercise testing and recent diagnosis, a dual energy x-ray absorptiometry (DEXA) scan had already been performed to ascertain bone mineral density six weeks previously. Finally, waist to hip ratio was recorded via tape measure.
Mobility and flexibility
A key area for assessment was left-sided glenohumeral function. Bilateral shoulder range of motion was digitally assessed in external rotation, internal rotation, abduction, flexion, and extension. Scapular function was monitored via a functional movement pattern assessment. Lower back range of motion was also measured via a ‘sit and reach’ test.
Neuromotor
This testing was performed using force plates to digitally record lower limb movement quality. Asymmetry in terms of weight bearing and force production (during selected movements, eg, squat) was monitored.
Personalised exercise prescription
In clinical populations there are practical implications in designing a personalised exercise prescription. The exercise-specific barriers to entry for healthy populations are well documented (motivation, education, health literacy, access, resources, time constraints, supervision, etc). In clinical populations we also need to factor in presenting condition, physical activity history, medical history, medications, proposed treatment plan and side-effects, secondary complications, fear and avoidance, psychological wellbeing, quality-of-life, and more.
Therefore, the ideal exercise prescription is often aspirational and unattainable. Anecdotally, a key issue in the clinical setting is motivational interviewing. This helps to identify patient goals and a therapeutic alliance can be formed to help gradually achieve these goals over time. In exercise oncology, flexibility is a baseline requirement in terms of patient compliance, due to the myriad of treatment related side-effects. Notwithstanding, the medical oncology treatment plan is highly specific in terms of treatment dosage, frequency, intensity, time, and type of intervention. Therefore, exercise prescription ought to be similarly specific, with a view to building compliance and capability over time.
The American Society of Clincial Oncology (ASCO), ACSM and the American Heart Association contributed to roundtable publications on optimising exercise oncology interventions in 2019. The exercise prescription guidelines advise a minimum of 150 minutes of light-moderate activity, 75 cumulative minutes of vigorous activity and two strength/resistance training sessions per week across all major muscle groups. As always, there are special considerations, precautions, and contraindications, however, none of these applied to Michelle’s personalised programme. The testing data contributed to further specificity in her recommendations, including personalised target heart rate zones, targets for cardiorespiratory function, strength, and mobility based on normative age-related data. Supervision was recommended with the introduction of a strength training regime.
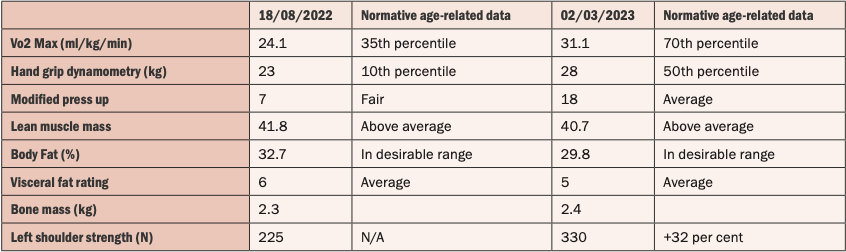
Table 1: Testing data plus retesting table of data
Intervention
During a treatment plan spanning over 28 weeks in total, Michelle was active in her exercise oncology programme for 24 of these 28 weeks. Treatment-related side-effects (in order of frequency and severity) included intermittent but severe fatigue, sleep disturbances, hot flushes, mouth ulcers and resultant lack of appetite, self-reported brain fog, low white cell count, and resultant antibiotics for bronchitis. She completed 16 in-clinic exercise sessions supervised by a chartered physiotherapist or exercise physiologist. These sessions focused on combination training of strength and cardiorespiratory function. She further completed 14 sessions with a personal trainer in her local gym, who helped to implement the recommended prescription.
Interpretation of results
The results were highly encouraging. There was a statistically-significant and noteworthy improvement in cardiorespiratory function. Given that the location of radiation therapy was in the upper left quadrant, there is an increased five-year risk (post-treatment) of cardio or pulmonary toxicity. Maintaining a high Vo2 max score is directly correlated with longevity and reduction in all-cause mortality across the general population.
However, in this clinical presentation, complications, such as treatment-related toxicity, are also mitigated by maintaining a high level of cardiorespiratory function. We believe that the significant improvement in cardiorespiratory fitness is partly related to regular bouts of small, but high-intensity interval training. However, these results may also be attributed to the improvements in upper and lower limb isometric strength testing. Stronger peripheral tissues are more efficient in their oxygen usage and consumption.
In terms of body composition, there was a decrease in total body fat percentage, and a small decrease in lean muscle mass. However, total weight loss being largely attributed to fat loss meant that the ratio of lean muscle to total body weight improved. In the presence of hormone therapy and early menopause, these scores are important and encouraging in terms of overall metabolic management. Similarly, a small increase in bone mass was detected. This may have been as a result of focused and consistent strength training.
Michelle had yet to undergo a repeat DEXA scan to ascertain changes in bone mineral density at the time of publication. Finally, a 32 per cent improvement in (external rotation) shoulder strength ensured Michelle was no longer guarding or avoiding shoulder usage in activities of daily living.
Discussion
With significant increases in funding and research over the last 10 years, oncology management is improving rapidly. Advances in drug development, pharmacological specificity, and personalised multidisciplinary care are having a positive impact on cancer survivorship. Exercise oncology is recommended as a key pillar in the standard of cancer care alongside surgery, radiotherapy, traditional chemotherapy, precision therapy, and immunotherapy. In terms of exercise oncology, the research is widespread and irrefutable in terms of its positive impact on treatment-related side-effects.
Further research is ongoing in the area of exercise impacting the systemic milieu of tumour cell biology and vascularisation. However, there is a translation gap from ‘bench to bedside’ as exercise oncology is still not a routine standard of care for all cancer patients. Aligned to the widespread evidence base, this case study is a small example which highlights compelling reasons for the inclusion of exercise oncology as standard of care.
References on request
Author: Andrew Dunne, Chartered Physiotherapist, Personal Health Medical Exercise Clinic, Dublin, www.personalhealth.ie












Leave a Reply
You must be logged in to post a comment.